Serological Markers
| Marker | Lab Results and Interpretation | Notes |
|---|---|---|
| Hepatitis B surface antigen (HBsAg) | Positive: Chronic or acute infection | Hallmark of infection in screening and disease. If positive for >6 months → chronic infection |
| Hepatitis B surface antibody (anti-HBs or HBsAb) | Positive: Immune (via vaccine or past infection); >10 IU/mL is protective | Appears after clearance of HBsAg or post-vaccine. Not present in chronic infection |
| Hepatitis B core antibody (anti-HBc or HBcAb) | Positive: Previous or current infection (Exposure to HBV) | Not present after vaccination (only shows natural infection; IgM acute infection) |
| IgM antibody to HBV core (IgM anti-HBc) | Positive: Acute or recent infection | Detects infection in the “window period” |
| IgG antibody to HBV core (IgG anti-HBc) | Positive: Past or chronic infection | Persists for life; not protective |
| Hepatitis B envelope antigen (HBeAg) | Positive: active viral replication, high infectivity | If positive, patient is highly infectious |
| Antibody to envelope antigen (anti-HBe) | Positive: Lower infectivity, seroconversion | Sign of improving immune control or response to therapy |
| HBV viral load (HBV DNA via PCR) 5 copies = 1 IU | Negative, lowly elevated (<100 IU/mL) Slightly elevated (≥100, <2000 IU/mL) Moderately elevated (≥2000, <20000 IU/mL) Highly elevated (≥20000 IU/mL) | Used to guide treatment decisions |
Common Clinical Scenarios
| Status | HBsAg | anti-HBs | anti-HBc (IgG) | HBV DNA | Interpretation |
|---|---|---|---|---|---|
| Vaccinated | Negative | Positive | Negative | Negative | Immune via vaccination |
| Acute Infection | Positive | Negative | Positive (IgM) | High | Early infection |
| Chronic Infection | Positive | Negative | Positive (IgG) | High or low | Chronic HBV |
| Resolved Infection | Negative | Positive | Positive (IgG) | Negative | Past exposure, immune |
| Window Period | Negative | Negative | Positive (IgM) | Usually low | Early acute infection |
| Immune tolerant phase | Positive | Negative | Positive | High | Common in young chronic carriers |
| Inactive carrier | Positive | Negative | Positive | Low or undetectable | Chronic infection with low replication |
If HBc+ but sAg−, HBs−: intermediate-high risk (exposed but low HBs, still at risk for HCC), false positive, acute HBV (test HBc IgM, HBV DNA).
Risk of HBV reactivation
| Very high risk (>20%) | HBsAg+ | Anti-CD20 (Rituximab, Ofatumumab, Obinutuzumab), HCT |
| High risk (11-20%) | HBsAg+ | High-dose glucocorticoids (≥20 mg/day prednisone ≥4 weeks), anti-CD52 (alemtuzumab) |
| Moderate risk (1-10%) | HBsAg+ | Chemo (no steroids), anti-TNF, solid organ txp rejection therapy; doxorubicin, TKI (imatinib, ibrutinib) |
| Moderate risk (1-10%) | HBsAg− and HBc+ | Anti-CD20 or HCT |
| Low risk (<1%) | HBsAg+ | MTX or AZA |
| Low risk (<1%) | HBsAg− and HBc+ | High-dose glucocorticoids (≥20 mg/day) or anti-CD52 (alemtuzumab) |
| Very low risk (rare) | HBsAg− and HBc+ | Chemo (no steroids), anti-TNF therapy, MTX, AZA |
| Uncertain risk | HBsAg− and HBc+ | Type of immunosuppressive therapy in solid organ txp, ICI (nivolumab, pembrolizumab) |
Anticancer causative agent (distribute to above table [look into articles]): proteasome inhibitors (Bortezomib, Carfilzomib, Ixazomib), BTKi (Ibrutinib, Acalabrutinib, Zanubrutinib, Pirtobrutinib), BCR::ABLi (Imatinib, Dasatinib, Nilotinib, Bosutinib, PONATinib, Asciminib), mTOR (Everolimus, Sirolimus, Temsirolimus), HDACi (Belinostat, Panobinostat, Romidepsin, Vorinostat), JAKi (Momelotinib, Ruxolitinib, Fedratinib, Pacritinib)
HBV Prophylaxis
Recommendations: Screen all patients (HBsAg, anti-HBs, anti-HBc) ≥1-2 weeks before anticancer. If any is positive, test HBV DNA.
