Comprehensive Pharmacotherapy Reference Guide
Guideline used: NCCN Clinical Practice Guidelines v1.2026 (April 2026)
DEFINITION
ALL is a malignancy of B- or T-lymphoid progenitor cells (lymphoblasts) characterised by uncontrolled proliferation and arrest of differentiation. Blasts replace the bone marrow and may infiltrate extramedullary sites (CNS, testes, lymph nodes, mediastinum).
EPIDEMIOLOGY
| Parameter | Key Data |
|---|---|
| Annual US cases | ~6,000–7,000 (ALL); bimodal peak: children <5 yrs & adults >50 yrs |
| Pediatric B-ALL | ~85% of pediatric ALL; 5-yr OS >90% with modern regimens |
| AYA (15–39 yrs) | Less favorable cytogenetics vs. children; higher Ph+ incidence |
| Adult ALL | 5-yr OS ~40–50%; drastically lower than pediatric due to comorbidities & worse biology |
| T-ALL | ~15% of ALL; bimodal peak (children & young adults); associated with mediastinal mass |
CLINICAL PRESENTATION
Symptoms reflect bone marrow failure and extramedullary disease:
- Bone marrow failure: fatigue, pallor (anemia); bleeding/petechiae/ecchymosis (thrombocytopenia); recurrent infections (neutropenia)
- Hyperleukocytosis (WBC >100,000/µL): leukostasis → pulmonary/CNS symptoms (dyspnea, confusion, headache)
- Organomegaly: hepatomegaly, splenomegaly (50–75%), lymphadenopathy
- Bone pain/arthralgia: common in pediatric patients (due to marrow expansion)
- Mediastinal mass (T-ALL): SVC syndrome, respiratory compromise — ONCOLOGIC EMERGENCY
- CNS involvement: headache, papilledema, cranial nerve palsies, seizures
- Testicular involvement: painless testicular enlargement (relapsed disease)
- B symptoms: fever, night sweats, weight loss (less common than lymphoma)
Clinical Pearls
- Mediastinal mass + superior vena cava syndrome in a young adult = T-ALL until proven otherwise. Avoid biopsy under general anesthesia if airway compromise is present.
- WBC >100,000/µL = leukostasis risk → emergent leukapheresis or cytoreduction (hydroxyurea/steroids) before definitive chemotherapy.
- Bone pain mimicking osteomyelitis or juvenile arthritis is common in pediatric ALL — always get CBC before assuming MSK cause.
- Testicular involvement is a sanctuary site (limited drug penetration). Must evaluate in male patients with relapse.
DIAGNOSIS (NCCN ALL-1)
Diagnostic criteria: Diagnosis requires bone marrow aspirate/biopsy demonstrating ≥20% lymphoblasts (immunophenotypically clonal). A clonal lymphoblast population of <20% may be considered ALL in appropriate clinical circumstances.
| Test | Requirement | Clinical Relevance |
|---|---|---|
| Bone Marrow Aspirate + Biopsy | Required | H&E stain; ≥20% blasts; morphology classification |
| Immunophenotyping (Flow Cytometry) | Required | B- vs T-lineage, myeloid markers; aberrant antigen expression (CD10, CD19, CD20, CD34, TdT, CD3, CD7, etc.) |
| Cytogenetics (Conventional Karyotype) | Required | G-banded metaphase analysis for chromosomal abnormalities |
| FISH Panel | Required | BCR::ABL1, KMT2A, ETV6::RUNX1, MYC, others as indicated |
| RT-PCR for BCR::ABL1 | Required | Distinguish p190 vs p210 transcript — critical for treatment & MRD monitoring |
| NGS (Comprehensive Fusion Panel) | Recommended | Detect Ph-like fusions (JAK-STAT, ABL-class), KMT2A partners, DUX4, MEF2D, ZNF384, others |
| MGPT (Multigene Panel Testing) | Recommended | Additional mutations; germline predisposition variants |
| CSF Analysis (LP) | Required at first IT therapy | CNS staging (CNS-1/2/3). Flow cytometry may be considered. |
| CBC with differential, CMP, LDH, Uric Acid | Required | Baseline; TLS risk assessment |
| Coagulation studies (PT, aPTT, fibrinogen, AT) | Required | DIC screen; baseline before asparaginase |
| Echocardiogram or MUGA | Required | Baseline cardiac function before anthracyclines |
| HLA typing | Strongly consider | Early donor search for transplant-eligible patients |
| CT/MRI head with contrast | If neuro symptoms | Rule out CNS bleeding, chloroma, meningeal disease |
| PET/CT (whole body preferred) | If lymphomatous involvement suspected/confirmed by CT | Updated NCCN v1.2026 recommendation |
| Pregnancy test (females of childbearing age) | Required | Before initiating chemotherapy |
| HIV, Hepatitis B/C serology | Required | Infection screen; HBV reactivation risk with rituximab |
| Germline predisposition testing | Recommended | Especially prior to allogeneic HCT; impacts donor/regimen selection |
Immunophenotyping Key Markers
| Lineage | Positive Markers | Negative Markers / Notes |
|---|---|---|
| B-ALL | CD19, CD22, CD79a, PAX5, TdT, CD34 (variable), CD10 (common) | CD10 NEGATIVE → correlates with KMT2A rearrangement. CD20 positivity (>20% blasts) has therapeutic implications (rituximab) |
| T-ALL | CD3 (cytoplasmic or surface), CD7, CD2, CD5, CD4/CD8, TdT | ETP-ALL: CD5 dim/negative, CD1a negative, CD34 positive/negative, stem cell markers + myeloid markers |
| MPAL | Co-expression of lymphoid + myeloid markers meeting WHO/ICC threshold | Requires expert hematopathology review; separate treatment algorithm |
Clinical Pearls
- ALWAYS get BCR::ABL1 RT-PCR and determine transcript type (p190 vs p210) — p190 is more common in de novo Ph+ ALL; p210 may suggest blast-phase CML → different clinical implications.
- FISH t(12;21) ETV6::RUNX1 is typically CRYPTIC by conventional karyotype — requires FISH or PCR. Do not miss it!
- CD20 expression (>20% blasts) in B-ALL: flag for oncologist — rituximab can be added to induction/consolidation. Studies (GRAALL-2005) show improved outcomes.
- ETP-ALL (Early T-cell Precursor): worst prognosis in T-ALL; neoplastic cells resemble early thymic precursors with myeloid/stem cell features. High MRD post-induction → allogeneic HCT.
- LP timing: NCCN recommends first LP at time of initial scheduled IT therapy (not necessarily at diagnosis workup) — reduces risk of traumatic LP seeding blasts to CSF.
- PET/CT now explicitly recommended (updated v1.2026) when lymphomatous involvement is suspected/confirmed by CT.
CNS STAGING & EXTRAMEDULLARY DISEASE (NCCN ALL-B)
CNS Classification
| CNS Status | Definition | Clinical Implications |
|---|---|---|
| CNS-1 | No blasts on cytocentrifuge of CSF | Standard CNS prophylaxis only |
| CNS-2 | <5 WBC/µL with blasts on cytocentrifuge (non-traumatic LP), OR traumatic LP with blasts | Intensified IT therapy; higher-risk classification |
| CNS-3 | ≥5 WBC/µL with blasts OR cranial nerve palsy | Active CNS disease — requires treatment-intensity IT + systemic therapy adjustment |
| Traumatic LP | RBC present; presence of blasts unclear | Assess blasts:RBC ratio; repeat LP may be needed; some protocols upstage |
Extramedullary Sites & Management
- CNS: IT therapy (methotrexate ± cytarabine ± corticosteroid). Cranial irradiation largely replaced by IT + systemic therapy.
- Testes: Testicular radiation (involved site) if bilateral involvement or failure to respond to systemic therapy.
- Mediastinum (T-ALL): Responds to systemic therapy; steroids for rapid cytoreduction if airway compromise.
- Lymph nodes/liver/spleen: Generally respond to systemic chemotherapy; PET/CT for assessment.
Pharmacist Watchout (CNS Prophylaxis)
- IT methotrexate dose is NOT weight/BSA-based — it is AGE-BASED (pediatric protocols) or FLAT-DOSED (adult: typically 12 mg IT MTX). Verify against protocol.
- Leucovorin rescue timing for high-dose IV methotrexate (used in some consolidation regimens) is CRITICAL — must be given per protocol; delayed rescue = severe mucositis, nephrotoxicity.
- NEVER give IT methotrexate and systemic high-dose methotrexate on the same day without explicit protocol guidance.
- Liposomal cytarabine (DepoCyt) dosing and frequency DIFFER from conventional IT cytarabine — do not interchange.
