Chronic Lymphocytic Leukemia / Small Lymphocytic Lymphoma (CLL/SLL)
28–42 minutes
Based on NCCN Clinical Practice Guidelines in Oncology: CLL/SLL, Version 2.2026 (December 22, 2025). For educational and clinical reference use only. Always verify with current guidelines and prescribing information.
1. DIAGNOSIS & DISEASE DEFINITION
1.1 CLL vs SLL vs MBL
Entity
Diagnostic Criteria
Key Distinction
CLL (Chronic Lymphocytic Leukemia)
Monoclonal B lymphocytes ≥5 × 10⁹/L in peripheral blood (confirmed by flow cytometry); clonality confirmed
Blood-based; no lymph node biopsy needed if flow cytometry diagnostic
SLL (Small Lymphocytic Lymphoma)
Lymphadenopathy and/or splenomegaly WITH monoclonal B lymphocytes <5 × 10⁹/L in peripheral blood; confirmed by LN histopathology
CpG-stimulated metaphase karyotype for complex karyotype (CK)
IGHV mutation status (does NOT need to be repeated once performed prior to treatment)
Beta-2 microglobulin (B2M)
Clinical Pearls – Diagnosis PEARL 1: CLL and SLL are the SAME disease biologically – CLL is leukemic phase, SLL is nodal/solid phase. PEARL 2: MBL is NOT CLL – do NOT treat. High-count MBL (0.5–4.9 × 10⁹/L) progresses to CLL at ~1–2%/year. PEARL 3: IGHV mutation status does NOT change over time – do not repeat if already documented before treatment. PEARL 4: TP53 mutation can exist WITHOUT del(17p) – always sequence TP53 independently; FISH alone is insufficient. PEARL 5: Low VAF TP53 mutations (<10%) may behave similarly to wild-type – but VAF ≥10% = poor prognosis. PEARL 6: CD23 may be dim or negative in some CLL; bright CD20/sIg should trigger MCL workup (FISH t(11;14)).
Pharmacist Watchout – Diagnosis NEVER initiate treatment without FISH + TP53 + IGHV testing – del(17p)/TP53 mutations CONTRAINDICATE chemoimmunotherapy (CIT) as first-line. BTK inhibitors and venetoclax are preferred for del(17p)/TP53-mutated disease at ALL lines of therapy. Fludarabine-based CIT (FCR) in del(17p) patients → inferior response, very short PFS, potentially lethal. MBL: No treatment warranted. Pharmacists should flag inappropriate treatment orders for MBL.
2. STAGING SYSTEMS
2.1 CLL – Rai Staging System
Rai Stage
Description
Modified Risk
Key Feature
0
Lymphocytosis only; lymphocytes >5 × 10⁹/L (blood) or >40% (BM)
Low
Lymphocytosis alone
I
Stage 0 + enlarged lymph node(s)
Intermediate
Lymphadenopathy
II
Stage 0–I + splenomegaly and/or hepatomegaly
Intermediate
Organomegaly
III
Stage 0–II + Hgb <11.0 g/dL OR hematocrit <33%
High
Anemia
IV
Stage 0–III + platelets <100,000/mm³
High
Thrombocytopenia
2.2 CLL – Binet Staging System
Stage
Criteria
A
Hgb ≥10 g/dL AND platelets ≥100,000/mm³ AND <3 enlarged areas
B
Hgb ≥10 g/dL AND platelets ≥100,000/mm³ AND ≥3 enlarged areas
C
Hgb <10 g/dL and/or platelets <100,000/mm³ (any number of areas)
2.3 SLL – Lugano Modification of Ann Arbor Staging
Stage
Nodal Involvement
Extranodal
I
One node or group of adjacent nodes
Single extranodal lesion without nodal involvement
II
≥2 nodal groups, same side of diaphragm
Stage I or II with limited contiguous extranodal involvement
II Bulky
Stage II with bulky disease
N/A
III
Nodes both sides of diaphragm OR above diaphragm + spleen
Clinical Pearls – Staging PEARL: Rai stage alone does NOT drive treatment decision in modern era; del(17p)/TP53 status and IGHV mutation are more important. PEARL: ALC (absolute lymphocyte count) alone is NOT an indication for treatment – even very elevated ALC unless causing leukostasis (very rare in CLL). PEARL: Platelet count >100,000/µL typically not associated with clinical risk – do NOT start treatment for mild thrombocytopenia alone. PEARL: SLL localized (Lugano Stage I) → consider locoregional ISRT (radiation); systemic therapy NOT needed initially. PEARL: CT scans are NOT required for diagnosis, serial monitoring, surveillance, or routine response monitoring outside clinical trials. Use only if clinically indicated (bulky disease symptoms, TLS risk assessment before venetoclax).
3. RISK STRATIFICATION, GENOMICS & CYTOGENETICS
3.1 FISH Cytogenetics – Clinical Association (Dohner Hierarchy)
Abnormality
Frequency
Prognosis
Key Clinical Impact
Del(13q) sole
~55%
Favorable
Longest median OS with CIT; favorable TTFT
Trisomy +12
~15%
Intermediate
Intermediate prognosis for TTFT and OS with CIT
Normal
~20%
Intermediate
Intermediate TTFT and OS with CIT
Del(11q)
~10%
Unfavorable
Shortened TTFT; shorter median OS with CIT; often ATM mutation
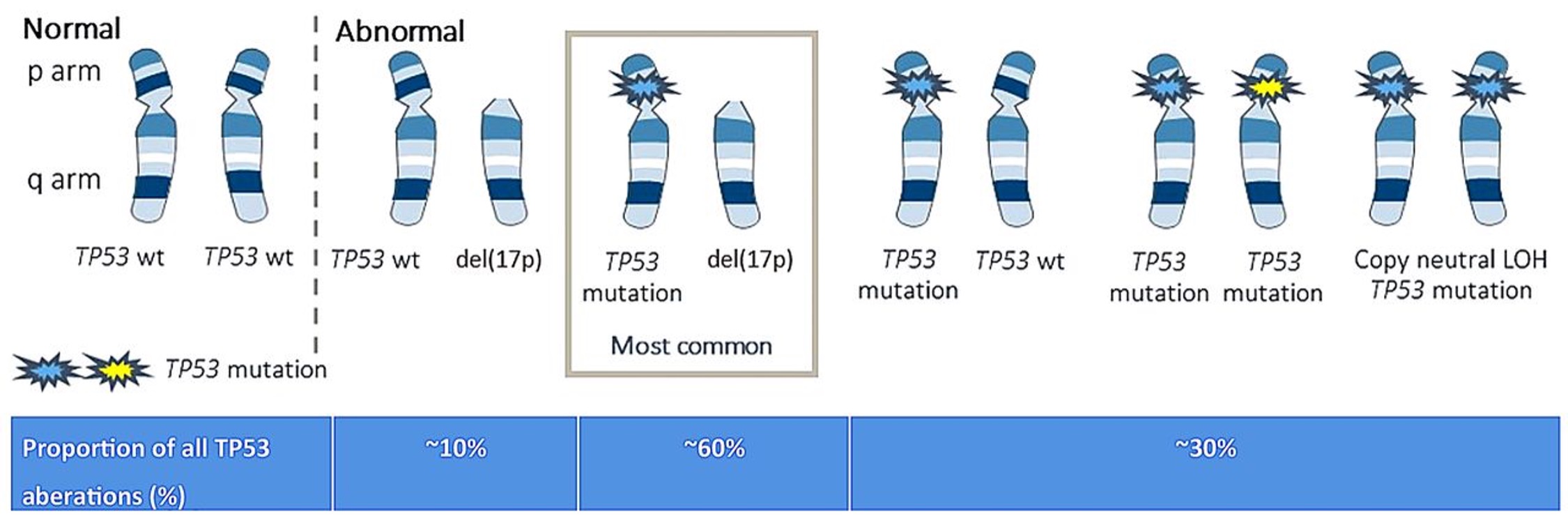
Del(17p)
~7% untx’d; up to 25% R/R
Very Unfavorable
Inferior response to CIT; shorter PFS/OS even with targeted therapy; AVOID CIT as front-line
Del(17p): Loss of TP53 gene locus; frequently co-occurs with TP53 mutation on second allele
TP53 mutation WITHOUT del(17p): Also associated with shortened PFS/OS; outcomes may be slightly more favorable than concurrent del(17p) + TP53 mutation
Low VAF (<10%) TP53 mutations: May behave like wild-type; high VAF (≥10%) = definitely poor prognosis
TP53 aberrations: Increased resistance to ALL chemoimmunotherapy; significantly shortened TTFT and TTNT; increased risk for Richter transformation