| Serology | Interpretation | Recommendations |
|---|---|---|
| HBsAg+ | Chronic HBV | Start antiviral prophylaxis (entecavir, tenofovir) 7 days before and 6-12 months after anti-cancer |
| HBsAg−, anti-HBc+ | Resolved infection (risk varies) | If high-risk therapy (rituximab): consider prophylaxis or close HBV DNA monitoring every 1–3 months |
| HBsAg−, anti-HBc− | No infection | No action unless vaccinated |
Duration of Antiviral Prophylaxis
- Start ≥1 week before immunosuppressive therapies.
- Continue antiviral prophylaxis for ≥6–12 months after completion of anticancer (some recommend up to 12–18 months for high-risk regimens like rituximab).
- Monitor ALT and HBV DNA regularly during and after treatment.
Monitoring: ALT/DNA every 3 months, HBeAg/anti-HBe every 6 months, HCC every 6 months
Monitoring parameters if treatment is not considered in HBeAg+, HBV DNA >20,000 IU/mL, normal ALT (ALT, HBeAg)
- ALT every 3-6 months, HBeAg every 6-12 months.
- If ALT levels increase 1-2x ULN (35-70 U/L for men, >25-50 U/L for women):
- Recheck ALT every 1-3 months, HBeAg every 6 months.
- Assess liver fibrosis (biopsy or noninvasive) if ALT remains high and patient is >40 yrs or has FHx of HCC. Treat if moderate-severe inflammation or fibrosis (METAVIR score ≥F2).
- If ALT >2x ULN for 3–6 months, HBeAg+, HBV DNA >20,000 IU/mL: start treatment.
- HCC screening if at risk.
Monitoring parameters if treatment is not considered in HBeAg-, HBV DNA <2,000 IU/mL, normal ALT (ALT, HBV DNA)
- ALT and HBV DNA every 3 months for 1 year. If persistently normal, then every 6–12 months (or ALT alone if cost is a concern).
- If ALT levels increase 1–2x ULN (35-70 U/L for men, >25-50 U/L for women):
- Check HBV DNA and rule out other causes of liver disease.
- Monitor ALT and HBV DNA every 3 months.
- Assess liver fibrosis (biopsy or noninvasive) if ALT or HBV DNA (≥2,000 IU/mL) remains high. Treat if moderate-severe inflammation or fibrosis (METAVIR score ≥F2).
- If ALT levels increase >2x ULN and HBV DNA >2,000 IU/mL: treat.
- If ALT <2x ULN if and HBV DNA >2,000 IU/mL: assess fibrosis (biopsy or noninvasive). Treat if moderate-severe inflammation or fibrosis (METAVIR score ≥F2).
- HCC screening if at risk.