CYTOGENETICS & MOLECULAR RISK STRATIFICATION (NCCN ALL-2)
B-ALL Risk Groups
| Risk Group | Cytogenetic/Molecular Alterations | |
|---|---|---|
| Standard Risk | Hyperdiploidy (51–65 chr) — best if trisomy 4, 10, 17 t(12;21) ETV6::RUNX1 t(1;19) TCF3::PBX1 DUX4 rearranged PAX5 P80R BCR::ABL1 WITHOUT IKZF1plus and without antecedent CML | Favorable prognosis; chemotherapy ± TKI (Ph+) ETV6::RUNX1 is CRYPTIC — needs FISH/PCR BCR::ABL1 alone (no IKZF1plus, no prior CML) = standard risk |
| Poor Risk | Hypodiploidy (<44 chr): – Low hypodiploidy (30–39 chr) – Near triploidy (60–78 chr) TP53 mutation KMT2A rearranged (t[4;11] or others) IgH rearrangements (incl. IGH::IL3) HLF rearranged ZNF384 rearranged MEF2D rearranged MYC rearranged Ph-like (BCR::ABL1-like) ALL: – JAK-STAT (CRLF2r, EPORr, JAK1/2/3r, TYK2r, SH2B3, IL7R) – ABL class (ABL1, ABL2, PDGFRA, PDGFRB, FGFR) – Other (NTRK1/2/3r, FLT3r, LYNr, PTK2Br) PAX5alt BCR::ABL1 WITH IKZF1plus and/or antecedent CML iAMP21 IKZF1 alterations (alone or as IKZF1plus) Complex karyotype (≥5 abnormalities) | Poor prognosis; strong consideration for allogeneic HCT in CR1 IKZF1plus = IKZF1 deletion + CDKN2A/B, PAX5, or other co-deletions → very high risk Ph-like ALL: targetable kinase fusions; JAK-STAT → consider JAK inhibitors; ABL-class → TKI therapy KMT2A t(4;11): very poor prognosis; often CD10-negative Near-haploidy/low hypodiploidy may appear hyperdiploid on flow cytometry (doubled chromosomes) — verify by SNP array |
T-ALL Risk Features
- No universally standardized risk stratification system for T-ALL (unlike B-ALL).
- ETP-ALL: Worst prognosis subset. Markers: CD5 dim/negative, CD1a negative, CD34+/−, myeloid/stem cell markers.
- Non-ETP T-ALL: Better outcomes. Cortical T-ALL (CD1a+, CD4/CD8 double positive) has best prognosis within T-ALL.
- MRD positivity after induction is the strongest prognostic marker for relapse.
- NOTCH1/FBXW7 mutations: favorable; PTEN/RAS/PI3K mutations: worse prognosis.
Adult Risk Stratification Parameters
- High WBC (≥30×10⁹/L for B-ALL; ≥100×10⁹/L for T-ALL): traditional risk factor but may lose independent significance when cytogenetics + MRD are considered.
- Age ≥35 yrs: generally associated with worse outcomes in adults.
- Patients ≥65 years or with substantial comorbidities: classified/managed separately — reduced-intensity regimens.
- MRD status post-induction: strongest independent predictor of outcome regardless of other risk factors.
Clinical Pearls
- Ph-like (BCR::ABL1-like) ALL: ~20–25% of AYA/adult B-ALL. SAME poor prognosis as Ph+ ALL but BCR::ABL1 NEGATIVE. Requires comprehensive NGS to detect actionable fusions. ABL-class → TKI-sensitive; JAK-STAT → ruxolitinib-sensitive.
- IKZF1plus deletion pattern: IKZF1 deletion + CDKN2A/B + PAX5 deletion = very high-risk; these patients should be strongly considered for allogeneic HCT in CR1.
- Near-haploid leukemia TRAP: hypodiploid cells can double their chromosomes appearing as hyperdiploidy on karyotype. Use SNP-array or additional cytogenetic testing to distinguish. Misclassification leads to wrong risk group!
- BCR::ABL1 with IKZF1plus = POOR risk (not standard risk) — different therapeutic pathway.
- iAMP21: amplification of chr 21 fragments — associated with poor prognosis; requires intensified therapy.
DIFFERENTIAL DIAGNOSIS
| Diagnosis | Key Distinguishing Features | How to Differentiate from ALL |
|---|---|---|
| AML (Acute Myeloid Leukemia) | Myeloid blasts; Auer rods | Flow cytometry: MPO+, CD33+, CD117+; TdT usually negative; no lymphoid markers |
| MPAL (Mixed Phenotype Acute Leukemia) | Meets criteria for both lymphoid + myeloid | WHO/ICC criteria; requires expert review; treated differently |
| Burkitt Leukemia/Lymphoma (B-ALL with MYC) | High-grade B-cell; >25% blasts in BM; MYC translocation | Mature B-cell (sIg+, TdT−); distinct morphology; requires specific R-CODOX-M/R-IVAC regimen |
| CML Blast Phase | BCR::ABL1+; prior CML history or evidence of CP/AP CML | p210 transcript; check for chronic phase features; treated as Ph+ ALL but different goals |
| Lymphoblastic Lymphoma (LL) | <25% blasts in bone marrow; predominantly nodal/mediastinal | Same biology as ALL — treated with ALL regimens; CNS prophylaxis same principles |
| Aplastic Anemia | Pancytopenia without blasts | BM biopsy: hypocellular without blasts |
| Viral/EBV infectious lymphocytosis | Reactive lymphocytes | Flow cytometry: polyclonal; self-limiting; no blasts |
| Myelodysplastic Syndrome | Cytopenias with dysplasia | BM dysplastic features; chromosomal analysis; rarely >20% blasts |
TREATMENT PHASES
| Induction | Consolidation | Maintenance | |
|---|---|---|---|
| Goal | Achieve complete remission (CR) and MRD negativity | Eliminate residual disease/MRD; reduce relapse | Long-term disease control; reduce late relapse |
| Duration | 4–8 weeks | Several months (cycles) | 2–3 years |
| Key Components | Corticosteroids, vincristine, asparaginase, anthracycline ± TKI (Ph+). IT chemotherapy throughout. | High-dose methotrexate, cytarabine, asparaginase, anthracyclines, cyclophosphamide, vincristine ± blinatumomab (Ph+/Ph-) ± TKI | Daily 6-MP, weekly MTX, monthly vincristine + prednisone pulses ± TKI (Ph+) |
Ph+ B-ALL TREATMENT (NCCN ALL-4 | ALL-D 5–8 of 29)
Induction — Ph+ B-ALL
NCCN Recommendation: Clinical trial (PREFERRED) OR Systemic therapy + TKI
AYA and Adults <65 yrs Without Substantial Comorbidities — Frontline
