NCCN 2024-2025
Clinical Pearls
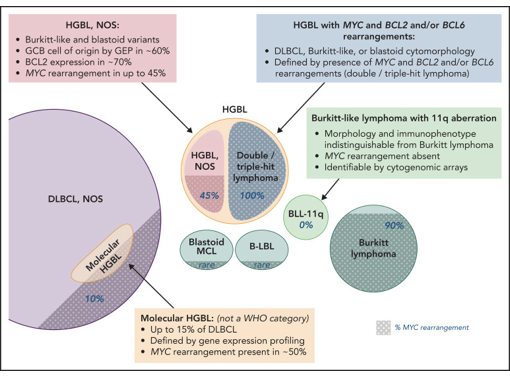
- HGBCL are aggressive lymphomas that do not fit neatly into DLBCL or BL categories (overlapping features) and often have poor prognosis, with frequent CNS involvement.
- Genomics (FISH for MYC, BCL2, BCL6). Majority are GCB-like lymphoma
- Double-Hit Lymphoma (DHL) (MYC + BCL2 and/or BCL6 rearrangements)
- Triple-Hit Lymphoma (THL) (MYC + BCL2 + BCL6 rearrangements)
- Translocation from indolent lymphomas (FL) to DHL is 2-3% annually, associated with poor prognosis.
- Initial Workup & Staging: LP/MRI for CNS involvement, echo/MUGA scan (if anthracycline planned), ID screening (HBV, HCV, HIV).
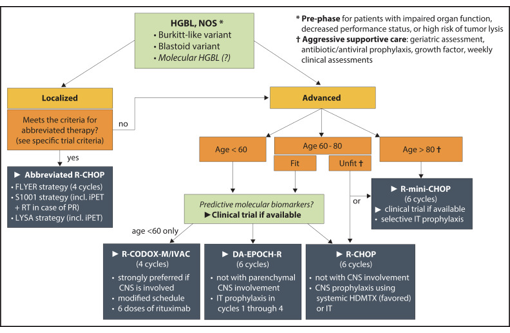
- Standard of care regimens is not yet established. Clinical trial is recommended in MYC/BCL2±BCL6 rearrangement and HGBL-NOS. R-CHOP showed inferior outcomes, could be considered in low-risk disease (IPI<2).
- HGBL with MYC+BCL2±BCL6: ISRT (localized disease), DA-EPOCH-R (preferred, better outcome vs R-CHOP), R-HyperCVAD,
R-CODOX-M/R-IVAC (for young, fit patients; BL), R-mini-CHOP (for elderly or frail).- Median PFS: DA-R-EPOCH (22mo) > R-HyperCVAD or R-CODOX-M/R-IVAC(19mo) > R-CHOP (12mo)
| DA-R-EPOCH Dosing Strategy (CVC line, 21d cycle) | ||||||||
| Levels | -2 (64%) | -1 (80%) | 1 (100%) | 2 (120%) | 3 (144%) | 4 (173%) | 5 (207%) | 6 (248%) |
| Etoposide (mg/m2/day) D1-4 | 50 | 50 | 50 | 60 | 72 | 86 | 104 | 124 |
| Doxorubicin (mg/m2/day) D1-4 | 10 | 10 | 10 | 12 | 14.4 | 17.3 | 20.7 | 24.8 |
| Cyclophosphamide (mg/m2/day) D5 | 480 | 600 | 750 | 900 | 1080 | 1296 | 1555 | 1866 |
| Rituximab 375mg/m2 IV on D1 (before others). Prednisone 60 mg/m² PO BID Days 1–5. Infusion over 96h (together): etoposide, doxorubicin, vincristine (0.4mg/m2/d, max 2mg/day) Requires G-CSF prophylaxis (filgrastim 5mcg/kg SC daily on D6+ until ANC >0.5 x109/L of nadir) Dose adjustments (ANC/platelet for etoposide, doxorubicin, cyclophosphamide on the next cycle) ANC: ≥0.5 (↑ 1 level), <0.5 for 1-2 times (same dose), <0.5 for ≥3 times (↓ 1 level)Platelet: <2.5 (↓ 1 level)CrCl: 15-50 (↓ etoposide 25%), 10 (↓ cyclophosphamide 25%, etoposide 50%)Bilirubin: 20-50 (↓ doxo 50%, vincr 25%, consider etop), 51-85 (↓ doxo 75%, vincr 50%, consider etop), >85 (omit doxo, etop)Peripheral neuropathy (motor): G2 (↓ vincr 25%), G3 (↓ vincr 50%), G4 (omit vincr)Peripheral neuropathy (sensory): G3 (↓ vincr 25%), G4 (omit vincr) | ||||||||
- Other considerations
- “Pre-phase” induction: steroids (low doses) ± chemotherapy (vincristine or cyclophos) to reduce fatal TLS risk.