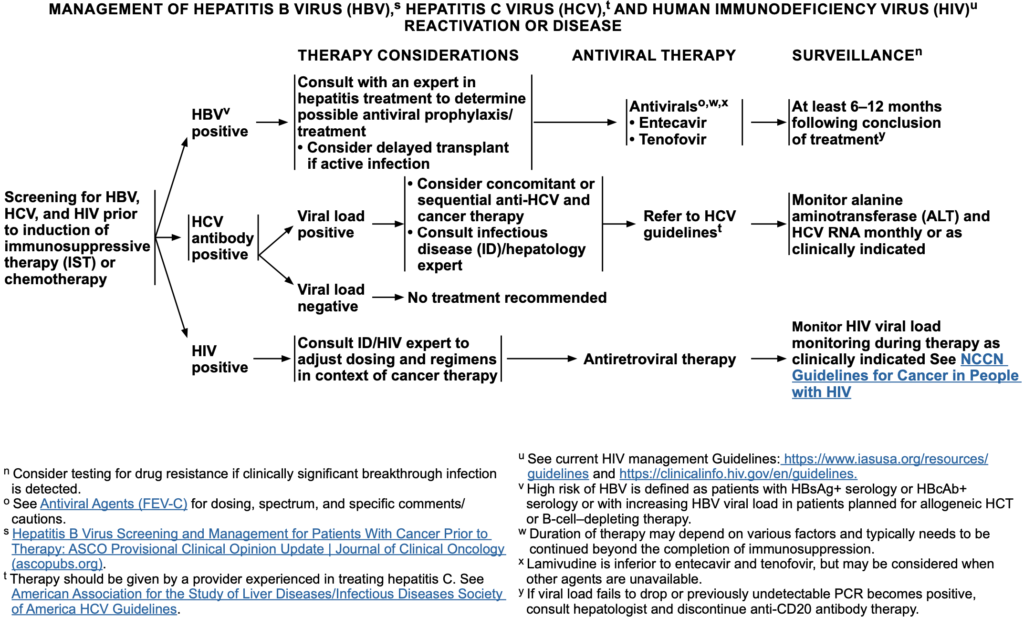
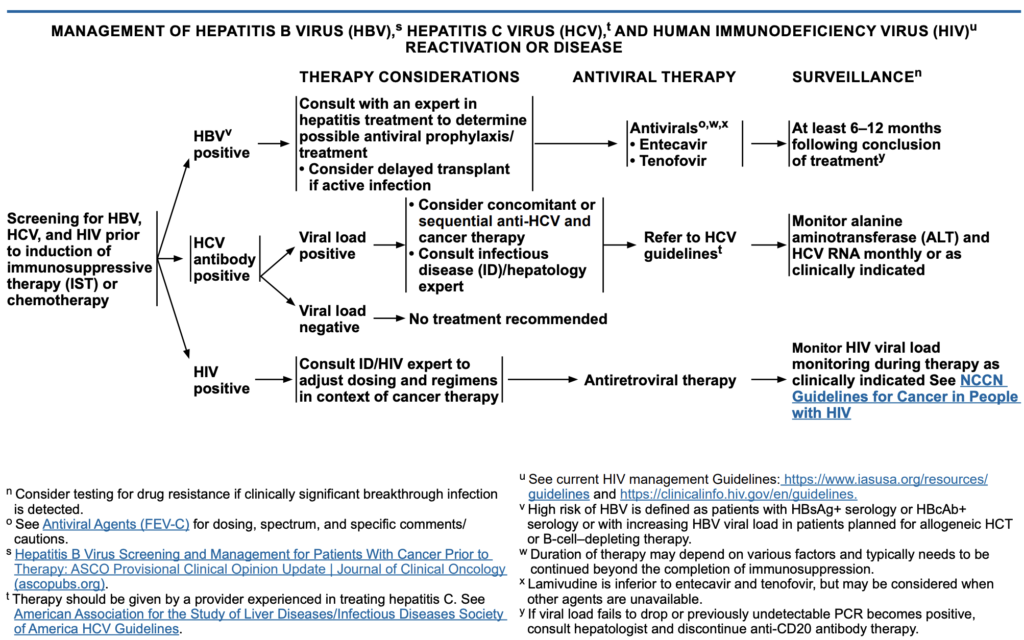
HBV Treatment
If HBV DNA is elevated (active viral replication) regardless of symptoms
- Delay cancer therapy briefly (if possible) to initiate antiviral therapy and reduce viral load (especially in high HBV DNA levels >2,000 IU/mL)
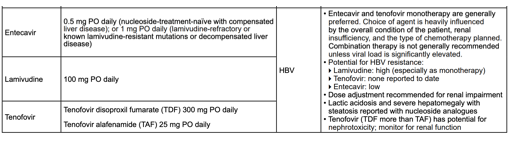
- Start Antiviral Therapy Immediately: Entecavir or Tenofovir alafenamide (TAF) or Tenofovir disoproxil fumarate (TDF). These are first line, potent and have a high barrier to resistance. Avoid lamivudine monotherapy due to resistance risk.