| Category | Regimens |
|---|---|
| Preferred | – Clinical trial – HyperCVAD + TKI (dasatinib preferred over imatinib) – Pediatric-inspired regimen (CALGB 10403 modification) + TKI |
| Other Recommended (High Intensity) | – Multiagent induction + TKI (BFM-based) – COG AALL0031-based regimen + TKI |
| Other Recommended (Moderate Intensity) | – ECOG/MRC/MDACC-based regimens + TKI – DA-EPOCH + TKI (Category 2B, added v1.2026) – PhALLCON Regimen + TKI (added v1.2026) – Steroids + TKI (low-intensity option for frail/elderly-like patients) |
Adults ≥65 yrs or Substantial Comorbidities — Frontline
- Steroids + TKI (prednisone/dexamethasone + dasatinib/ponatinib/nilotinib)
- Moderate intensity multiagent regimens + TKI
- Dose-adjusted EPOCH + TKI (Category 2B, v1.2026 addition)
- PhALLCON Regimen + TKI (v1.2026 addition)
- Consider allogeneic HCT in appropriate fit individuals achieving remission (updated v1.2026)
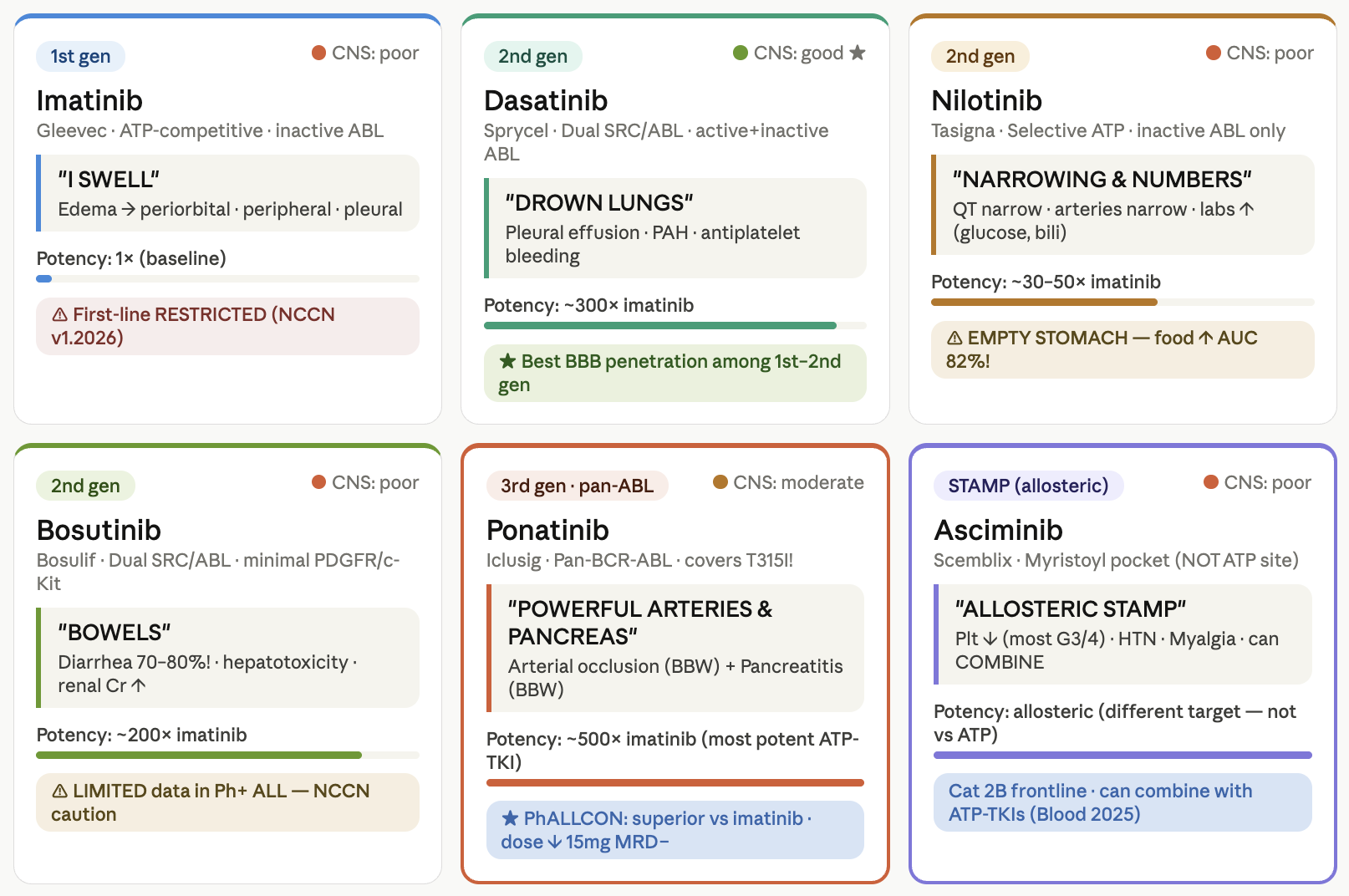
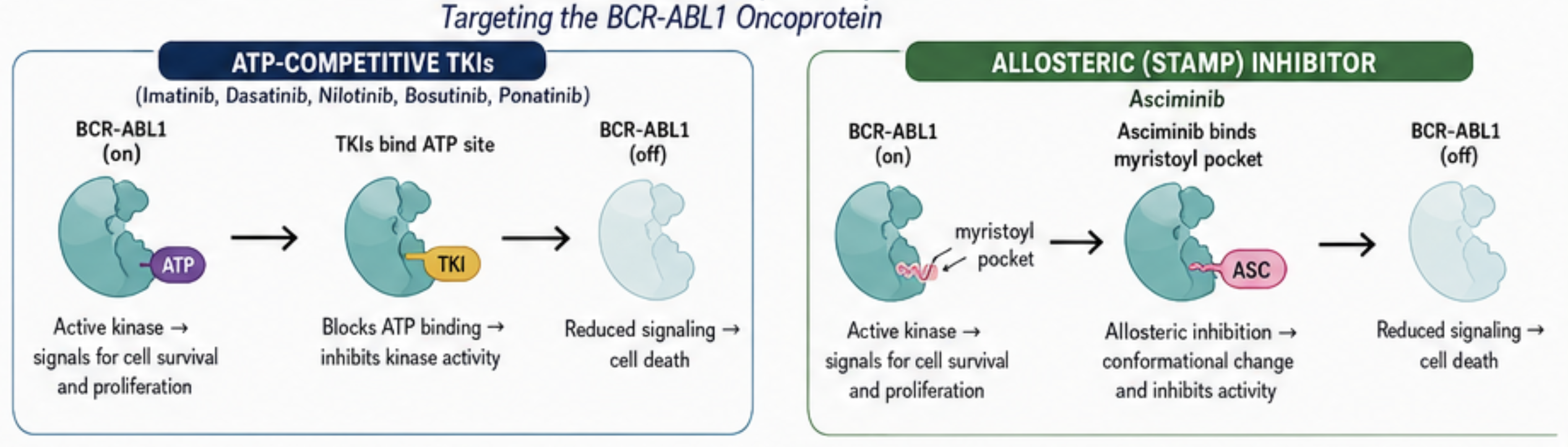
BCR::ABL1 Inhibition Selection — Ph+ B-ALL (NCCN ALL-D 1–2 of 29)
| TKI | Generation | Key Notes for Ph+ ALL |
|---|---|---|
| Imatinib | 1st gen | RESTRICTED to patients who cannot tolerate broader-acting TKIs (per updated v1.2026). Narrow mutation coverage. |
| Dasatinib | 2nd gen | Preferred for first-line (broad BCR::ABL1 coverage; CNS penetration). 100 mg daily (typical ALL dose). Watch: pleural effusion, QTc prolongation, thrombocytopenia. |
| Nilotinib | 2nd gen | Less CNS penetration. Risk: QTc prolongation, pancreatitis. Avoid with strong CYP3A4 inhibitors. |
| Bosutinib | 2nd gen | Limited data in Ph+ ALL specifically (NCCN notes). GI toxicity profile. |
| Ponatinib | 3rd gen | Active against T315I mutation. High potency. Risk: arterial occlusive events, pancreatitis. Dose-adjusted based on response (starting 30–45 mg → reduce to 15 mg for MRD negativity). |
| Asciminib | STAMP inhibitor | Category 2B, useful in certain circumstances — for patients with intolerance/ contraindication to multiple other TKIs. Can be used ± another TKI. |
ABL1 Kinase Domain Mutation Testing
- Perform at: baseline (induction), MRD+ after induction, less than marrow CR, persistent/progressive/emergent MRD, and before switching TKI.
- Note: ABL1 KD mutation testing may be LESS SENSITIVE with minimal disease burden — interpret with caution.
- T315I mutation: ONLY sensitive to ponatinib or asciminib.
- E255K/V, F359V: more resistant to dasatinib — switch to ponatinib.
- Y253H, E255K/V: resistant to nilotinib — switch accordingly.
Dose-Adjusted EPOCH
| Levels | -2 (64%) | -1 (80%) | 1 (100%) | 2 (120%) | 3 (144%) | 4 (173%) | 5 (207%) | 6 (248%) |
| Etoposide (mg/m2/day) D1-4 | 50 | 50 | 50 | 60 | 72 | 86 | 104 | 124 |
| Doxorubicin (mg/m2/day) D1-4 | 10 | 10 | 10 | 12 | 14.4 | 17.3 | 20.7 | 24.8 |
| Cyclophosphamide (mg/m2/day) D5 | 480 | 600 | 750 | 900 | 1080 | 1296 | 1555 | 1866 |
Infusion over 96h (together): etoposide, doxorubicin, vincristine (0.4mg/m2/d, max 2mg/day)
Requires G-CSF prophylaxis (filgrastim 5mcg/kg SC daily on D6+ until ANC >0.5 x109/L of nadir)
Dose adjustments (ANC/platelet for etoposide, doxorubicin, cyclophosphamide on the next cycle)
ANC: ≥0.5 x109/L (↑ 1 level), <0.5 x109/L for 1-2 times (same dose), <0.5 x109/L for ≥3 times (↓ 1 level)
Platelet: <25,000 (↓ 1 level)
CrCl: 15-50 (↓ etoposide 25%), 10 (↓ cyclophosphamide 25%, etoposide 50%)
Bilirubin: 20-50 (↓ doxo 50%, vincr 25%, consider etop), 51-85 (↓ doxo 75%, vincr 50%, consider etop), >85 (omit doxo, etop)
Peripheral neuropathy (motor): G2 (↓ vincr 25%), G3 (↓ vincr 50%), G4 (omit vincr)
Peripheral neuropathy (sensory): G3 (↓ vincr 25%), G4 (omit vincr)
Consolidation — Ph+ B-ALL
| MRD Status Post-Induction | NCCN Recommended Consolidation |
|---|---|
| MRD Positive | Blinatumomab + TKI (PREFERRED — especially for MRD+ and those not previously on blinatumomab) OR Multiagent therapy + TKI (can continue induction if MRD declining; change if MRD+ >3 months) OR Allogeneic HCT in appropriate candidates |
| MRD Negative | Blinatumomab + TKI (preferred, still recommended) OR Continue multiagent therapy + TKI OR TKI alone (rare; seldom effective alone) OR Allogeneic HCT in appropriate candidates |
| Post-HCT | TKI maintenance (post-HCT TKI maintenance standard) Consider allogeneic HCT + post-HCT TKI when feasible |
Maintenance — Ph+ B-ALL
- TKI maintenance (preferred for those not proceeding to HCT).
- May include: vincristine, corticosteroids, IT therapy in addition to TKI.
- Duration: typically 2–3 years total therapy duration (protocol-specific).
Clinical Pearls
- Key 2024 trial: Jabbour et al., JAMA 2024 — supports MRD-driven TKI strategies; reference cited in v1.2026 footnotes for TKI selection guidance.
- Blinatumomab + TKI is now preferred in consolidation for MRD+ Ph+ B-ALL AND should be considered for MRD-negative patients not previously treated with blinatumomab.
- MRD qPCR BCR::ABL1 positivity in Ph+ ALL: may reflect persistence in myeloid compartment (residual CML clone). Where feasible, sort myeloid vs. lymphoid cells for FISH/NGS to distinguish.
- Ponatinib dose reduction to 15 mg/day once MRD negativity is achieved has shown similar efficacy with reduced toxicity — important to flag at tumor board.
- Imatinib in frontline Ph+ ALL: NCCN now explicitly restricts imatinib use to patients who CANNOT tolerate broader-acting TKIs.