BTKi-based and venetoclax-based regimens: Better outcomes than CIT in del(17p)/TP53-mutated CLL, but still inferior to non-mutated CLL
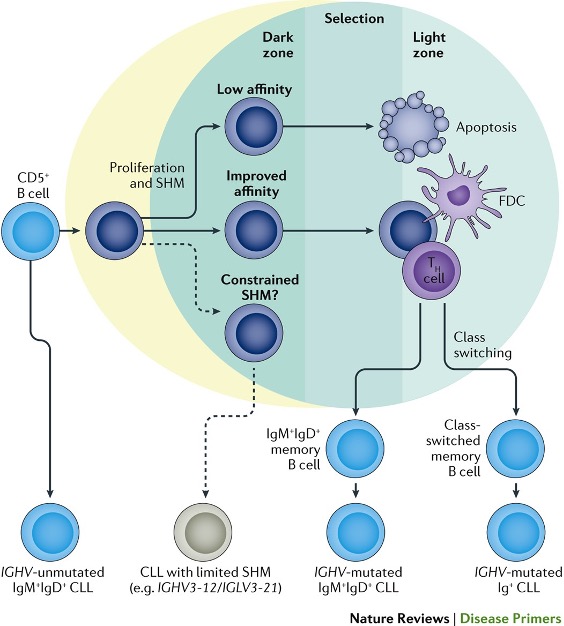
3.3 IGHV Mutation Status
IGHV Status
Definition
Prognosis
Mutated (M-IGHV)
>2% mutation (or <98% homology with germline)
Favorable; longer TTFT/PFS with CIT; particularly durable remissions with FCR in M-IGHV (plateau in PFS at 10+ years)
Unmutated (U-IGHV)
≤2% mutation (or ≥98% homology with germline)
Unfavorable with CIT; shorter TTFT and PFS; however, PFS/OS NOT correlated with IGHV status on cBTKi continuous therapy
SPECIAL NOTE: IGHV4-39 usage → higher risk for Richter’s transformation
SPECIAL NOTE: IGHV VH3-21 gene usage → higher risk regardless of mutation status
IGHV status does NOT predict response rates to BTKi or venetoclax-based regimens (ORR similar), but does impact PFS with time-limited venetoclax regimens
CK defined as: ≥3 unrelated clonal chromosome abnormalities in >1 cell on CpG-stimulated karyotype
High CK: ≥5 unrelated chromosomal abnormalities → adverse independent of stage, IGHV, del(17p)/TP53
High CK may be stronger predictor of poor outcome than del(17p) alone on ibrutinib-based regimens
Low CK (3 abnormalities) and intermediate CK (4 abnormalities) → clinically relevant mainly when co-existing with TP53 aberrations
High CK remains adverse prognostic factor even on venetoclax-based regimens
3.5 Key Gene Mutations (Baseline & Acquired)
Gene
Clinical Association
ATM (del 11q)
Shorter TTFT, PFS, TTNT, OS with CIT vs WT
BIRC3
Shorter TTNT, PFS with CIT; may be more sensitive to BCL2i-containing regimens
NOTCH1
Shorter TTFT, PFS regardless of IGHV; shorter TTNT with CIT; higher risk for Richter transformation
SF3B1
Shorter TTFT and OS with CIT vs WT
BTK C481 / A428D
Resistance mutations in patients progressing on cBTKi (ibrutinib, acalabrutinib, zanubrutinib)
BTK L528 / T474
Resistance on both cBTKi AND ncBTKi (pirtobrutinib)
PLCG2
Resistance to BTK inhibitors (alternative pathway activation)
CARD11
Resistance to BTK inhibitors
BCL2 G101V / D103Y
Venetoclax resistance mutations
3.6 CLL-IPI (International Prognostic Index for CLL)
Variable
Score
Cutoff
TP53 status (del[17p] or mutation)
4 points
Present vs absent
IGHV mutation status
2 points
Unmutated vs mutated
Beta-2 microglobulin
2 points
>3.5 mg/L
Clinical stage
1 point
Binet B/C or Rai I–IV
Age
1 point
>65 years
CLL-IPI Group
Score
5-Year OS
Low risk
0–1
93%
Intermediate risk
2–3
79%
High risk
4–6
63%
Very high risk
7–10
23%
Note: CLL-IPI was developed in CIT era; may underestimate OS in patients treated with targeted/novel therapies
B2M cutoff varies: CLL-IPI uses >3.5 mg/L; other studies use 4 mg/L with CIT; B2M is affected by renal dysfunction independently
Clinical Pearls – Genomics & Risk PEARL: ALWAYS re-check del(17p)/TP53 + CK at disease progression before starting next-line therapy (clonal evolution occurs). PEARL: BTK/PLCG2 mutation testing at progression on BTKi helps confirm resistance vs poor adherence. Mutation status alone ≠ indication to change therapy without disease progression. PEARL: BCL2 G101V mutation = venetoclax resistance. Test at venetoclax progression. PEARL: CK ≥5 is now emerging as a standalone adverse prognostic factor independent of del(17p) – consider as a reason to enroll in clinical trial. PEARL: IGHV VH3-21 = high risk regardless of mutation status – do not classify as favorable based on mutation status alone.
4. SIGNS, SYMPTOMS & CLINICAL PRESENTATION
4.1 Common Presenting Features
Feature
Description / Pearls
Lymphocytosis
Often incidental on CBC; median age at diagnosis 72 years; most common leukemia in Western countries
Lymphadenopathy
Painless, rubbery, non-tender; common in neck, axillae, groin
Splenomegaly / Hepatomegaly
May cause early satiety, left-sided discomfort; spleen >6 cm below costal margin = indication for treatment
B Symptoms
Drenching night sweats, unintentional weight loss ≥10% in 6 months, fever without infection → indication for treatment
Fatigue
Often severe; disease-related anemia or immune dysfunction; severe fatigue = indication for treatment
Cytopenias
Anemia (disease-related or AIHA), thrombocytopenia (disease-related or ITP); progressive cytopenias = treatment indication
Hypogammaglobulinemia
Recurrent sinopulmonary infections; low serum IgG common; consider IVIG if IgG <500 mg/dL with recurrent infections
Autoimmune Complications
AIHA (~10%), ITP (~2%), PRCA (<1%); CLL-associated immune dysregulation; may precede need for CLL treatment
Pharmacist Watchout – Treatment Indications ALC alone is NOT an indication for treatment (even if very high) unless leukostasis is present (very rare in CLL). Mild, stable cytopenia (ANC <1000, Hgb <11, platelets <100K) may still be observed if stable – rule out other causes first (AIHA, vitamin deficiency, drug-induced). Autoimmune cytopenias: Treat the autoimmunity first (steroids, rituximab, IVIG) before initiating CLL-directed therapy unless disease is driving the cytopenia. AIHA with fludarabine: Stop fludarabine immediately; do NOT re-challenge. Use rituximab, steroids, IVIG, or BTKi-based therapy for steroid-refractory AIHA.