- Coordinate with Hepatology/Infectious Disease, especially if ALT is elevated or HBV DNA is very high (>20,000 IU/mL)
- Continue antiviral therapy throughout cancer therapy, and for ≥12 months after last rituximab dose. Some experts recommend up to 18 months in high-risk regimens
- Monitor: HBV DNA and ALT every 1–3 months. Watch for flare-ups (ALT spikes) or virologic rebound
| Medication | Class | ADE and Clinical Pearls |
|---|---|---|
| Entecavir PO | Nucleoside analog (guanosine) | Preferred in renal impairment, HBsAg+ receiving immunosuppressive cancer therapy Dosing: 0.5 mg/day (renal dosing if CrCl <50); oral solution is recommended if dose <0.5mg; 1mg in decompensated liver disease, previous lamivudine treatment, or suspected 3TC-resistance. Take on empty stomach (≥2h before/after food) ADE (well tolerated): lactic acidosis (rare, in advanced liver disease), HA, fatigue, nasuea Risk of resistance if prior lamivudine exposure, avoid in lamuvidine-resistance (50% resistance in up to 5 years) |
| Tenofovir alafenamide PO (TAF) | Nucleotide analog (NRTI, adenosine) | TAF (intracellular delivery, less systemic levels) is preferred over TDF (nephrotoxic, osteoporosis) but similar potency (potent HBV suppression). Preferred in renal impairment, osteoporosis risk, older adults Dosing: TAF 25 mg/day (renal dosing if CrCl <15) ADE (more tolerated vs TDF): less nephrotoxic, BMD loss; mild GI symptoms. $$$, availability issues. |
| Tenofovir disoproxil fumarate PO (TDF) | Nucleotide analog (NRTI, adenosine) | TAF is preferred over TDF (nephrotoxic, osteoporosis) but similar potency (potent HBV suppression). Preferred in HIV coinfection, normal renal function, no bone disease. Dosing: TDF 300 mg/day (renal dosing if CrCl <50) ADE: nephrotoxicity (↑ SCr, ↓ phosphate), BMD loss, GI upset, headache Monitor: renal function & electrolytes |
NCCN B-cell lymphoma Guideline
Hepatitis B virus (HBV):
- Anti-CD20 mAb-based chemoimmunotherapy is associated with risk of HBV reactivation. Hepatitis B surface antigen (HBsAg) and hepatitis B core antibody (HBcAb) testing for all patients receiving anti-CD20 mAb therapy
- Quantitative hepatitis B viral load by PCR and surface antibody only if one of the screening tests is positive
- Note: Patients receiving IV immunoglobulin (IVIG) may be HBcAbpositive as a consequence of IVIG therapy.
- Prophylactic antiviral therapy with entecavir is recommended for any patient who is HBsAg-positive and receiving anti-lymphoma therapy. If there is active disease (PCR+), it is considered treatment/management and not prophylactic therapy. In cases of HBcAb positivity, prophylactic antiviral therapy is preferred; however, if there is a concurrent high-level hepatitis B surface antibody, these patients may be monitored with serial hepatitis B viral load.
- Entecavir is preferredb
- Avoid lamivudine due to risks of resistance development.
- Other antivirals including adefovir, telbivudine, and tenofovir are proven active treatments and are acceptable alternatives.
- Monitor hepatitis B viral load with PCR monthly through treatment and every 3 months thereafter.
- ◊ If viral load is consistently undetectable, treatment is considered prophylactic.
- ◊ If viral load fails to drop or previously undetectable PCR becomes positive, consult hepatologist and discontinue antiCD20 mAb therapy.
- Maintain prophylaxis up to 12 months after oncologic treatment ends
- ◊ Consult with hepatologist for duration of therapy in patient with active HBV.
NCCN ID Guideline
The risk factors for HBV infection include personal or parental history of an intermediate to high prevalence of HBV infection in one’s birthplace (defined as a prevalence of hepatitis B surface antigen [HBsAg] positivity in >2% of the population); household and sexual contact with HBsAg+ persons; individuals with multiple sexual partners or history of sexually transmitted diseases; individuals who have been inmates of correctional facilities; patients with chronically elevated AST or ALT levels; patients with a history of injection drug use; males who have sex with other males (MSM); and patients positive for HCV or HIV.
