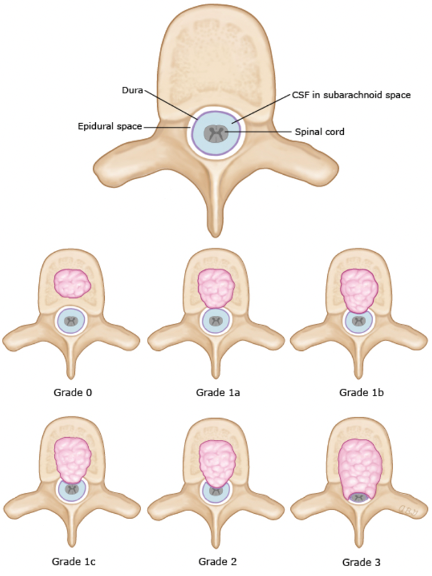
Malignant spinal cord compression (MSCC) is a compression of dural sac/spinal cord/cauda equina by extradural tumor. It is considered an oncologic emergency, and a delay in treatment can cause irreversible paralysis.
Incidence: Occurs in 5-10% of cancer patients. First symptom of cancer in 20-34%.
- Location: Thoracic (70%) > Lumbar (20%) > Cervical (10%).
Signs and symptoms include back pain (80-95%), radiculopathy, motor weakness, sensory deficits, sphincter incontinence (loss of bowel and bladder function), autonomic dysfunction, paresthesia (pins/needles).
Diagnosis: MRI with contrast (entire spine; detects compression & evaluates multiple levels). CT myelography (if MRI is CI like pacemaker). Plain X-rays are NOT reliable as they miss early-stage compression.
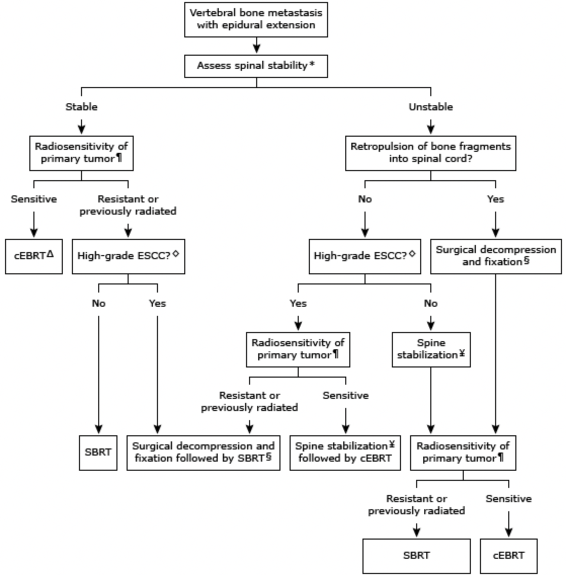
Treatment consists of dexamethasone and radiation therapy or surgery.
Goals: Relieve pain, preserve/improve neurologic function, local tumor control, stabilize spine. Preservation or improvement of neurologic function and spinal mechanical stability utilizing treatments appropriate to the patient’s burden of disease, life expectancy, values and preferences, and goals for care
Radiation
Management
| Treatment | Indication | Dosing | Clinical Pearl |
| Dexamethasone (IV → PO) | ALL SCC patients | 10 mg IV → 16 mg/day PO | Taper after definitive therapy starts |
| Dexamethasone (high dose) | Severe deficits | 96 mg IV → 24 mg q6h ×3d | Higher toxicity; no clear benefit |
| Opioids (Morphine, Fentanyl, Hydromorphone) | Severe pain | As needed | Adjust for renal/hepatic impairment |
| RT (cEBRT 20–30 Gy) | Radiosensitive tumors | 5–10 fractions | Standard for SCC without instability |
| SBRT (24–30 Gy/1–3 fractions) | Post-op, radioresistant tumors | 1–3 fractions | Higher precision, better tumor control |
| Surgical Decompression | Instability, failure of RT | Case-by-case | Separation surgery + SBRT preferred |
| VTE Prophylaxis (LMWH, UFH, Fondaparinux) | Immobile patients | Standard doses | Hold pre-surgery |
General management
- Dexamethasone is the steroid of choice – rapid onset, potent anti-inflammatory action.
- Taper steroids gradually to prevent adrenal insufficiency.
- Pain relief often requires opioids & neuropathic agents (gabapentin, duloxetine).
- Monitor for steroid side effects: GI bleeding (PPI co-administration recommended), hyperglycemia, insomnia, psychosis.
- For patients on long-term steroids, consider prophylaxis against PJP (TMP-SMX 160/800 mg PO TIW).
- Radiotherapy is the backbone of SCC treatment but is less effective for radioresistant tumors.