>55% prolymphocytes; very high WBC; CD23−; aggressive
CD5+/−, CD23−, CD20 bright, sIg bright
Large Granular Lymphocyte (LGL) Leukemia
T-cell or NK phenotype; neutropenia; rheumatoid arthritis association
CD3+, CD8+, CD57+, CD16+, TCR gene rearrangement
Clinical Pearls – Differential Diagnosis PEARL: MCL is the most critical differential – it can be CD23+ in some cases. ALWAYS check cyclin D1 and/or FISH t(11;14) when immunophenotype is atypical. PEARL: CD200 positivity helps distinguish CLL from MCL. MCL is usually CD200−. PEARL: LEF1 IHC is consistently positive in CLL/SLL and negative in MCL – useful tissue marker. PEARL: SOX11 positivity = MCL (especially cyclin D1-negative MCL). SOX11-negative MCL = indolent variant. PEARL: SPEP/SIFE added to workup in v2.2026 – to evaluate for monoclonal protein and help differentiate from WM or co-existing plasma cell dyscrasia.
6. MANAGEMENT ALGORITHM (NCCN v2.2026)
6.1 First-Line Treatment Decision Framework
BEFORE STARTING ANY TREATMENT – Mandatory Pre-Treatment Evaluation:
1. FISH: del(17p), del(11q), del(13q), trisomy 12
2. TP53 sequencing (NGS preferred)
3. CpG-stimulated metaphase karyotype for complex karyotype
4. IGHV mutation status
5. Cardiovascular risk assessment (BEFORE initiating any BTK inhibitor)
6. Hepatitis B testing (HBsAg + HBcAb) – risk of reactivation
7. Assess TLS risk (especially if planning venetoclax) – CBC with ALC, CT scan if bulky adenopathy
8. Assess pseudohyperkalemia risk before venetoclax (especially with high ALC – check K+ via blood gas or tourniquet-free draw)
Bendamustine + Rituximab (age ≥65 or comorbidities; NOT for del[17p]/TP53)
Other Recommended (Cat 2A del17p; 2B no del17p)
HDMP + anti-CD20 mAb
Consider
Allogeneic HCT (if without significant comorbidities)
Critical Sequencing Pearls PEARL: When transitioning from cBTKi to venetoclax – DO NOT abruptly stop BTKi (risk of disease flare). OVERLAP BTKi with venetoclax ramp-up until disease control achieved. PEARL: Acalabrutinib or zanubrutinib are NOT effective for ibrutinib-refractory CLL with BTK C481S mutation. However, they CAN be used for ibrutinib INTOLERANCE (not progression/resistance). PEARL: Pirtobrutinib (ncBTKi) can overcome cBTKi resistance (C481 mutations), but BTK L528/T474 mutations = resistance to BOTH cBTKi AND pirtobrutinib. PEARL: Treatment-free interval should be as SHORT as possible when transitioning at disease progression. It is safe to overlap venetoclax with a BTKi. PEARL: After CIT first-line – observe until relapse with indications, then use BTKi or BCL2i-based regimens (NOT CIT again in most cases). PEARL: Ibrutinib is NOT listed as preferred due to its toxicity profile (afib, bleeding, hypertension) compared to acalabrutinib/zanubrutinib.
7. KEY DRUGS: DOSING, ADJUSTMENTS & MONITORING
7.1 BTK Inhibitors (cBTKi)
Drug
Dose
Key Adjustments
Critical Monitoring
Ibrutinib (Imbruvica®) Covalent BTKi
420 mg PO once daily (continuous) With water; take same time daily; do NOT crush/chew
CBC (cytopenias), BMP (creatinine), LFTs Afib/flutter/ventricular arrhythmia – hold, then reassess Bleeding – especially with anticoagulants Hypertension – monitor and manage Atrial fibrillation – high incidence (~9%) Hold 3 days before/after minor surgery; 7 days before/after major surgery
Acalabrutinib (Calquence®) Covalent BTKi (2nd gen) (More selective for BTK)
100 mg PO BID (continuous) ~12 hours apart; with or without food Capsules: Do NOT open Tablets: Can be crushed; avoid with PPIs (use H2 blocker if needed – give acala 2 hrs before or 10 hrs after PPI)
Hepatic: Child-Pugh A/B: 100 mg BID; Child-Pugh C: Avoid CYP3A4 strong inhibitors: Reduce to 100 mg once daily CYP3A4 strong inducers: AVOID Renal: No dose adjustment; dialysis: use with caution Antacids/PPIs: Affect absorption of capsule formulation (NOT tablets)
CBC, LFTs, BMP Headache (very common – usually mild, 1st month) Afib (lower rate than ibrutinib ~4%) Bleeding, bruising Second primary malignancies Hold 3 days before/after minor; 7 days before/after major surgery Avoid concurrent ≥3 antiplatelet/anticoagulant agents
160 mg PO BID OR 320 mg PO once daily (continuous) With or without food; Capsules: Do NOT open
Hepatic: Child-Pugh A/B: no adjustment; Child-Pugh C: reduce to 80 mg BID CYP3A4 strong inhibitors: Reduce to 80 mg once daily CYP3A4 moderate inhibitors: Reduce to 80 mg BID CYP3A4 strong inducers: AVOID Renal: No adjustment; dialysis: use with caution
CBC, LFTs, BMP Afib (low rate ~2%) Neutropenia, infections Bleeding/bruising Skin rash Hold 3 days before/after minor; 7 days before/after major surgery Lower cardiovascular toxicity than ibrutinib (head-to-head ALPINE trial)
200 mg PO once daily (continuous) With or without food; swallow whole
Hepatic: No dose adjustment in mild/mod; severe hepatic: not well studied CYP3A4 strong inhibitors: Reduce to 100 mg/day CYP3A4 strong inducers: AVOID Renal: No dose adjustment
No dose adjustment for CrCl ≥15 mL/min; avoid strong CYP3A4 inhibitors in ramp-up; reduce to 100 mg if moderate CYP3A4 inhibitor must be used
Hepatic adjustment
Mild/moderate: no adjustment; Severe (Child-Pugh C): reduce dose by ≥50%
CYP3A4 strong inhibitors
During ramp-up: AVOID if possible; if needed – reduce dose by ≥75%. During steady state: reduce dose by ≥50%
CYP3A4 moderate inhibitors
Reduce dose by ≥50% during ramp-up AND steady state
P-gp inhibitors
Reduce dose by ≥50%
Neutropenia management
ANC <1000/µL: consider G-CSF; hold if Grade 4; restart at same dose or reduce
TLS Risk Assessment for Venetoclax (Per PI)
TLS Risk Category
Criteria
Monitoring Setting
Pre-Treatment
Low
All LNs <5 cm AND ALC <25 × 10⁹/L
Outpatient
Hydration 1–2 days before; allopurinol starting 2–3 days before