A positive HBsAg is associated with active infection or a window period before the development of protective immunity in patients exposed to HBV. An individual who has been vaccinated for HBV typically has the following serology: negative HBsAg, positive hepatitis B surface antibody (HBsAb), and negative hepatitis B core antibody (HBcAb). False-negative HBsAg results may occur in patients with chronic liver disease. HBsAb positivity is generally equated with protective immunity, although reactivated HBV disease may occur in the setting of significant immunosuppression in individuals who are HBcAb-positive. A patient with resolved hepatitis B infection will be HBcAb positive but HBsAg negative. As mentioned above, some patients with cancer are at increased risk for HBV reactivation due to profound immunosuppression stemming from cytotoxic regimens, high-dose corticosteroids, tyrosine kinase inhibitors, anti-CD20/CD52 monoclonal antibodies, and/or the underlying malignancy (eg, leukemia, lymphoma). Patients with malignancies who are HBsAg positive and/or HBcAb positive are at risk for HBV reactivation with cytotoxic chemotherapy. Approximately 20% to 50% of patients with HBsAg positivity and 3% to 45% with HBcAb positivity develop HBV reactivation. The risk of HBV reactivation for patients who are HBsAg negative, HBcAb positive varies widely based on the virological profile, disease, and immunosuppressive regimen. Serum HBV DNA testing prior to the initiation of therapy may help define their risk of reactivation. If viremic, they may receive similar prophylaxis as patients who are HBsAg positive. Complications of HBV reactivation can range from self-limited hepatitis to fulminant hepatic failure and death. HBV reactivation can lead to early discontinuation or delayed initiation of treatment. A systematic review and meta-analysis by Zhang et al revealed that patients with B-cell non-Hodgkin lymphoma (NHL) who are HBsAg+ had worse prognosis and higher incidence of hepatic dysfunction during chemotherapy. In a meta-analysis and evaluation of the U.S. Food and Drug Administration (FDA) safety reports, it was reported that HBcAb positivity correlated with increased incidence of rituximab-associated HBV reactivation. After allogeneic HCT, loss of HBV-specific immunity may occur (ie, loss of HBsAb and development of HBsAg and HBV PCR positivity). This has been observed in up to 40% of susceptible individuals in one report and may be confused with hepatic GVHD. A retrospective study showed that allogeneic HCT recipients who were HBsAg negative but HBcAb positive had a high risk of seroconversion to HBsAg positivity and HBV reactivation (subsequently leading to hepatitis) following allogeneic HCT.
There are several nucleos(t)ide analogs approved by the FDA for the prevention and treatment of HBV. Historically, data supporting the use of these analogues have been based on lamivudine, a reverse transcriptase inhibitor. In a meta-analysis of clinical trials evaluating lamivudine prophylaxis in patients with HBsAg-positive lymphoma treated with IST, prophylaxis resulted in a significant reduction in HBV reactivation (risk ratio, 0.21; 95% CI, 0.13–0.35) and a trend for reduced HBV-related deaths (risk ratio, 0.68; 95% CI, 0.19–2.49) compared with no prophylaxis. However, despite its initial effectiveness, virologic breakthrough was high, with reports of resistance in 80% of patients after 5 years of therapy. Thus, lamivudine monotherapy has fallen out of favor. Studies suggest one of the newer agents (such as entecavir or tenofovir) may be preferable or combination therapy may have a possible role for patients with lamivudine-resistant HBV infections.