Ph− B-ALL TREATMENT (NCCN ALL-5 | ALL-D 10–15 of 29)
Induction — Ph− B-ALL (AYA & Adults)
| Category (AYA/Adults <65 yrs) | Regimens |
|---|---|
| Preferred | Clinical trial Pediatric-inspired regimens (e.g., CALGB 10403, DFCI, COG-based for AYA) HyperCVAD (MD Anderson) |
| Other Recommended (High Intensity) | Linker 4-drug regimen BFM-based multiagent regimens |
| Other Recommended (Moderate) | Modified BFM with liposomal cytarabine for older adults |
| CD20+ B-ALL | Add rituximab to induction/consolidation (CD20 >20%) |
HyperCVAD Regimen — Key Pharmacotherapy Details
| Cycle Type | Drugs | Standard Doses |
|---|---|---|
| Odd cycles (A): 1,3,5,7 | Hyperfractionated Cyclophosphamide Vincristine Doxorubicin (Adriamycin) Dexamethasone | Cyclophosphamide 300 mg/m² IV q12h × 6 doses (days 1–3) Vincristine 2 mg IV days 4, 11 Doxorubicin 50 mg/m² IV day 4 Dexamethasone 40 mg PO/IV days 1–4, 11–14 |
| Even cycles (B): 2,4,6,8 | High-dose Methotrexate Cytarabine | Methotrexate 1 g/m² IV over 24h day 1 (with leucovorin rescue) Cytarabine 3 g/m² IV q12h × 4 doses days 2–3 (1 g/m² if age >60 or CrCl issues) |
| IT therapy | IT methotrexate and/or cytarabine | IT MTX 12 mg + IT Ara-C 100 mg each cycle; total CNS prophylaxis per protocol |
Leucovorin rescue (MTX cycles): MUST be on schedule. Typically leucovorin 15–25 mg PO/IV q6h starting 12–24h after MTX infusion completion until MTX level <0.05–0.1 µmol/L. Monitor MTX levels.
High-dose cytarabine (≥1 g/m²): Steroid eye drops (prednisolone 1% or dexamethasone) BID from day of cytarabine through 48h after LAST dose — prevents cytarabine-induced keratoconjunctivitis. NON-NEGOTIABLE.
Cytarabine dose reduction in elderly (>60 yrs) or renal impairment: reduce to 1 g/m² — severe neurotoxicity (cerebellar) risk.
Vincristine: 2 mg CAP (most institutions). Do NOT exceed 2 mg regardless of BSA. Peripheral neuropathy monitoring.
Doxorubicin: Cumulative lifetime dose limit (~450–550 mg/m²). Track running total. Baseline and serial ECHO.
CALGB 10403 (Pediatric-Inspired) — Key Features
- AYA population (ages 17–39). 5-yr OS ~73% vs ~46% with adult regimens (major trial).
- Includes pegaspargase (core component), not in traditional adult regimens.
- Induction: prednisone, vincristine, daunorubicin, pegaspargase + IT methotrexate.
- Consolidation: high-dose MTX, MP, 6-MP, IT therapy.
- Maintenance: 6-MP daily, MTX weekly, vincristine/prednisone monthly pulses × 2 years.
Rituximab in CD20+ Ph− B-ALL
- GRAALL-2005 trial: Rituximab 375 mg/m² added to induction/consolidation in CD20+ (>20%) Ph− B-ALL → significantly improved event-free survival in adults ≤60 yrs.
- NCCN: addition of rituximab should be considered in CD20-positive (>20% of blasts) B-ALL.
- Dose: 375 mg/m² IV, timing per protocol. Premedication: acetaminophen + diphenhydramine.
- Monitor: HBV reactivation (screen all patients; prophylaxis with entecavir if HBsAg+ or anti-HBc+ with low anti-HBs).
Consolidation — Ph− B-ALL
- Continuation of multiagent chemotherapy (high-dose MTX, ara-C, asparaginase, cyclophosphamide-based).
- Blinatumomab: may be incorporated for MRD+ disease (data from BLAST trial and others).
- Inotuzumab ozogamicin (InO): primarily relapsed/refractory setting; can be used as bridge to HCT.
- Allogeneic HCT: strongly favored for poor-risk cytogenetics and/or MRD positivity post-consolidation.
Maintenance — Ph− B-ALL
| Drug | Standard Dose | Duration | Monitoring |
|---|---|---|---|
| 6-Mercaptopurine (6-MP) | 50–75 mg/m² PO daily (adjust to target ANC 1.5–3.0×10⁹/L) | 2–3 years total (per protocol) | CBC weekly initially → q2-4 weeks; LFTs; TPMT/NUDT15 genotype before starting |
| Methotrexate (oral) | 20 mg/m² PO weekly | 2–3 years | CBC, LFTs; hold for oral mucositis; hold if significant transaminase elevation |
| Vincristine | 1.5 mg/m² IV (2 mg cap) monthly | 2 years (per protocol) | Neuropathy assessment; constipation prophylaxis (stool softeners/bowel regimen) |
| Prednisone/Dexamethasone | Prednisone 40 mg/m²/day (or dex equivalent) × 5 days monthly | 2 years (per protocol) | Blood glucose, BP, bone density (long-term); GI prophylaxis (PPI) |
Pharmacist Watchout (6-MP Maintenance)
- TPMT/NUDT15 genotyping BEFORE starting 6-MP: poor metabolizers → risk of fatal myelosuppression at standard doses. NCCN/CPIC recommend dose reduction (50–90%) in intermediate/poor metabolizers.
- 6-MP must be taken on EMPTY STOMACH (food reduces absorption by ~27%). Counsel patients to take at bedtime, 1–2h after last meal, with water only.
- 6-MP + allopurinol: DANGEROUS interaction — allopurinol inhibits xanthine oxidase (6-MP metabolism) → 6-MP levels increase 3–4x. REDUCE 6-MP dose by 75% if co-prescribed (rare; avoid if possible).
- 6-MP + milk/dairy: xanthines in milk may slightly reduce absorption. Separate by 1 hour.
- Oral MTX weekly: hold if active mucositis, vomiting, or transaminases >3x ULN. Resume at lower dose after resolution.
- Monitor CBC at EVERY cycle — myelosuppression is the dose-limiting toxicity of maintenance.
T-ALL TREATMENT (NCCN ALL-6 | ALL-D 17–22 of 29)
Induction — T-ALL (AYA & Adults)
| Category | Regimen |
|---|---|
| Preferred | Clinical trial Pediatric-inspired regimens (AYA) HyperCVAD (adults) |
| Other Recommended | ECOG-based multiagent regimens Nelarabine-containing regimens (T-ALL specific — category 2B for frontline; preferred in relapse) |
| Nelarabine Addition | Nelarabine 650 mg/m²/day IV days 1–5 (pediatric inspired) or protocol-specific dosing. Addition to standard induction/consolidation; associated with improved OS in some T-ALL subsets. |
Nelarabine — Key Pharmacotherapy
- MOA: Prodrug of 9-β-D-arabinofuranosylguanine (ara-G) — T-cell selective due to high expression of deoxyguanosine kinase.
- Dose: Adults 1500 mg/m² IV over 2h on days 1, 3, 5 (q21 days). Pediatric: 650 mg/m²/day × 5 consecutive days.
- CNS toxicity: Major concern — somnolence, confusion, seizures, peripheral neuropathy, ascending neuropathy (Guillain-Barré-like syndrome). Hold for neurotoxicity Grade ≥2.
- NEVER administer intrathecally.
- Myelosuppression: Monitor CBC closely.
- Adequate hydration required.
Consolidation — T-ALL
- Continuation multiagent chemotherapy with T-ALL specific intensification.
- Nelarabine: incorporated in some consolidation cycles.
- Allogeneic HCT: Strongly considered for ETP-ALL, MRD+ post-induction, relapsed disease.
- No approved targeted agents specific for T-ALL frontline (unlike B-ALL with blinatumomab/InO).
Maintenance — T-ALL
- 6-MP 75 mg/m² PO daily + oral MTX 20 mg/m² weekly.
- Monthly vincristine + prednisone pulses.
- Nelarabine may be incorporated (protocol-specific).
- CNS prophylaxis continues throughout.
Clinical Pearls
- ETP-ALL requires very close MRD monitoring — even a slight MRD positivity post-induction should prompt early allogeneic HCT discussion at tumor board.
- Nelarabine neurotoxicity is cumulative and can be severe — progressive peripheral neuropathy or encephalopathy → HOLD immediately. Inform the team proactively during rounds.
- Mediastinal mass in T-ALL: DO NOT biopsy under general anesthesia without airway assessment — airway collapse risk. Low-dose steroids may be used for cytoreduction. Keep patient in upright position.
- T-ALL does NOT express CD19/CD22 — therefore blinatumomab (anti-CD19) and inotuzumab ozogamicin (anti-CD22) are NOT applicable in frontline T-ALL.
- CD38 expression in T-ALL: daratumumab investigated (relapsed/refractory setting — category 2B per NCCN). Not frontline standard.