Medium
Any LN 5–10 cm OR ALC ≥25 × 10⁹/L
Outpatient with labs 6–8 hrs post-dose OR inpatient on Day 1 ramp-up
Hydration + allopurinol; consider inpatient for first ramp-up dose
High
Any LN ≥10 cm OR (LN ≥5 cm + ALC ≥25 × 10⁹/L)
Inpatient for each dose during first ramp-up week
Hydration + allopurinol; consider rasburicase if uric acid elevated
7.3 Anti-CD20 Monoclonal Antibodies
Drug
Dose & Schedule
Pharmacist Notes
Obinutuzumab (Gazyva®) Type II glycoengineered anti-CD20
Cycle 1: 100 mg D1, 900 mg D2, 1000 mg D8, D15; then 1000 mg D1 each cycle Premeds: Corticosteroid (IV methylprednisolone 20 mg or equivalent or oral prednisone 20 mg/dexamethasone 20 mg ≥1 hr before); antihistamine; acetaminophen Consider HDMP (1000 mg x3 doses) for high ALC (>100,000/µL) or very bulky disease before first dose
Severe IRR risk with first infusion especially with high ALC (>100,000/µL) Hold antihypertensive meds surrounding initial dose (BP fluctuations with IRR) HBV reactivation risk – test before treatment TLS risk similar to CIT – monitor closely HBV: entecavir prophylaxis preferred
Rituximab (Rituxan®) / biosimilars Type I anti-CD20
375 mg/m² IV Cycle 1; then 500 mg/m² IV Cycles 2–6 (with FCR/BR) Premedicate: Acetaminophen, diphenhydramine, consider methylprednisolone SC rituximab: Available after at least 1 full IV dose; 1400 mg SC Rapid infusion (90 min): Acceptable if no severe IRR on prior full infusion
Lower efficacy vs obinutuzumab in CLL (obinutuzumab preferred with venetoclax) Biosimilars: FDA-approved biosimilars are appropriate substitutes HBV reactivation risk: Monitor monthly through treatment and q3 months after B-cell recovery ~9 months after rituximab – vaccines given before B-cell recovery may be ineffective
Pharmacist Watchouts – Key Dosing Issues VENETOCLAX + CYP3A4 INHIBITORS: Azoles (fluconazole, voriconazole, posaconazole) dramatically increase venetoclax exposure → TLS risk. Reduce venetoclax dose per PI. If azole initiation is unavoidable during ramp-up, DELAY venetoclax ramp-up. IBRUTINIB + ANTICOAGULANTS: Triple therapy (ibrutinib + aspirin + anticoagulant) = high bleeding risk; do NOT combine ≥3 antiplatelet/anticoagulant agents. ACALABRUTINIB CAPSULE + PPI: PPIs significantly reduce acala capsule absorption. Switch to H2 blocker or use tablet formulation. Capsule requires acidic environment; take 2 hrs before or 10 hrs after PPI if unavoidable. OBINUTUZUMAB IRR: Pre-treat with corticosteroid 1–3 DAYS BEFORE for patients with very high ALC. Monitor closely; have emergency meds available. PSEUDOHYPERKALEMIA: Before venetoclax, rule out pseudohyperkalemia (falsely elevated K+ due to high ALC). Use tourniquet-free draw, blood gas tube, or whole blood K+. DO NOT start venetoclax with unreliable K+ level.
8. SUPPORTIVE CARE (CSLL-C)
8.1 Anti-Infective Prophylaxis
Regimen/Indication
Agent / Dose
Duration
PJP prophylaxis (REQUIRED with PI3Ki, purine analogs, bendamustine-based CIT, alemtuzumab)
TLS untreated: Acute kidney failure, cardiac arrhythmias, seizures, death
TLS Management:
Intervention
Details
Hydration
IV hydration 150–200 mL/hr; maintain urine output >100 mL/hr; start 24–48 hrs before treatment
Allopurinol
Urate synthesis inhibitor; start 2–3 days before treatment; adjust for renal function; may increase 6-MP/azathioprine levels
Febuxostat
Xanthine oxidase inhibitor; alternative to allopurinol; avoid in patients on azathioprine/6-MP
Rasburicase (Elitek®)
Recombinant urate oxidase; degrades uric acid; CONTRAINDICATED in G6PD deficiency (causes hemolysis). Check G6PD BEFORE use. Fixed dose 3–6 mg; often one dose is sufficient. CANNOT use together with samples on ice (degrades uric acid in sample – gives falsely low UA)
Electrolyte management
Aggressive correction of hyperkalemia, hyperphosphatemia, hypocalcemia; dialysis if refractory
8.3 Immunizations
Vaccine
Recommendation
Notes
Influenza
Annual; inactivated (NOT live attenuated)
Patients on rituximab: B-cell recovery ~9 months; vaccinate before rituximab or after recovery
Pneumococcal
Per CDC guidelines (PCV20 or PCV15 + PPSV23)
Higher risk of encapsulated organism infections
Zoster (Shingrix®)
Recombinant, adjuvanted – ALL BTKi patients
Recombinant (not live); 2 doses 2–6 months apart
RSV
Single dose – ALL CLL/SLL patients including age <60
Added in 2026 NCCN update
COVID-19
All CLL/SLL patients; mRNA preferred; boosters per CDC
Response may be blunted with ongoing therapy
AVOID
All live vaccines (including live attenuated influenza, live zoster Zostavax)
Immunocompromised state – live vaccine risk
8.4 Bleeding & BTKi Management
Increased bleeding/bruising risk with all BTK inhibitors (cBTKi and ncBTKi) – BTK is involved in platelet activation
Hold BTKi: 3 days before and after MINOR surgical procedure; 7 days before and after MAJOR surgical procedure
Supportive Care Pearls PEARL: Irradiate ALL blood products in CLL/SLL patients to prevent transfusion-associated GVHD. PEARL: Annual dermatology skin screening for ALL CLL/SLL patients – higher risk of melanoma and non-melanoma skin cancers. PEARL: CMV monitoring required with PI3K inhibitors (idelalisib, duvelisib) and alemtuzumab – PCR at least every 4 weeks; use ganciclovir pre-emptively. PEARL: Progressive multifocal leukoencephalopathy (PML, JCV) can occur with CLL treatments – maintain clinical suspicion. PEARL: Lenalidomide-specific: Aspirin 81 mg PO daily for DVT prophylaxis if platelets >50 × 10¹²/L; dose adjustments for cytopenias; tumor flare management (prednisone 25–50 mg × 5–10 days). PEARL: HCV with CLL: DAA therapy with direct-acting antivirals can result in regression of low-grade B-cell NHL associated with HCV.