- Consolidation with high-dose chemotherapy and auto-SCT rescue
- HGBL with MYC + BCL6: outcomes are similar to DLBCL-NOS, treat with DA-EPOCH-R.
- HGBCL-NOS (CD20+, EBER2-, CD30+, CD15+): blastoid, or intermediate between DLBCL and BL, may lack MYC/BCL2/BCL6 rearrangement. Poor prognosis (high LDH, bone marrow and CNS involvement, high IPI)
- Clinical trial is recommended
- R-CHOP (if DLBCL-like features), Pola-R-CHP (category 2B), R-mini-CHOP (if elderly, frail), DA-EPOCH-R or R-HyperCVAD or R-CODOX-M/R-IVAC (if aggressive features like Burkitt-like, very high Ki-67, CD10 positivity),
- CNS Prophylaxis if High Risk (IT Methotrexate).
- Relapsed/Refractory (R/R): managed per R/R DLBCL. HGBCL has a high relapse rate, so aggressive salvage therapy is needed:
- If <12mo and CAR-T cell eligible: Yescarta (axi-cel, Category 1), Breyanzi (liso-cel, Category 1)
- Bridging therapy: platinum-based chemo (DHAP±R, GDP±R, ICE±R, GemOx±R), PV±Bendamustine±Rituximab, ±ISRT
- TRASCEND NHL 001 (Breyanzi) showed ORR 73%, CR 53%, PFS 44%, OS 58%
- If <12mo and CAR-T cell ineligible (preferred): BiTE (Epcoritamab + GemOx, Glofitamab + GemOx), PV±Bendamustine±Rituximab, PV+Mosunetuzumab, Tafasitamab+Lenalidomide (not in refractory primary)
- Other options: CEOP±R, DHAP±R, ESHAP±R, GDP±R, ICE±R, GemOx (if BiTE ineligible), MINE±R, BV (if CD30+), ibrutinib (non-GCB DLBCL), R2 (non-GCB DLBCL)
- EPCORE NHL-1 (Epcoritamab-bysp) showed ORR 61% (CR 38%), median DOR 15.6mo.
- NP30179 (Glofitamab-gxbm) showed ORR 56% (CR 43%), DOR 18.4 months, median time to response 42 days.
- If >12mo and ASCT eligible: platinum-based chemo (DHAP±R, GDP±R, ICE±R, ESHAP±R, GemOx±R), MINE±R
- If >12mo and ASCT ineligible: CAR-T (Breyanzi if eligible), BiTE [Epcoritamab+GemOx, Glofitamab+GemOx (category 1)], PV±Bendamustine±Rituximab, PV+Mosunetuzumab, Tafasitamab+Lenalidomide
- Other options: CEOP±R, GDP±R, GemOx (if BiTE ineligible), Rituximab monotherapy, BV (if CD30+), ibrutinib (non-GCB DLBCL), R2 (non-GCB DLBCL)
- If <12mo and CAR-T cell eligible: Yescarta (axi-cel, Category 1), Breyanzi (liso-cel, Category 1)
- CNS Prophylaxis Required
- CNS-IPI (need for CNS prophylaxis): age >60yo, stage III-IV, ECOG ≥2, LDH > ULN, ≥2 extranodal site, kidney and adrenal involvement. High risk (4-6, kidney/adrenal involvement) shows 2-year CNS relapse of ~10%.
- Independent risk factors: Testicular lymphoma, primary cutaneous DLBCL (leg type), breast DLBCL (stage IE), kidney or adrenal gland involvement, uterine (not ovarian), paranasal or parameningeal, orbital, bone-marrow, high-grade lymphoma, HIV-associated lymphoma, ABC cell of origin.
- CNS prophylaxis:
- Leptomeningeal (BL): IT MTX/Cytarabine (4-8 doses). May consider Ommaya reservoir placement, systemic MTX.
- Parenchymal (HGBL, DLBCL): Systemic HD-MTX (3–3.5 g/m2 x2–4 cycles; D15 of 21-day cycle) + G-CSF.
- CNS-IPI (need for CNS prophylaxis): age >60yo, stage III-IV, ECOG ≥2, LDH > ULN, ≥2 extranodal site, kidney and adrenal involvement. High risk (4-6, kidney/adrenal involvement) shows 2-year CNS relapse of ~10%.
- Supportive Care Considerations for Oncology Pharmacists
- Infusion-reaction (Rituximab, Tafasitamab): APAP + diphenhydramine ± steroids + H1/H2 blocker (with Tafasitamab only)
- Febrile Neutropenia ppx (DA-R-EPOCH, age≥65): G-CSF (filgrastim 5mcg/kg SC daily D6+ until ANC >0.5 x109/L of nadir). Use broad-spectrum antibiotics if febrile.