As of 2015, tenofovir is available in two different pro-drug forms, tenofovir disoproxil fumarate (DF) and tenofovir alafenamide (AF). Tenofovir AF has greater plasma stability than tenofovir DF, allowing use of a lower dose and lesser systemic exposure to the drug. Tenofovir DF has demonstrated superior antiviral efficacy compared with adefovir in a phase III randomized double-blind study in patients with chronic HBV infection, making tenofovir preferred over adefovir in this setting. Two randomized, phase III, double-blind studies comparing tenofovir AF to tenofovir DF in patients with HBeAg-negative or HBeAg-positive chronic HBV infection showed that the efficacy of tenofovir AF was non-inferior to tenofovir DF, with better bone and renal safety for tenofovir AF. While these data support the use of tenofovir for HBV infection, limited data are available regarding its use in patient populations with cancer. A systematic review and meta-analysis showed that in patients with HBV-associated hepatocellular carcinoma (HCC), tenofovir was associated with better overall survival and reduced late recurrence compared to entecavir. No detectable resistance to tenofovir DF was reported in patients with chronic hepatitis B after 6 years of treatment. In another study, sequencing of the HBV polymerase/reverse transcriptase indicated sequence changes at polymorphic sites, though none resulted in drug resistance. In total, there were only 16 cases of virologic breakthrough, 12 of which were associated with nonadherence to study medication. Resistance for tenofovir DF remained undetectable throughout a 5-year span. By comparison, lamivudine resistance was calculated to be 24% in the first year, and this number steeply climbed to 70% by year 5.
Entecavir has shown improved antiviral activity compared to adefovir in randomized open-label studies in patients with chronic hepatitis B. A few small case studies have evaluated entecavir in the prevention or treatment of HBV in patients with cancer (reviewed by Liu et al). Entecavir had a low drug resistance of 1.2% at 5 years compared to adefovir, which had an intermediate resistance that increased from 0% in the first year to 29% by year 5.
In addition to drug resistance, the safety profile of the nucleos(t)ide analogues should affect drug selection. Nephrotoxicity has been seen with adefovir and tenofovir (specifically tenofovir disoproxil fumarate [TDF]). No significant side effects have been reported with lamivudine or entecavir; however, it is recommended that all patients be monitored for lactic acidosis and severe hepatomegaly with steatosis.
Risk-based screening is recommended by the American Society of Clinical Oncology (ASCO) and the American Association for the Study of Liver Disease (AASLD). Although it is possible that risk-based screening may be more cost-effective than universal screening, there are currently no validated risk tools that could easily be implemented into clinical practice. Furthermore, <60% of patients with HBV infection may have obvious risk factors,285 and only 10% to 35% of these patients may be aware of their own HBV infection. Therefore, any patient expected to receive IST or chemotherapy should be screened. Implementation of universal screening, as recommended by the CDC, should be considered.
In patients undergoing intensive IST, including HCT, both patient and donor should be screened for HBV, HCV, and HIV prior to treatment. Evaluation of HBsAg, HBcAb, and HBsAb should be considered at baseline. Vaccination against HBV should be strongly considered in patients who are HBV-naïve (ie, negative for HBsAg, HBsAb, and HBcAb) (see Vaccination). In patients who are HBV-naïve undergoing allogeneic HCT, grafts from donors who are HBsAg-positive or HBV DNA-positive should be avoided wherever possible. Donors who have not been exposed to HBV should be considered for HBV vaccination before hematopoietic cell collection.
In individuals who are HBsAg-positive or HBcAb-positive, baseline quantitative PCR for HBV DNA should be obtained. In allogeneic HCT candidates with evidence of active HBV infection (chronic hepatitis based on biopsy or positive HBsAg or high levels of HBV DNA), transplant procedure should be delayed when possible, and antiviral therapy should be given for 3 to 6 months prior to conditioning. In HCT candidates who are HBsAg-positive or HBcAb-positive but without evidence of active HBV replication, antiviral prophylaxis should be considered (starting shortly before the transplant procedure). All allogeneic HCT recipients should continue surveillance for at least 12 months after transplant or during GVHD.
The optimal choice of antiviral agents for prophylaxis (or preemptive approaches) will primarily be driven by institutional standards. The NCCN Panel recommends consultation with an expert in hepatitis treatment to determine appropriate antiviral prophylaxis for patients who test positive for HBV. Preferred agents for HBV prophylaxis are entecavir and tenofovir. Although data were originally obtained with lamivudine, entecavir and tenofovir are preferred, especially when treating patients with active HBV infections due to the low threshold of resistance with lamivudine. Monitoring of HBsAg and HBV DNA and transaminases should be considered for patients without active HBV infection who are not receiving prophylaxis.