9. KEY CLINICAL TRIALS (Brief Summary)
Trial
Population
Intervention vs. Comparator
Key Results / Outcomes
CLL14 (Eichhorst, NEJM 2023)
Treatment-naïve CLL, elderly/comorbid (CIRS >6 or CrCl <70)
Venetoclax + Obinutuzumab (12 cycles, fixed-duration) vs Chlorambucil + Obinutuzumab
6-yr PFS ~57% vs 17%; uMRD4 blood 76% vs 35%; uMRD6 blood 57% vs 8%; OS not significantly different at 5 yr. del(17p)/TP53 + IGHV-unmutated → shortest PFS
Zanubrutinib superior ORR (80% vs 73%); LESS afib (5% vs 13%); less cardiac events; no significant OS difference; zanubrutinib preferred over ibrutinib
E1912 (Shanafelt, Blood 2022)
Treatment-naïve CLL age ≤70
Ibrutinib + Rituximab vs FCR
5-yr PFS: Ibrutinib-R superior overall; FCR comparable in IGHV-mutated. Ibrutinib-R better for IGHV-unmutated. OS benefit for ibrutinib-R
Clinical Trials Pearls for Pharmacists PEARL: CLL14 established venetoclax + obinutuzumab (VenO) as fixed-duration standard; obinutuzumab is PREFERRED over rituximab with venetoclax. PEARL: AMPLIFY (2025) established AVO (acalabrutinib + venetoclax ± obinutuzumab) as new preferred Category 1 option – highest uMRD rates reported. PEARL: FLAIR (2025) confirmed MRD-guided venetoclax/ibrutinib as valid strategy – 79% stopped treatment at 6 years based on uMRD achievement. PEARL: ALPINE confirmed zanubrutinib > ibrutinib for safety (especially afib) with equal/superior efficacy – explains why ibrutinib moved off preferred list. PEARL: CAR T-cell therapy (liso-cel) now has a role in CLL – after both BTKi and BCL2i failure; CRS management critical.
Most widely available; ERIC-standardized; does NOT require pretreatment sample; preferred for clinical use
NGS-based assay (ClonoSEQ)
≤10⁻⁶ (MRD6)
Only FDA-cleared assay in US; REQUIRES pretreatment sample; most sensitive; used in clinical trials
ASO-PCR
≤10⁻⁴ to ≤10⁻⁵
Expensive, labor-intensive, less available; requires pretreatment sample
uMRD4 = undetectable MRD at <10⁻⁴ sensitivity (1 CLL cell per 10,000 leukocytes)
uMRD6 = undetectable MRD at <10⁻⁶ (deepest remission achievable with venetoclax-based regimens)
Serial MRD monitoring: Every 3–6 months during active treatment in MRD-guided protocols
CAUTION: Anti-CD20 mAb given within prior 3 months → false uMRD4 in blood (B-cell depletion, not true uMRD)
MRD-guided treatment decisions: Specific to clinical trial protocols – use published criteria for stopping rules
MRD in BTKi therapy: Continuous BTKi monotherapy rarely achieves uMRD; combinations with CD20 mAb achieve higher uMRD
MRD Pearls PEARL: NGS-based MRD testing (ClonoSEQ): Must collect a BASELINE sample BEFORE treatment begins – cannot be done retrospectively. PEARL: Blood MRD is more convenient than BM MRD but BM MRD is more sensitive for treatment discontinuation decisions (deeper measure). PEARL: uMRD4 at EOT with VenO predicts improved PFS and OS. 6-yr PFS: 62% for uMRD6 vs 23% for detectable MRD4. PEARL: IGHV-unmutated, del(17p), and genomic complexity = higher risk of MRD conversion to detectable and subsequent progression. PEARL: Obinutuzumab within 3 months causes B-cell depletion that can mask true MRD status in blood (false uMRD4). Bone marrow MRD is more reliable in this setting.
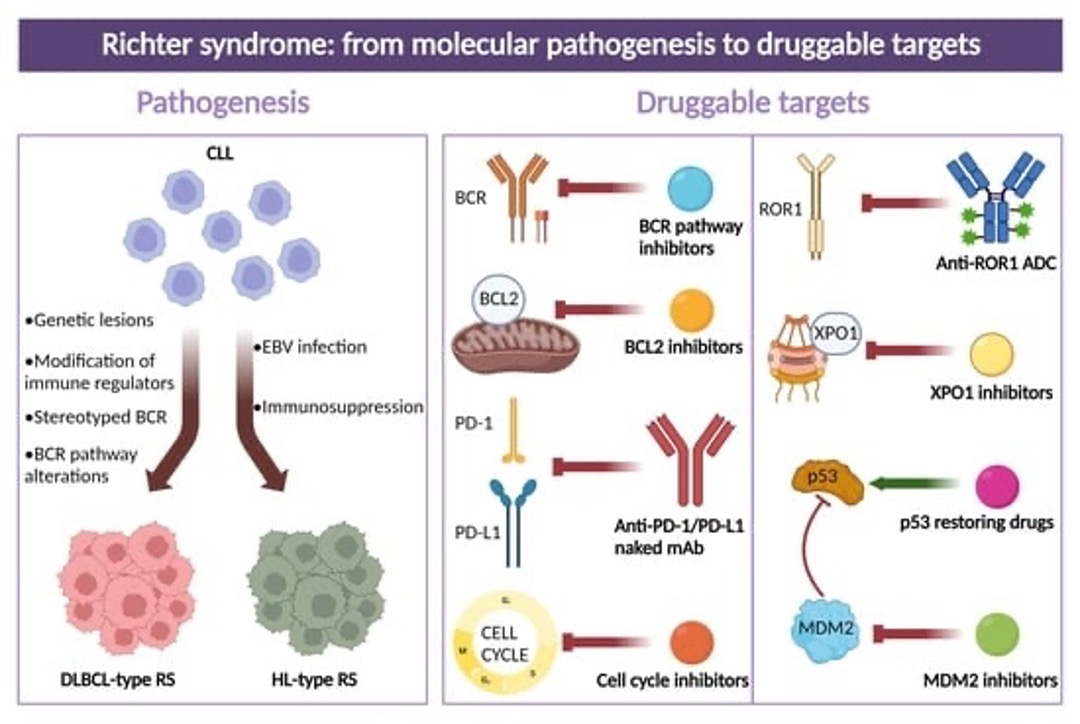
11. HISTOLOGIC TRANSFORMATION (RICHTER SYNDROME)
11.1 Definition & Background
Richter Transformation (RT): Transformation of CLL/SLL to an aggressive lymphoma, most commonly Diffuse Large B-Cell Lymphoma (DLBCL) (~95% of cases), rarely Classic Hodgkin Lymphoma (cHL, ~5%)
Incidence: ~2–10% of CLL patients; median OS historically <12 months for clonally related DLBCL
Clonal relatedness (IGH gene rearrangement): Determines prognosis and treatment approach
Clonally UNRELATED RT (de novo DLBCL arising independently) → better prognosis; treated like standard DLBCL
Clonally RELATED RT → worse prognosis; CIT regimens often inadequate
Accelerated CLL (expanded proliferation centers, Ki-67 >40%) and CLL with increased prolymphocytes (>15%) = NOT Richter transformation; they represent CLL progression