RELAPSED / REFRACTORY ALL (NCCN ALL-8 | ALL-D 24–29 of 29)
Relapsed/Refractory Ph+ B-ALL
| Category | Options |
| Preferred | Clinical trial Blinatumomab ± TKI Ponatinib-based regimen (especially T315I mutation) Asciminib +/- TKI (if multiple TKI intolerance, Cat 2B) |
| Other Recommended | HyperCVAD + TKI (switch TKI based on mutation profile) MOpAD regimen + TKI ± rituximab (CD20+) Steroids + TKI CAR T-cell therapy (if eligible) Allogeneic HCT after salvage CR |
| Post-Salvage | Allogeneic HCT preferred if CR2 achieved |
Relapsed/Refractory Ph− B-ALL
| Agent/Regimen | Class/MOA | Key Notes |
| Blinatumomab (BLINCYTO®) | BiTE (CD19×CD3 bispecific T-cell engager) | Preferred in R/R B-ALL. 28-day continuous IV infusion via pump. CRS management crucial. Cytoreduction if blasts ≥15,000/µL. See toxicity section. |
| Inotuzumab Ozogamicin (Besylomi®) | Anti-CD22 ADC (calicheamicin payload) | SOS/VOD risk — critical pre-HCT consideration. Avoid double-alkylator conditioning. Monitor LFTs/bilirubin. |
| Tisagenlecleucel (Kymriah®) | CD19-directed CAR T-cell | Ages ≤25 yrs (FDA-approved). 1-time infusion. CRS, ICANS, cytopenia management. Lymphodepletion (fludarabine + cyclophosphamide) required. |
| Brexucabtagene Autoleucel (Tecartus®) | CD19-directed CAR T-cell | Adults with R/R B-ALL. 1-time infusion after lymphodepletion. CRS, ICANS risk. |
| Obecabtagene Autoleucel (Aucatzyl®) | CD19-directed CAR T-cell | Adults with R/R B-ALL. 1-time infusion. Added to NCCN as option. |
| Augmented HyperCVAD | Intensified chemotherapy | Intensified vincristine, pegaspargase, dexamethasone alternating with HD MTX/Ara-C |
| Clofarabine ± combinations | Purine nucleoside analog | Monitor LFTs closely; hepatotoxicity; myelosuppression. Intensive supportive care required. |
| FLAG-IDA | Fludarabine, cytarabine, G-CSF ± idarubicin | MRD monitoring essential; bridging to HCT |
| Revumenib | KMT2A/menin inhibitor | KMT2A-rearranged ALL; differentiation syndrome monitoring |
| Venetoclax combinations | BCL-2 inhibitor | mini-hyperCVD + venetoclax; azacitidine + venetoclax; emerging data in R/R Ph-negative B-ALL |
Relapsed/Refractory T-ALL
- PREFERRED: Clinical trial.
- Nelarabine ± etoposide/cyclophosphamide (key agent in R/R T-ALL).
- High-dose cytarabine-containing regimens.
- Venetoclax-containing regimens (nelarabine + venetoclax; mini-hyperCVD + venetoclax; HMA + venetoclax).
- Daratumumab-containing regimen (category 2B; targets CD38 expression in T-ALL).
- Revumenib: KMT2A-rearranged T-ALL.
- Bortezomib-containing regimen.
- MOpAD regimen (late relapse >3 yrs from initial diagnosis: consider same initial regimen).
- FLAG-IDA, clofarabine ± cyclophosphamide/etoposide
Clinical Pearls
- Late relapse (>3 yrs from initial diagnosis): NCCN guidance allows consideration of same regimen as initial therapy — discuss at tumor board.
- For E. coli asparaginase hypersensitivity: substitute ERW-rywn (recombinant Erwinia asparaginase). New v1.2026 IM dosing: 25 mg/m² Mon/Wed, 50 mg/m² Fri × 2 weeks.
- Inotuzumab + double-alkylator conditioning pre-HCT: STRONGLY DISCOURAGED due to catastrophic SOS/VOD risk. Flag this during HCT planning.
- CAR T-cell therapy bridging: patients often require bridging chemotherapy during manufacturing (3–4 weeks). Coordinate steroid use carefully — corticosteroids can impair CAR T-cell function. Minimize pre-infusion steroid exposure.
- Revumenib (menin inhibitor): approved for KMT2A-rearranged leukemia. Watch for differentiation syndrome (fever, hypoxia, pleural/pericardial effusion) — treat with dexamethasone.
- Blinatumomab: antiepileptic prophylaxis (dexamethasone is given before each cycle; levetiracetam for seizure-prone patients — ESPECIALLY patients with Down syndrome per v1.2026 update).
KEY AGENTS — DOSING, MONITORING & PHARMACIST WATCHOUTS
Blinatumomab (BLINCYTO®)
| Parameter | Details |
| MOA | BiTE antibody: binds CD19 (B-cell) and CD3 (T-cell) simultaneously → T-cell cytotoxicity against B blasts |
| Indication | R/R B-ALL (adults & peds ≥1 yr); MRD+ B-ALL; Ph+ consolidation (+ TKI) |
| Dose — R/R B-ALL | Induction cycle 1: 9 mcg/day × 7 days, then 28 mcg/day × 21 days (28-day continuous IV infusion). Subsequent cycles: 28 mcg/day × 28 days. Consolidation: 28 mcg/day × 28 days. |
| Dose — MRD+ (Ph+ consolidation) | 28 mcg/day continuous IV infusion × 28 days per cycle |
| Administration | Continuous IV infusion via ambulatory pump. Must use IV bag with specific stabilizer. Change bags per pharmacy/manufacturer instructions (every 24–96h depending on concentration). |
| Premedication | Dexamethasone 20 mg IV 1h prior to first dose of cycle and prior to step-up dosing (day 8 in cycle 1) |
| Cytoreduction threshold | Cytoreduction if blasts ≥15,000/µL before starting blinatumomab |
| CRS Management | Interrupt infusion; steroids; consider tocilizumab for severe CRS. Restart at reduced rate after resolution. |
| Neurological toxicity | Hold for Grade ≥3 neurological events; restart at 9 mcg/day after ≥7 days resolution. |
| Down syndrome | NEW v1.2026: Increased seizure risk — consider antiepileptic prophylaxis (e.g., levetiracetam). |
| Key Labs | CBC, LFTs, BMP, neurological assessment before each cycle |
Inotuzumab Ozogamicin (Besylomi® / Besponsa®)
| Parameter | Details |
| MOA | Anti-CD22 antibody conjugated to calicheamicin (DNA-damaging payload) — targeted delivery to CD22+ B blasts |
| Indication | R/R B-ALL (adults); bridge to allogeneic HCT |
| Dose | Cycle 1: 0.8 mg/m² day 1 + 0.5 mg/m² days 8 & 15 (total 1.8 mg/m²/cycle). Subsequent cycles (CR): 0.5 mg/m² days 1, 8, 15 (total 1.5 mg/m²/cycle). 28-day cycles. |
| Cytoreduction threshold | Consider cytoreduction if absolute blast count ≥10,000/µL (use hydroxyurea or steroids + vincristine) |
| SOS/VOD Risk | CRITICAL: Monitor bilirubin and liver enzymes closely. Highest risk: prior allogeneic HCT, >2 cycles, double-alkylator conditioning pre-HCT. Avoid double-alkylator conditioning. Consider ursodiol prophylaxis. |
| SOS Treatment | Defibrotide for inotuzumab-related SOS/VOD (per NCCN ALL-C) |
| Myelosuppression | Common; institutional antimicrobial prophylaxis recommended |
| Key Labs | LFTs, bilirubin (watch closely for SOS), CBC, coagulation |
| Post-HCT planning | Inform transplant team of prior InO exposure — avoid double alkylator conditioning |
Pharmacist Watchout (Inotuzumab Ozogamicin)
- SOS/VOD IS LIFE-THREATENING. Flag ALL patients receiving InO for upcoming allogeneic HCT at tumor board — DOUBLE ALKYLATOR CONDITIONING IS STRONGLY DISCOURAGED.
- Monitor bilirubin DAILY/EVERY-OTHER-DAY after InO in pre-HCT patients. Rising bilirubin = early SOS signal.
- Ursodiol prophylaxis: 300 mg PO TID should be considered (per institutional practice; evidence base in HSCT context).
- Defibrotide: only FDA-approved treatment for SOS/VOD. Early recognition and initiation are critical.
- InO + >2 cycles: SOS risk significantly increases — reassess benefit:risk at tumor board before additional cycles.
Asparaginase Products
| Product | Source | Dose / Route | Half-Life | Key Notes |
| Pegaspargase (Oncaspar®) | E. coli (PEGylated) | 2500 IU/m² IM or IV (vial = 3750 IU); DOSE CAPPED AT 1 VIAL (3750 IU) | 5–7 days (PEGylation extends activity) | Preferred first-line asparaginase. IV route preferred (NCCN). TDM recommended with low-grade reactions. |
| Calaspargase pegol-mknl (Asparlas®) | E. coli (PEGylated; different PEG linkage) | 2500 IU/m² IV; dose capped at 1 vial (3750 IU) | Longer than pegaspargase (~26 days) | Used in patients aged ≤21 yrs as substitution for more sustained activity (per v1.2026). IV only. |
| ERW-rywn (Rylaze®) | Erwinia chrysanthemi (recombinant) | 25 mg/m² IM Mon/Wed + 50 mg/m² IM Fri × 2 weeks (new v1.2026 schedule) | ~16 hrs (IM) | For E. coli asparaginase hypersensitivity. More frequent dosing required. IM injection only. Monitor nadir activity. |
Asparaginase Toxicity Management (NCCN ALL-C 3–5 of 6)
| Toxicity | Grade/Threshold | NCCN Recommended Action |
| Hypersensitivity / Allergy | Grade 1–2 (rash, flushing, urticaria, fever <38°C without bronchospasm) | Continue with premedication (hydrocortisone, famotidine, diphenhydramine/cetirizine, acetaminophen). TDM highly recommended if premedicating (masks neutralizing antibody reaction). |
| Anaphylaxis / Grade 3–4 Allergic Reaction | Grade 3 or 4 systemic | PERMANENTLY DISCONTINUE causative asparaginase. Switch to ERW-rywn. |
| Hyperglycemia | Grade 3 or higher | Hold asparaginase AND steroids until blood glucose regulated with insulin. Resume after control. |
| Hypertriglyceridemia | Grade 4 | Hold asparaginase until normalized. Resume after normalization. |
| Pancreatitis | Clinical or Grade ≥2 | Hold asparaginase. Assess severity. For severe or hemorrhagic pancreatitis: likely permanent discontinuation. For mild: may resume after full resolution (protocol-dependent). |
| Hepatotoxicity — Direct Bilirubin | ≤3.0 mg/dL: Continue 3.1–5.0 mg/dL: Hold until <2.0, then resume >5.0 mg/dL: Hold or discontinue; resume if <2.0 with dose reduction + close monitoring | Monitor LFTs and bilirubin before each dose |
| Hepatotoxicity — AST/ALT | Grade 3: Hold until Grade 1, then resume Grade 4: Hold until Grade 1 (if ≤1 week: resume; if >1 week: discontinue or very close monitoring) | Close monitoring essential |
| Coagulopathy / Thrombosis | Fibrinogen <50–100 mg/dL; AT deficiency; symptomatic DVT/PE | Replace fibrinogen (cryoprecipitate), AT (AT concentrate/FFP). Anticoagulation per institutional protocol. Consider primary VTE prophylaxis. |
| Cerebral sinus thrombosis | Neurological symptoms, headache | MRV/MRA imaging. Anticoagulation typically indicated. Multidisciplinary management. |
Pharmacist Watchout (Asparaginase)
- Asparaginase DOSE CAP: Both pegaspargase and calaspargase pegol-mknl are CAPPED AT 1 VIAL (3750 IU) regardless of BSA calculation. Flag any orders exceeding this.