- TLS Prophylaxis (high risk due to rapid cell turnover, bulky, PV): Allopurinol 100 mg/m2/dose q8h upto 300-800mg/day (intermediate risk) or Rasburicase 0.2mg/kg/day (or flat dose 3-7.5 mg – 6mg) upto 5 days (high risk).
- Cardiotoxicity (Doxorubicin): monitor LVEF by ECHO/MUGA at baseline, then when needed. Use DA-R-EPOCH (if LVEF >35%),
R-CEOP (if anthracycline is contraindicated).
- Neuropathy (Vincristine, Cisplatin, Oxaliplatin, Brentuximab vedotin, Polatuzumab vedotin): dose reduction/interruption if severe. Gabapentin 300mg/day (adjust dose per response)
- Cold-induced neuropathy (Oxaliplatin): Avoid cold exposure for 7-10d after dose
- Nephrotoxicity/hemorrhagic cystitis (Cyclophosphamide, Ifosfamide, MTX): aggressive hydratin, mesna (Ifosfamide, cyclophos >1200mg/m2)
- Pulmonary toxicity (Carmustine): PFT at baseline, then as needed
- Conjunctivitis ppx (Cytarabine systemic): prednisolone 1% 2 drops to each eye 4 times daily during first day, until 24-72h post-completion.
- CRS (Mosunetuzumab-axqb) at C1-2, C3+ is optional: APAP, dexamethasone, diphenhydramine.
- CRS (Epcoritamab, Glofitamab, CAR T): Obinutuzumab 1g IV (7d prior Glofitamab as CRS mitigation); premeds of APAP, diphenhydramine, dexamethasone (Epcoritamab, Glofitamab, CAR T-cell therapy)
- Anticoagulation prophylaxis (Lenalidomide)
- HBV/HCV reactivation (Rituximab): screen at baseline, treat when needed. Entecavir or Tenofovir ppx if receiving rituximab.
- PJP Prophylaxis (Bendamustine, prolonged steroids): TMP-SMX or Dapsone.
- HSV ppx (Bendamustine, prolonged steroids): acyclovir 400mg PO BID; Acyclovir/Valacyclovir in rituximab-regimen.
- REMS: CAR-T (CRS/ICANS), Lenalidomide (fetal-embryonic toxicity)
| Regimens | Medications |
| DA-R-EPOCH | Dose-Adjusted Rituximab, Etoposide, Prednisone, vincristine (Oncovin), Cyclophosphamide, doxorubicin (Hydroxydaunorubicin) |
| R-HyperCVAD | Rituximab, Hyperfractionated (smaller doses but more frequent), Cyclophosphamide, Vincristine, doxorubicin (Adriamycin), Dexamethasone Alternating with rituximab, high-dose methotrexate and cytarabine |
| R-CODOX-M/R-IVAC | Rituximab, Cyclophosphamide, vincristine (Oncovin), DOXorubicin, Methotrexate (high-dose) Alternating with rituximab, ifosfamide, etoposide, cytarabine |
| R-mini-CHOP (for elderly and frail) | Rituximab 375 mg/m² D1, Cyclophosphamide 400 mg/m² D1, Doxorubicin 25 mg/m² D1 (Hydroxydaunorubicin), Vincristine 1 mg D1 (Oncovin), Prednisone 40 mg/m² D1–5 |
| R-CHOP | Rituximab, Cyclophosphamide, doxorubicin (Hydroxydaunorubicin), vincristine (Oncovin), Prednisone |
| Pola-R-CHP (if IPI≥2) | Polatuzumab vedotin, Rituximab, Cyclophosphamide, doxorubicin (Hydroxydaunorubicin), Prednisone |
| R-DHAP | Rituximab, Dexamethasone, cytarabine (High-dose Ara-C), Platinum (carboplatin, cisplatin, oxaliplatin) |
| R-GDP | Rituximab, Gemcitabine, Dexamethasone, Platinum (carboplatin, cisplatin) |
| R-ICE | Rituximab, Ifosfamide, Carboplatin, Etoposide |
| R-ESHAP | Rituximab, Etoposide, methylprednisolone (Solu-Medrol), cytarabine (High-dose Ara-C), Platinum (cisplatin) |
| R-CEOP | Rituximab, Cyclophosphamide, Etoposide, vincristine (Oncovin), Prednisone |
| R-MINE | Rituximab, Mesna (uroprotectant, supportive), Ifosfamide, mitoxaNtrone, Etoposide |
| GemOx | Gemcitabine, Oxaliplatin |
| BEAM | Carmustine (BICNU), Etoposide, Cytarabine (Ara-C), Melphalan |
| R2 | Lenalidomide (Revlimid), Rituximab |