11.2 Diagnosis of Richter Transformation
SUSPECT when: Rapid lymph node growth (discordant with other sites), elevated LDH, B symptoms, new extranodal disease
FDG-PET/CT: Preferred imaging; biopsy lesion with SUV ≥5 (especially if discordant elevated uptake)
Excisional or incisional biopsy preferred; FNA INADEQUATE alone
IGH gene rearrangement studies: Compare CLL tissue vs. transformed tissue (commercial NGS or lab-based assay)
EBV stain (EBER-ISH): If RS-like cells seen; EBV+ CLL can produce RS-like cells but background is still CLL → NOT Richter; do NOT diagnose RT in this setting
PET/CT required for response assessment (Lugano 5-Point Scale)
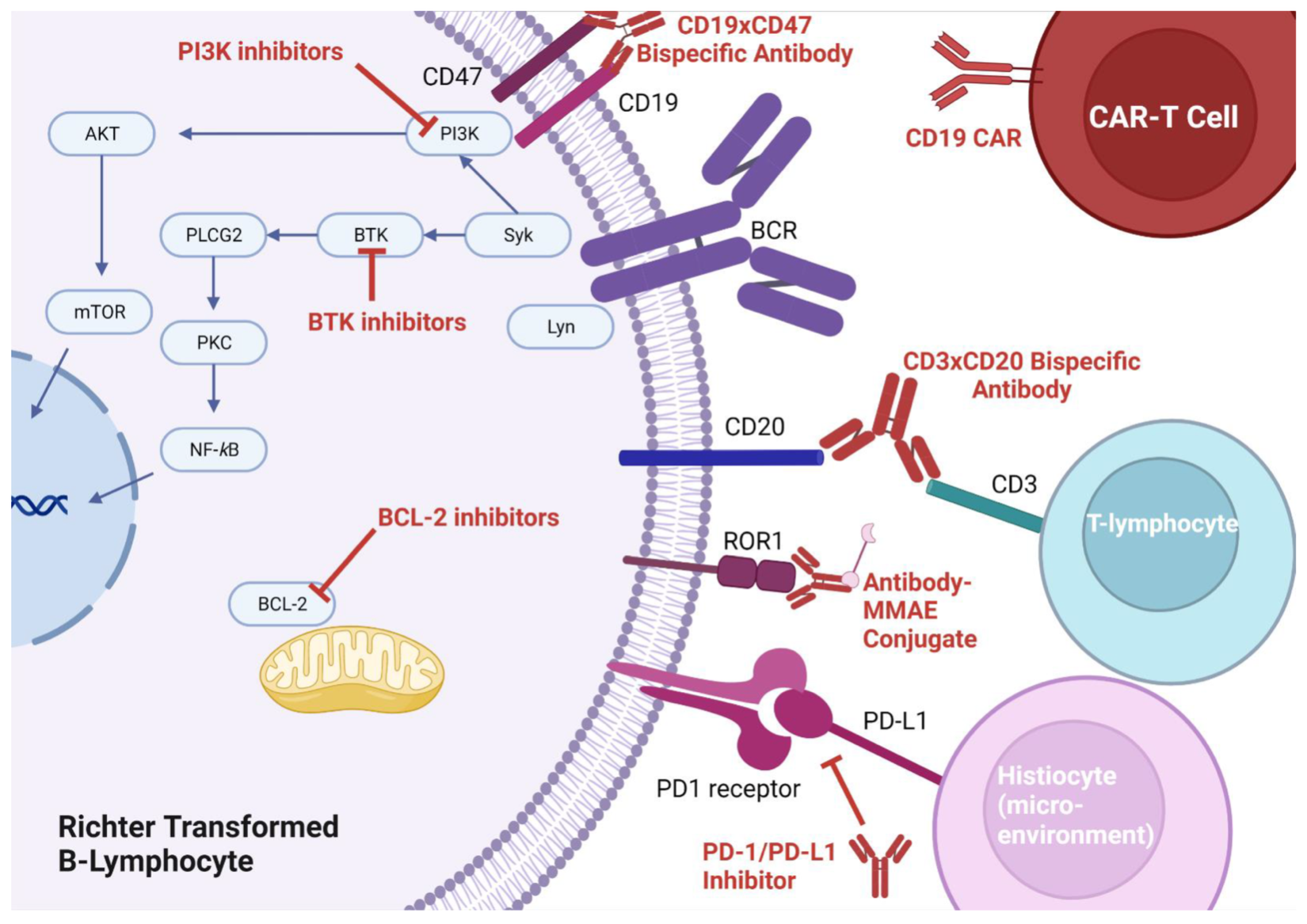
11.3 Treatment of Richter Transformation to DLBCL
Presentation
Preferred Treatment
Subsequent Options
Untreated CLL or clonally UNRELATED RT
Clinical trial (preferred) OR CIT regimens (CHOP-R, DA-EPOCH-R, HyperCVAD-R, OFAR-R)
If CR → consider allogeneic HCT
Previously treated CLL, clonally RELATED (or unknown)
Clinical trial (preferred) OR Non-CIT regimens (BTKi, ICI-based, bispecifics, CAR T)
CAR T-cell therapy after ≥1 prior systemic therapy; allogeneic HCT in CR
RT – Any
CAR T-cell therapy (liso-cel, axi-cel, tisa-cel) – after ≥1 prior systemic therapy
Allogeneic HCT if eligible and CR achieved
Non-CIT Regimens for Richter Transformation (HT-A):
Richter Transformation – Critical Pharmacist Watchouts Do NOT delay initiating treatment for clonality testing results – start treatment empirically if clinical suspicion is high. CLL that was previously treated with BTKi: ICI-based combinations containing the SAME cBTKi used prior are NOT appropriate if intolerant or progressed on that BTKi. CLL with del(17p)/TP53 mutation: Paucity of data for CIT regimens; limited responses. Non-CIT regimens preferred. CIT regimens (CHOP-R etc.) are reasonably SAFE to combine with cBTKi (given continuously for CLL disease control during Richter treatment). Checkpoint inhibitors + BTKi: Significant immune-mediated toxicity risk; monitor closely for irAEs. CAR T-cell therapy for RT: Manage CRS and ICANS per NCCN CAR T toxicity guidelines. Transformation to CHL: Treat per NCCN Hodgkin Lymphoma guidelines.
Main SE: Neutropenia, TLS (HIGH RISK – ramp-up mandatory), infections, anemia, thrombocytopenia, diarrhea, nausea TLS: 5-week ramp-up non-negotiable; G6PD test before rasburicase; pseudohyperkalemia rule-out CYP3A4: Major substrate; azoles → markedly increase exposure; avoid grapefruit Counseling: Take with food; swallow whole; same time daily; report fevers, black stools, bleeding, shortness of breath Duration: Fixed (12–24 months per protocol) or MRD-guided – NOT indefinitely continuous
Main SE: Afib/flutter (9%), hypertension, bleeding/bruising, infections, diarrhea, arthralgias, fatigue, rash Cardio: Baseline CV assessment mandatory; manage afib (rate control; hold for serious afib); avoid venetoclax combination for afib patients Drug-drug: CYP3A4 substrate (strong); major interaction with azoles, anticoagulants NOT preferred: NCCN moved to Other Recommended due to toxicity profile vs newer BTKi Counseling: Swallow whole; do not crush. Report palpitations, unusual bruising, blood in stool. Hold before surgery.
Acalabrutinib (Calquence®)
Covalent BTKi (2nd gen; more selective) MOA: Highly selective irreversible BTK inhibitor (C481); less off-target kinase inhibition vs ibrutinib
Main SE: Headache (very common, usually mild, 1st month – treat with caffeine or analgesics), infections, neutropenia, afib (~4%, lower than ibrutinib), bruising, diarrhea Drug-drug: CYP3A4 substrate; significant interaction with PPIs (capsule formulation) Formulations: Capsule vs tablet – capsule affected by gastric pH, tablet is NOT. Capsule requires acidic environment. Counseling: BID dosing ~12 hrs apart; do not open capsules; if using H2 blocker give acala at least 2 hrs before or 10 hrs after PPI.