- Surgical decompression is critical for unstable spines, radioresistant tumors, or failure of RT.
- Prophylactic anticoagulation is essential for immobile patients unless contraindicated.
Immediate Management (Before Definitive Therapy)
High-Dose Dexamethasone (Anti-inflammatory & Edema Reduction)
- Mechanism: Reduces vasogenic edema. May temporarily treat cancer (e.g., MM).
- Indication: ALL symptomatic patients with SCC (immediate administration)
- Dosing:
- Dexamethasone 16 mg/day (moderate-dose) to 96 mg/day (high-dose) divided QID. Most clinicians use 4-10 mg PO or IV every 6 hours. Higher doses for profound/rapidly progressive neurologic demise.
- Standard dose: Dexamethasone 10 mg IV, then 16 mg/day PO (divided doses)
- Mild cases (minimal deficits, early-stage compression): Consider lower doses (4–8 mg IV BID)
- Severe neurologic deficits (paraparesis/paraplegia): Dexamethasone 96 mg IV LD, then 24 mg q6h ×3d, f/b a 10-day taper
- Clinical Pearls:
- Start BEFORE imaging confirmation if SCC is highly suspected.
- Taper once definitive therapy (radiation/surgery) starts to prevent steroid toxicity.
- High-dose regimens do NOT improve long-term outcomes & increase risk of gastric ulcers, psychosis, and infections.
Pain Management
- Opioids (morphine, hydromorphone, fentanyl) are first-line
- Neuropathic pain: Consider gabapentinoids (pregabalin, gabapentin) or duloxetine
Venous Thromboembolism (VTE) Prophylaxis
- Indication: ALL immobile SCC patients (unless contraindicated)
- Anticoagulants: LMWH (Enoxaparin 40 mg SC daily), UFH 5,000 units SC q8-12h, Fondaparinux 2.5 mg SC daily
- Hold if surgery is planned within 24 hours
- If anticoagulation contraindicated → Use mechanical compression (SCDs, stockings)
Definitive Treatment Options
Radiation Therapy (RT)
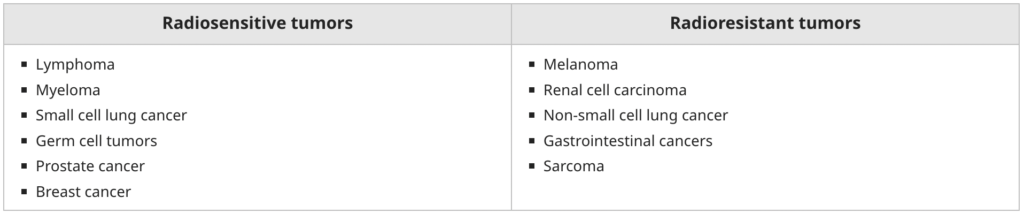
- Radiation Therapy: Most frequently offered. For radiosensitive tumors (lymphoma, breast, MM, SCLC, seminoma, neuroblastoma, Ewing sarcoma), expected survival <3 months, unable to tolerate surgery, total neurological deficit for >24 hours, multilevel/diffuse spinal involvement.
- Indication: SCC from radiosensitive tumors (lymphomas, myeloma, small cell lung cancer, prostate cancer)
- Preferred Approach:
- Conventional external beam radiation therapy (cEBRT) 20–30 Gy in 5–10 fractions
- Stereotactic body RT (SBRT) 24–30 Gy in 1–3 fractions (for oligometastatic or post-surgery cases). SBRT preferred for:
- Post-surgical patients (separation surgery)
- Previously irradiated patients
- Radioresistant tumors (e.g., renal cell carcinoma, melanoma, sarcoma)
Surgery (Spinal Decompression & Stabilization)
- Indication: Considered if >3 months life expectancy and <24 hours of paraplegia. Preferred for specific cases (spinal instability, radioresistant tumors, rapid deterioration, previous radiation, single site compression, etc.).
- Spinal instability, radioresistant tumor (renal cell, melanoma, sarcoma), progression despite RT, pathologic vertebral fracture
- Preferred Approach: Separation surgery + Post-op SBRT (less invasive, lower risk of surgical morbidity; avoids extensive vertebrectomy)
Supportive Care Considerations
Urinary Retention & Bowel Dysfunction
- Bladder scanning for retention
- Foley catheter placement if retention present
- Prophylactic bowel regimen (due to steroids & immobility)
- First-line: Stimulant laxatives (senna, bisacodyl) + stool softeners (docusate)
- Avoid bulk-forming agents (e.g., psyllium) due to risk of impaction
- Opioid-induced constipation: Consider methylnaltrexone