- TDM (Therapeutic Drug Monitoring): If premedication used, TDM is HIGHLY RECOMMENDED because premedication masks neutralizing antibody reactions. Target nadir asparaginase activity >0.1 IU/mL.
- Silent inactivation: Neutralizing antibodies can develop silently without clinical allergy → TDM is the only way to detect. If activity <0.1 IU/mL: switch product.
- Anticoagulation prophylaxis: NCCN recommends considering prophylaxis if no contraindications — asparaginase causes thrombosis via AT, fibrinogen, protein C/S depletion.
- Coagulation panel (PT/aPTT/fibrinogen/AT) BEFORE each asparaginase dose. Flag AT <50% — may require supplementation.
- Pancreatitis: Amylase/lipase elevation even without symptoms (asymptomatic hyperamylasemia) — do NOT automatically hold. Only hold for symptomatic pancreatitis or Grade ≥2.
- ERW-rywn IM scheduling: Monday 25 mg/m², Wednesday 25 mg/m², Friday 50 mg/m² × 2 weeks (updated v1.2026). Ensure IM site rotation; large volumes may need to be divided.
- ONLY use in SPECIALIZED CENTERS with expertise in ALL management.
CAR-T Cell Therapy
| Agent | Indication | Lymphodepletion | Key Toxicities & Management |
| Tisagenlecleucel (Kymriah®) | Pediatric/AYA ≤25 yrs, R/R B-ALL | Fludarabine 25 mg/m²/day × 3 days + cyclophosphamide 900 mg/m² × 1 day (days −4 to −2) | CRS (tocilizumab ± steroids), ICANS (steroids, levetiracetam), prolonged cytopenias, B-cell aplasia (IVIG replacement), infections |
| Brexucabtagene autoleucel (Tecartus®) | Adults with R/R B-ALL | Fludarabine 30 mg/m²/day × 3 + cyclophosphamide 500 mg/m²/day × 3 | CRS, ICANS, cytopenias, HLH/MAS, infections |
| Obecabtagene autoleucel (Aucatzyl®) | Adults with R/R B-ALL | Protocol-specified lymphodepletion | CRS, ICANS, cytopenias |
Clinical Pearls (CAR-T Cell)
- Pre-infusion steroid exposure should be MINIMIZED — corticosteroids (except for CRS/ICANS management) can impair CAR T-cell expansion and efficacy.
- Tocilizumab should be available AT BEDSIDE for the first 24h post-infusion per institutional requirement. Pharmacy must ensure availability.
- B-cell aplasia after CAR T-cell therapy is expected and may be PERMANENT — patients require IVIG replacement (IVIg q3–4 weeks to maintain IgG levels) and infection prophylaxis.
- Manufacturing time: 3–4 weeks (apheresis to infusion). Bridging chemotherapy is often needed. Plan ahead.
- CRS grading: ASTCT criteria used (Lee criteria in older literature). Tocilizumab first-line for Grade ≥2 CRS; steroids for ICANS.
- NCCN now refers to NCCN Guidelines for Management of CAR T-Cell and Lymphocyte Engager-Related Toxicities (name updated v1.2026).
MEASURABLE (MINIMAL) RESIDUAL DISEASE (MRD) (NCCN ALL-F)
12.1 MRD Assessment Methods
| Method | Sensitivity | Application |
| Multiparameter flow cytometry (MFC) | 10⁻⁴ | Standard method; widely available; requires baseline for leukemia-specific phenotype |
| RT-PCR (BCR::ABL1 quantitative) | 10⁻⁵–10⁻⁶ | Ph+ ALL only; gold standard for molecular MRD; p190 vs p210 must be tracked consistently |
| NGS-based (Ig/TCR clonotyping) | 10⁻⁶ | PREFERRED FDA-approved method (NCCN preferred) — detects clonal Ig/TCR rearrangements; does NOT require patient-specific primers. E.g., Adaptive clonoSEQ |
| ASO-PCR | 10⁻⁵ | Requires patient-specific primers from baseline sample; highly sensitive but labor-intensive |
12.2 MRD Interpretation & Clinical Action
- Preferred MRD method (NCCN v1.2026): FDA-approved NGS-based assay for Ig/TCR rearrangements, if available.
- MRD+ after induction: STRONG indication for intensification and/or allogeneic HCT consideration.
- Increasing MRD frequency of monitoring: useful for molecular relapse or low-level disease; and for Ph+ ALL patients discontinuing TKI.
- BCR::ABL1 qPCR positivity: may reflect persistence in myeloid compartment (residual CML clone) — not necessarily ALL relapse. Flow-sort myeloid vs. lymphoid cells for FISH/NGS to clarify when feasible.
- MRD negativity before allogeneic HCT: associated with better post-HCT outcomes. Therapy aimed at eliminating MRD before HCT is preferred.
- Referral: Given complexity of MRD management — NCCN recommends referral to/consultation with center with expertise for any ALL patient with MRD positivity.
| 🔑 Clinical Pearls — MRD MRD assessment time points MATTER — different regimens have different optimal MRD assessment time points (end of induction, after consolidation blocks). Always refer to the specific protocol being used.NGS MRD is now the PREFERRED method per NCCN v1.2026 — it uses broad primers (no patient-specific setup) and achieves 10⁻⁶ sensitivity.Flow cytometry MRD: requires a baseline (diagnostic) sample to characterize the leukemia-specific immunophenotype for subsequent comparison. If baseline was not sent, sensitivity and accuracy decrease.MRD+ post-induction in Ph+ ALL: ABL1 KD mutation testing may be less sensitive at low disease burden — do not rely solely on mutation testing when MRD is minimal. |
13. RESPONSE ASSESSMENT CRITERIA (NCCN ALL-E)
| Response | Definition |
| Complete Remission (CR) | <5% blasts in BM by morphology + no extramedullary disease + peripheral blood count recovery (ANC ≥1.0×10⁹/L, platelets ≥100×10⁹/L) |
| CR with Incomplete Hematologic Recovery (CRi) | <5% blasts + no extramedullary disease + incomplete peripheral blood count recovery (ANC <1.0 or Plt <100) |
| CR with Partial Hematologic Recovery (CRh) | <5% blasts + no extramedullary disease + partial count recovery (ANC ≥0.5, Plt ≥50) |
| Morphologic Leukemia-Free State (MLFS) | <5% blasts in BM with indeterminate peripheral blood recovery (e.g., in aplasia post-therapy) |
| No Response (NR) | ≥5% blasts in BM or persistent extramedullary disease |
| Progressive Disease (PD) | Increasing blast % or new extramedullary disease |
| MRD-negative CR | CR criteria met + MRD below detection threshold by sensitive method (NGS/PCR/flow) |
Count recovery per protocol is recommended BEFORE transitioning to post-remission therapy, even in the presence of MRD negativity. If count recovery is not achieved, assess for myelosuppression secondary to TKI and consider dose reduction.
14. ALLOGENEIC HEMATOPOIETIC CELL TRANSPLANT (ALL-G)
14.1 Indications for Allogeneic HCT in ALL
- Poor-risk cytogenetics (hypodiploid, KMT2A-rearranged, Ph+ with IKZF1plus, complex karyotype, Ph-like).
- MRD positivity after induction/consolidation (slow/incomplete MRD clearance).
- ETP-ALL with MRD positivity post-induction.
- CR2 or beyond (relapsed ALL achieving second remission).
- Ph+ ALL: Consider in MRD+ patients; patients ≤21 yrs achieving MRD negativity may not need HCT (data support chemo + TKI).
- Early transplant evaluation and donor search: NCCN strongly recommends consideration at diagnosis for all high-risk patients (updated ALL-3 v1.2026).
14.2 Post-HCT Considerations
- Post-HCT TKI maintenance: Standard for Ph+ ALL after allogeneic HCT. Typically dasatinib or ponatinib.