Zanubrutinib (Brukinsa®)
Covalent BTKi (2nd gen; most BTK-selective) MOA: Highly selective irreversible BTK inhibitor; designed for complete BTK occupancy
Main SE: Neutropenia, infections, bruising, hemorrhage, afib (~2%, lowest of all BTKi), rash, diarrhea, fatigue Advantage: Superior to ibrutinib in afib rate (ALPINE); most BTK-selective → less off-target kinase inhibition Dosing: 160 mg BID or 320 mg QD – clinically equivalent Counseling: With or without food; do not open capsules; report fever, unusual bleeding, palpitations; hold before surgery.
Pirtobrutinib (Jaypirca®)
Noncovalent BTKi (ncBTKi; reversible) MOA: Non-covalently and reversibly binds BTK active site; overcomes C481 covalent BTKi resistance mutations
Main SE: Neutropenia (most common), fatigue, musculoskeletal pain, diarrhea, bruising, infections Resistance: BTK L528W and T474I mutations = resistance to pirtobrutinib AND cBTKi Use case: AFTER cBTKi resistance or intolerance; preferred ncBTKi for post-cBTKi progression Counseling: QD dosing; with or without food; swallow whole; monitor CBC closely (neutropenia).
Obinutuzumab (Gazyva®)
Anti-CD20 mAb (Type II, glycoengineered) MOA: Direct cell death, ADCC, ADCP; glycoengineered for enhanced FcγRIII binding → superior efficacy vs rituximab in CLL
Main SE: Severe infusion reactions (esp. 1st dose and high ALC), TLS, neutropenia, thrombocytopenia, infections, HBV reactivation IRR prevention: Corticosteroid + antihistamine + acetaminophen; HDMP 1000 mg × 3 days for very high ALC/bulky disease before 1st dose; hold antihypertensives around 1st infusion HBV: Test all patients; prophylactic entecavir if HBsAg+ or HBcAb+ Counseling: IV administration; stay for monitoring after infusion; report fever, chills, difficulty breathing, unusual bleeding. Annual dermatology exam.
Rituximab (Rituxan®) + biosimilars
Anti-CD20 mAb (Type I) MOA: CDC, ADCC; less direct cell death than obinutuzumab; binds CD20 on B-cells
Main SE: IRR (1st infusion), neutropenia, HBV reactivation, PML (rare), cytopenias Subcutaneous: Available after ≥1 full IV dose; 1400 mg SC (with hyaluronidase); different administration vs IV Rapid infusion: 90-min infusion acceptable if no severe IRR on prior cycle HBV: Monitor monthly during treatment; q3 months after; maintain prophylaxis 12 months post-treatment Biosimilars: FDA-approved biosimilars are appropriate substitutes per NCCN
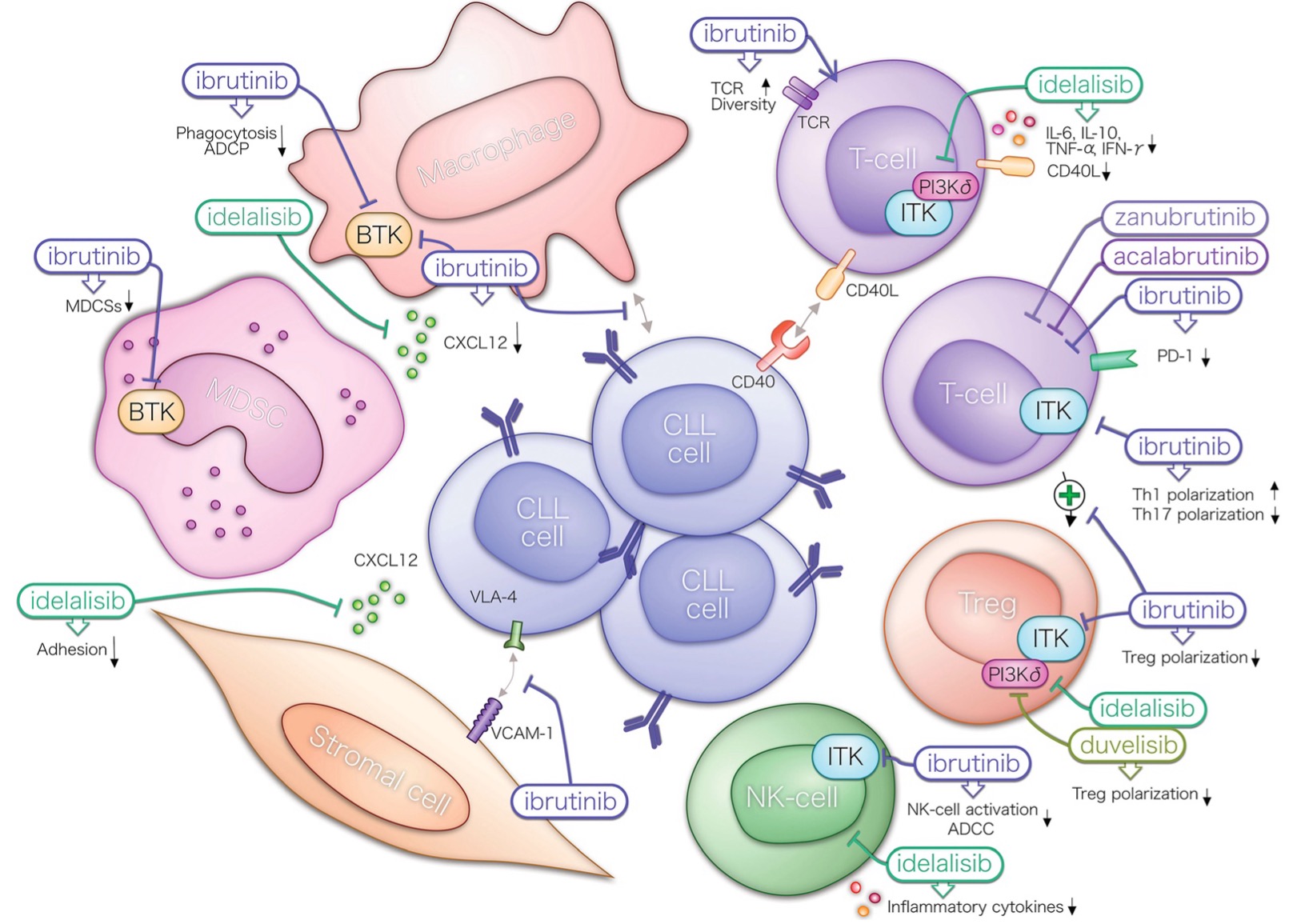
Duvelisib (Copiktra®)
PI3K-delta/gamma inhibitor MOA: Dual inhibition of PI3Kδ (lymphocyte signaling) and PI3Kγ (tumor microenvironment) → CLL cell death + immune modulation
Main SE: Diarrhea/colitis (often severe), pneumonitis, hepatotoxicity, CMV reactivation, infections (PJP, CMV, fungal), cytopenias Prophylaxis required: PJP (TMP-SMX) + herpes (acyclovir); CMV monitoring (PCR q4 weeks) Hold/discontinue: For Grade ≥3 diarrhea, pneumonitis, hepatotoxicity, skin reactions Counseling: With or without food; report diarrhea immediately; avoid live vaccines.
Main SE: Hepatotoxicity (ALT/AST elevation, often early onset), diarrhea/colitis, pneumonitis, severe skin reactions, CMV reactivation, infections Black Box Warning: Fatal and serious hepatotoxicity, diarrhea, colitis, pneumonitis, intestinal perforation, and serious skin reactions Prophylaxis: PJP + herpes prophylaxis mandatory; CMV monitoring LFT monitoring: Check at baseline, every 2 weeks for 3 months, monthly thereafter; hold for ALT/AST >5× ULN Counseling: Take with or without food; report diarrhea, bloody stool, rash, difficulty breathing, jaundice immediately.
Main SE: Tumor flare reaction (painful lymph node enlargement, fever, rash – manage with steroids), cytopenias (dose-limit), DVT/PE, teratogenicity (REMS program) REMS (RevAssist): Mandatory enrollment; pregnancy testing required; iPledge-like program DVT prophylaxis: Aspirin 81 mg PO daily if platelets >50K; patients on anticoagulation: continue anticoagulant Tumor flare: Prednisone 25–50 mg × 5–10 days; prophylaxis with prednisone 20 mg × 5–7 days if bulky nodes >5 cm Counseling: Do not crush; pregnancy prevention mandatory; report chest pain, leg swelling, shortness of breath, rash.
Lisocabtagene maraleucel (Breyanzi®) – liso-cel
CD19-directed CAR T-cell therapy MOA: Autologous T cells engineered with CD19-CAR; 4-1BB costimulatory domain; kills CD19+ CLL/RT cells
Main SE: CRS (cytokine release syndrome) – fever, hypotension, hypoxia (Grade 1–2 most common; Grade 3+ managed with tocilizumab +/- corticosteroids); ICANS (neurotoxicity – tremor, aphasia, encephalopathy) Administration: Inpatient or outpatient center; bridging therapy may be needed; lymphodepleting chemotherapy (fludarabine + cyclophosphamide) before infusion CRS Management: Tocilizumab 8 mg/kg IV (max 800 mg); Grade ≥3 add corticosteroids; see NCCN CAR T toxicity guidelines ICANS Management: Corticosteroids; neurology consult; anti-seizure prophylaxis if Grade ≥2 Counseling: Patient/caregiver must live within 2 hrs of treatment center for ≥4 weeks; do not drive; report confusion, fever, breathing difficulty immediately.
13. AUTOIMMUNE COMPLICATIONS IN CLL/SLL
Complication
Diagnosis
Treatment
AIHA (Autoimmune Hemolytic Anemia) ~10% of CLL
Reticulocyte count, haptoglobin (low), direct Coombs (DAT+), indirect bilirubin (elevated)
1st line: Corticosteroids (prednisone 1 mg/kg/day) 2nd line: Rituximab, IVIG, cyclosporin A Steroid-refractory: BTKi-based CLL therapy Fludarabine-related AIHA: STOP fludarabine permanently; do NOT re-challenge
ITP (Immune Thrombocytopenic Purpura) ~2% of CLL
Bone marrow evaluation to confirm platelet cause; exclude disease-related thrombocytopenia
1st line: Corticosteroids, IVIG 2nd line: Rituximab, cyclosporin A, splenectomy TPO agonists: Eltrombopag or romiplostim for refractory ITP
PRCA (Pure Red Cell Aplasia) <1% of CLL
Bone marrow evaluation; test for parvovirus B19, herpesviruses; exclude drug effects
Critical Point: Fludarabine & AIHA Fludarabine-associated AIHA can be life-threatening. STOP fludarabine immediately if AIHA occurs. DO NOT re-challenge with fludarabine-containing regimens in patients with history of fludarabine-associated AIHA. AIHA does NOT preclude use of combination therapy containing fludarabine INITIALLY – observe carefully. But discontinue at first sign of AIHA. BTKi-based therapy has shown efficacy for steroid-refractory or recurrent AIHA in CLL – a CLL-directed approach that addresses both the underlying disease and the autoimmune complication.
DIAGNOSIS & GENOMICS Never treat without del(17p)/TP53 + IGHV + FISH + CK testing. These drive ALL treatment decisions. IGHV mutation status does NOT change – document once pre-treatment; no need to retest. TP53 mutation exists WITHOUT del(17p) – always test TP53 by sequencing, not just FISH. Low VAF TP53 (<10%) may behave like WT – but VAF ≥10% = confirmed poor prognosis. CK ≥5 (high CK) = independent adverse prognostic factor; stronger predictor than del(17p) alone on ibrutinib. Always recheck del(17p)/TP53/CK at disease progression before next-line therapy – clonal evolution.
TREATMENT SELECTION del(17p)/TP53-mutated CLL: BTKi or venetoclax-based regimens ALWAYS; CIT is CONTRAINDICATED. Ibrutinib: No longer preferred by NCCN due to toxicity (afib, bleeding, hypertension) – acalabrutinib/zanubrutinib preferred. Obinutuzumab preferred over rituximab when using venetoclax-based combinations. Time-limited treatment (VenO, AVO, Ven-Ibrutinib): Achieves uMRD and allows treatment-free intervals. Continuous BTKi: Does NOT achieve uMRD typically; requires continuous therapy until progression. After cBTKi intolerance (no progression): Can switch to alternate cBTKi (acala or zanubrutinib) – OK. After cBTKi progression (C481 mutation): acalabrutinib/zanubrutinib are NOT effective. Use pirtobrutinib or venetoclax.
VENETOCLAX PHARMACOTHERAPY 5-week ramp-up is MANDATORY and NON-NEGOTIABLE – prevents fatal TLS. Pseudohyperkalemia: Rule out BEFORE starting venetoclax in patients with high ALC. CYP3A4 drug interactions: Azoles dramatically increase venetoclax exposure → reduce dose per PI. During ramp-up: AVOID strong CYP3A4 inhibitors if possible; if azole started during ramp-up, PAUSE ramp-up. Venetoclax + BTKi overlap: SAFE and recommended when transitioning from BTKi to venetoclax to prevent disease flare. G6PD testing: MANDATORY before rasburicase.
BTK INHIBITOR PHARMACOTHERAPY Acalabrutinib capsule + PPI: Major drug interaction – capsule requires acidic environment; switch to tablet or H2 blocker. Zanubrutinib: Lowest afib rate (~2%) – preferred for patients with cardiac risk factors. Hold all BTKi: 3 days pre/post minor surgery; 7 days pre/post major surgery. BTKi + anticoagulants: Triple therapy (BTKi + aspirin + anticoagulant) = very high bleeding risk. Cardiovascular assessment BEFORE starting any BTKi – baseline ECG, BP, assess for afib. Lymphocytosis after BTKi initiation: Expected (lymphocyte egress from tissue) – NOT progression; do not switch therapy.
SUPPORTIVE CARE ALL blood products: Must be IRRADIATED to prevent TA-GVHD. AVOID ALL live vaccines in CLL/SLL patients (including live zoster Zostavax, live attenuated flu). Shingrix (recombinant zoster) is SAFE and RECOMMENDED for all BTKi patients. RSV vaccine: Now recommended for ALL CLL/SLL patients including age <60 (NCCN 2026). HBV prophylaxis: Entecavir preferred; avoid lamivudine (resistance); maintain 12 months post-treatment. Annual dermatology screening: Mandatory for all CLL/SLL (elevated skin cancer risk). IVIG if IgG <500 mg/dL with recurrent infections; titrate to maintain nadir ≥500 mg/dL.
MASTER PHARMACIST WATCHOUT LIST
NEVER start CLL treatment without complete genomic profiling (del17p/TP53/IGHV/CK).
CIT (FCR/BR) in del(17p)/TP53-mutated disease = contraindicated → inferior outcomes.