- Post-HCT MRD monitoring: Increased frequency monitoring (especially for Ph+ ALL patients discontinuing TKI).
- Germline testing: Hereditary ALL predisposition variants may impact HCT DONOR selection — expeditious germline testing before HCT is important (updated ALL-A v1.2026).
- Defibrotide: available for SOS/VOD (can occur after HCT, especially in prior InO-treated patients).
| ⚠️ CRITICAL PHARMACIST WATCHOUT: Pre-HCT Planning in ALL Inotuzumab ozogamicin history → flag at tumor board before HCT conditioning planning. DOUBLE ALKYLATOR CONDITIONING STRONGLY DISCOURAGED due to catastrophic SOS/VOD risk.CAR T-cell manufacturing logistics: coordinate with apheresis, pharmacy, and transplant team. Bridging therapy must be carefully selected to avoid compromising CAR T fitness.Germline testing BEFORE HCT: if pathogenic germline variant identified (e.g., TP53, PAX5, ETV6, RUNX1) → may affect donor selection (avoid donor with same variant in related donors).Post-HCT TKI: ensure TKI is ordered and insurance-approved before discharge. Engraftment + TKI = standard of care in Ph+ ALL. |
15. PRINCIPLES OF SUPPORTIVE CARE (NCCN ALL-C)
15.1 Antiemesis
- Highly emetogenic chemotherapy (HEC: e.g., high-dose cyclophosphamide, high-dose cytarabine, cisplatin combinations): 3–4 drug prophylaxis (5HT3 RA + NK1 RA + dexamethasone + olanzapine).
- Moderately emetogenic (MEC): 5HT3 RA + dexamethasone ± NK1 RA (per institutional protocol).
- Asparaginase: low emetogenic potential — premed as needed.
- Methotrexate (high-dose): MEC category — 5HT3 RA + dexamethasone.
- Note: Dexamethasone as antiemetic must be carefully considered when steroids are already part of ALL regimen (avoid duplication/excess steroid).
15.2 Infection Prophylaxis (NCCN ALL-C)
| Infection Type | Recommended Prophylaxis | Key Notes |
| PCP (Pneumocystis jirovecii) | TMP-SMX DS PO 3×/week (preferred) OR dapsone 100 mg/day OR inhaled pentamidine 300 mg q4 weeks OR atovaquone 1500 mg/day | Continue throughout immunosuppressive therapy. TMP-SMX: check G6PD before dapsone. Dapsone: avoid with G6PD deficiency. |
| Fungal (Antifungal prophylaxis) | Fluconazole 400 mg PO daily (prophylaxis during neutropenia) OR posaconazole 300 mg PO/IV daily (for high-risk: ≥7d neutropenia expected) | Fluconazole: CYP2C9/3A4 interactions (major). Posaconazole: CYP3A4 strong inhibitor — TKI interactions! Voriconazole: strong CYP3A4 inhibitor — significant dasatinib/ponatinib interaction. Check all drug interactions. |
| HSV/VZV prophylaxis | Acyclovir 400 mg PO BID OR valacyclovir 500 mg PO daily | Continue for duration of immunosuppression and 3–6 months post-completion |
| HBV reactivation | Screen all patients: HBsAg, anti-HBc, anti-HBs. If HBsAg+ or anti-HBc+: entecavir or tenofovir prophylaxis | Especially important with rituximab. Prophylaxis continues 6–12 months post-therapy. |
| CMV (post-HCT) | Letermovir prophylaxis (CMV-seropositive recipients), or preemptive monitoring/treatment | Post-HCT management per transplant protocol |
| Bacterial (during aplasia) | Fluoroquinolone prophylaxis (levofloxacin/ciprofloxacin) during prolonged neutropenia per institutional protocol | Risk of fluoroquinolone resistance development with prolonged use |
| ⚠️ PHARMACIST WATCHOUT: Drug Interactions in ALL Prophylaxis + TKIs Posaconazole/voriconazole + dasatinib/nilotinib/ponatinib: MAJOR interaction — azole antifungals are potent CYP3A4 inhibitors → significantly increase TKI levels → toxicity. Flag and notify oncology team. Consider dose reduction of TKI per PKI-specific labeling, or switch to fluconazole (weaker CYP3A4 effect).Fluconazole + nilotinib: fluconazole significantly inhibits CYP2C9 and CYP3A4 → may increase nilotinib exposure + QTc prolongation risk. Monitor ECG.TMP-SMX: can cause myelosuppression (folate antagonism) — may confound maintenance myelosuppression from MTX/6-MP. Monitor CBC.Acyclovir: dose adjust for renal impairment. During high-dose MTX cycles, ensure adequate hydration to prevent both MTX and acyclovir nephrotoxicity. |
15.3 Tumor Lysis Syndrome (TLS) Prophylaxis
- High TLS risk: ALL with high WBC or bulky disease.
- Allopurinol 300 mg/day PO starting 24–48h before chemotherapy (first-line for prevention).
- Rasburicase (recombinant urate oxidase): Use for high-risk patients or established TLS (converts uric acid to allantois). CONTRAINDICATED in G6PD deficiency (hemolytic anemia risk). Check G6PD before use.
- IV hydration: 2–3 L/m²/day. Avoid alkalinization (unnecessary with rasburicase; may worsen calcium phosphate precipitation).
- Monitor: uric acid, K⁺, Ca²⁺, PO₄, creatinine q4–8h during high-risk period.
- Urinary alkalinization: historically used with allopurinol but generally not recommended with rasburicase. Avoid in hyperphosphatemia (Ca-phosphate precipitation risk).
15.4 Corticosteroid Toxicity Management
- Hyperglycemia (acute): Frequent blood glucose monitoring. Insulin sliding scale/correction doses. If dexamethasone-based: hyperglycemia more pronounced vs. prednisone.
- GI protection: PPI (omeprazole/pantoprazole) or H2 blocker for steroid-induced ulcer prophylaxis during induction.
- Avascular necrosis (AVN): Long-term complication of cumulative steroid exposure — especially in AYA. Symptom monitoring, DEXA scan, bone density.
- Mood/behavioral changes (neuropsychiatric): Common in pediatric/AYA population. Inform patients and families.
- Osteoporosis prophylaxis: Calcium + vitamin D during prolonged steroid therapy.
15.5 Nutritional Support
- Enteral or parenteral support: Consider for >10% weight loss.
- Asparaginase-related hypertriglyceridemia: Dietary fat restriction + pharmacological management (fibrates/omega-3s) as needed.
15.6 Growth Factor Support
- G-CSF (filgrastim/pegfilgrastim): Use per institutional protocol for severe or prolonged neutropenia after consolidation or maintenance cycles. Avoid during acute induction (may stimulate leukemic progenitors in some ALL subtypes — caution). Standard use post-intensification consolidation cycles.
- Pegfilgrastim: avoid if next cycle is within 14 days of administration.
- Erythropoiesis-stimulating agents (ESA): NOT routinely used in ALL given active disease/therapy.
16. ALL PHARMACOTHERAPY — QUICK REFERENCE DRUG TABLE
| Medication (Brand) | Class / Subclass / MOA | Clinical Pearls / Key Side Effects / Counseling Points |
| Vincristine (Vincasar®) | Vinca alkaloid / Antimitotic — binds tubulin → mitotic arrest | 2 mg IV CAP (adults). Vesicant — central line required. Peripheral neuropathy (dose-limiting; assess at every visit). Constipation — stool softener prophylaxis required. FATAL if given IT — multiple patient safety steps required. Never refrigerate. |
| Dexamethasone / Prednisone | Corticosteroid / Induces lymphoblast apoptosis via GR | Dexamethasone preferred in AYA (greater CNS penetration, less AVN at equivalent anti-tumor doses in some studies). Monitor glucose q6h during pulse. GI prophylaxis required. Taper after prolonged use to avoid adrenal insufficiency. |
| Daunorubicin (Cerubidine®) / Doxorubicin | Anthracycline / Intercalates DNA, inhibits topoisomerase II, generates ROS | Cumulative lifetime dose limits (doxorubicin: ~450–550 mg/m²; daunorubicin: ~550 mg/m²). Vesicant — extravasation = dexrazoxane antidote. Cardiotoxicity: serial ECHO monitoring. Red urine (normal — counsel patient). Myelosuppression. |
| Cyclophosphamide (Cytoxan®) | Alkylating agent / Cross-links DNA strands | MESNA required (hemorrhagic cystitis prevention). Urine output monitoring. Hyponatremia risk (SIADH). Nausea: pre-medications. Alopecia. Gonadotoxicity. |
| Methotrexate (systemic HD) | Antifolate / Inhibits DHFR → impairs DNA synthesis | Leucovorin rescue CRITICAL (timing per protocol). Monitor MTX levels. Creatinine and urine pH monitoring. Alkalinize urine to pH >7 for excretion. Renal toxicity risk. Mucositis. Drug interactions: NSAIDs ↑ MTX toxicity (avoid). |
| Methotrexate (IT) | Same MOA; direct CNS delivery | Age-based flat dosing (NOT BSA-based for adults: 12 mg IT). Arachnoiditis (transient). Leucovorin rescue NOT routinely given after IT dose (unless protocol specifies). Never administer with liposomal IT cytarabine on same day without specific protocol guidance. |
| Cytarabine (Ara-C) — Standard | Pyrimidine analog / Inhibits DNA polymerase → chain termination | Myelosuppression dose-limiting. Low-dose (SC) vs. high-dose (IV) — different toxicities. High-dose: cerebellar toxicity, keratoconjunctivitis — steroid eye drops mandatory. |
| Cytarabine (Ara-C) — High-Dose | Same MOA; higher drug exposure | Steroid eye drops (prednisolone 1% BID × 48h after last HD Ara-C dose). Dose reduce to 1 g/m² for age >60 or renal impairment. Cerebellar toxicity (ataxia, nystagmus) → HOLD immediately if suspected. |
| 6-Mercaptopurine (6-MP / Purinethol®) | Thiopurine / Inhibits purine synthesis → DNA incorporation → cell death | TPMT/NUDT15 genotype BEFORE starting. Take on EMPTY STOMACH. Allopurinol interaction — reduce dose by 75% if co-prescribed. Monitor CBC/LFTs q2–4wk. Hepatotoxicity, cholestasis. Azathioprine/6-MP duplication check. |
| Pegaspargase (Oncaspar®) | Asparaginase enzyme / Depletes circulating asparagine → protein synthesis inhibition in lymphoblasts | IV route preferred. Cap at 1 vial (3750 IU). Allergy screening before each dose. TDM recommended. Coagulation panel before each dose. Pancreatitis, hepatotoxicity, hyperglycemia, thrombosis/bleeding monitoring. See toxicity table. |
| Dasatinib (Sprycel®) | 2nd-gen BCR::ABL1 TKI + SRC kinase inhibition | 100 mg PO daily for ALL. QTc monitoring. Pleural effusion (may require diuretics or dose hold). CYP3A4 substrate — MAJOR azole interactions. Take without regard to food (avoid antacids). BMS within 2h of administration. |
| Ponatinib (Iclusig®) | 3rd-gen BCR::ABL1 TKI / STAMP inhibitor (pan-BCR::ABL1) | Active against T315I. Arterial occlusive events (ATE) — screen CV risk factors; dose-reduce to 15 mg once MRD negative. Hypertension, hepatotoxicity, pancreatitis. CYP3A4 substrate. Dose starting point: 30–45 mg/day → reduce per response. |
| Nilotinib (Tasigna®) | 2nd-gen BCR::ABL1 TKI | QTc prolongation — EKG before dosing and monitoring. Must be taken FASTING (2h before, 1h after food — food increases absorption and QTc risk). CYP3A4 substrate. Hyperglycemia, rash, pancreatitis. |
| Asciminib (Scemblix®) | STAMP inhibitor (BCR::ABL1 kinase + myristate pocket) | Category 2B in ALL (multiple TKI intolerance). Active against T315I (higher dose required: 200 mg BID). QTc monitoring. CYP3A4 substrate. |
| Blinatumomab (BLINCYTO®) | BiTE antibody construct / CD19×CD3 bispecific T-cell engager | Continuous IV infusion (ambulatory pump). Dexamethasone premeds. CRS/cytokine release monitoring. Neurological toxicity (confusion, seizures, aphasia — hold, restart at 9 mcg). Down syndrome: antiepileptic prophylaxis. Cytoreduction if blasts ≥15,000/µL. |
| Inotuzumab Ozogamicin (Besylomi® / Besponsa®) | ADC / Anti-CD22 + calicheamicin payload | SOS/VOD risk (fatal). Avoid double-alkylator conditioning pre-HCT. Monitor bilirubin closely. Ursodiol prophylaxis. Defibrotide for SOS. Cytoreduction if blasts ≥10,000/µL. |
| Nelarabine (Arranon®) | Purine nucleoside analog / Ara-G prodrug → T-cell selective cytotoxicity | T-ALL specific. Neurotoxicity (somnolence, encephalopathy, peripheral neuropathy, Guillain-Barré-like) — HOLD for Grade ≥2. Adequate hydration. Never IT. Myelosuppression. |
| Rituximab (Rituxan®) | Anti-CD20 monoclonal antibody / ADCC + complement-mediated cytotoxicity | CD20+ B-ALL (>20%). Infusion reactions — premedicate (acetaminophen + diphenhydramine). HBV reactivation risk — screen and prophylax. PML risk (progressive multifocal leukoencephalopathy) — rare. Neutropenia. |
| Tisagenlecleucel (Kymriah®) | CD19-directed CAR T-cell therapy (autologous) | CRS (tocilizumab), ICANS (steroids + levetiracetam), prolonged cytopenias, B-cell aplasia (IVIG). Minimize pre-infusion steroids. Manufacturing 3–4 weeks. For patients ≤25 yrs. |
| Revumenib (Revuforj®) | Menin inhibitor / Blocks MLL-menin interaction → differentiation | KMT2A-rearranged ALL. Differentiation syndrome: fever, dyspnea, edema, pleural/pericardial effusion → dexamethasone. QTc monitoring. CYP3A4 substrate. |
| Venetoclax (Venclexta®) | BCL-2 inhibitor / Restores apoptosis in BCL-2-overexpressing cells | Emerging in R/R ALL (combinations). TLS risk on initiation — ramp-up required (oncology team to follow heme TLS protocol). CYP3A4 substrate — MAJOR azole interactions. GI toxicity. |
| Defibrotide (Defitelio®) | Fibrinolytic/cytoprotective agent / Restores thrombofibrinolytic balance endothelially | ONLY FDA-approved treatment for SOS/VOD. 6.25 mg/kg IV q6h (25 mg/kg/day) × minimum 21 days. Monitor: bleeding, hypotension. Contraindicated with systemic anticoagulation (relative). Renal and hepatic dose adjustments not required. |
| Hydroxyurea (Hydrea®) | Ribonucleotide reductase inhibitor / Cytoreduction | Used for initial cytoreduction in hyperleukocytosis or pre-blinatumomab/InO cytoreduction. Not definitive therapy. Monitor CBC closely. Short half-life. |
17. KEY CLINICAL TRIALS — BRIEF SUMMARY
| Trial | Population | Intervention vs. Comparator | Key Results / Outcome |
| CALGB 10403 | AYA 17–39 yrs, Ph− ALL | Pediatric-inspired (COG AALL0434 regimen) vs historical adult regimens | 5-yr OS 73% vs 46% (historical adult). Demonstrated superiority of peds-inspired approach in AYA. Established benchmark. |
| GRAALL-2005 (Rituximab) | Adults ≤60 yrs, CD20+ Ph− B-ALL | Rituximab + chemotherapy vs chemotherapy alone | Improved event-free survival with rituximab (4-yr EFS 65% vs 52%). Rituximab now standard in CD20+ B-ALL. |
| BLAST Trial (Blinatumomab MRD+) | Adults with MRD+ B-ALL after consolidation | Blinatumomab (4 cycles) as consolidation | 78% achieved MRD negativity. Improved OS. Established blinatumomab in MRD+ B-ALL. |
| INO-VATE (Inotuzumab) | Adults R/R B-ALL | Inotuzumab ozogamicin vs standard salvage chemotherapy | CR/CRi 80.7% vs 29.4%. Improved OS. Established InO in R/R B-ALL. High SOS/VOD risk post-HCT noted. |
| ELIANA (Tisagenlecleucel) | Pediatric/AYA ≤25 yrs R/R B-ALL | Tisagenlecleucel (single infusion) | Overall remission rate 81%. 12-month EFS 50%. Established CAR T-cell in ≤25 yrs R/R B-ALL. |
| ZUMA-3 (Brexucabtagene) | Adults R/R B-ALL | Brexucabtagene autoleucel (single infusion) | Overall remission rate 71%. MRD negativity in 85% of responders. Established in adult R/R B-ALL. |
| PhALLCON (Ponatinib + chemotherapy) | Adults Ph+ ALL | Ponatinib + reduced-intensity chemotherapy vs imatinib + chemotherapy | Improved MRD negativity and survival with ponatinib. Ponatinib now preferred TKI over imatinib. (Jabbour et al., JAMA 2024 — cited in NCCN v1.2026) |
| COG AALL0031 (Dasatinib in peds Ph+) | Children/AYA Ph+ ALL | Chemotherapy + dasatinib (continuous) | Excellent outcomes without HCT in MRD− patients. Established TKI + chemo without mandatory HCT for MRD− ≤21 yrs. |
| AALL1231 (Nelarabine in T-ALL) | AYA/pediatric T-ALL | Backbone + nelarabine vs backbone alone | Improved DFS in standard-risk T-ALL with nelarabine addition. Supports nelarabine use in frontline T-ALL. |
| AALL1931 (ERW-rywn IM schedule) | Pediatric/AYA ALL, E. coli asparaginase hypersensitivity | ERW-rywn new IM schedule (25 mg/m² Mon/Wed, 50 mg/m² Fri × 2 wks) | Positive risk:benefit ratio. Supports new IM dosing schedule — incorporated in NCCN v1.2026. |
18. CRITICAL PHARMACIST WATCHOUTS — CONSOLIDATED
18.1 Chemotherapy Order Verification
- VINCRISTINE: Absolute cap = 2 mg IV. Check every order. Verify it is NOT ordered for IT administration (fatal error). Use vincristine-specific bags/overwraps per USP <797> and ISMP guidelines.
- HIGH-DOSE MTX: Leucovorin rescue timing is critical. MTX level monitoring at 24h, 48h, 72h post-infusion. Adequate urine alkalinization (pH >7) before and during infusion.
- HIGH-DOSE ARA-C (≥1 g/m²): Steroid eye drops order MUST be placed (prednisolone 1% or equivalent BID). Reduce to 1 g/m² for age >60 or CrCl <60 mL/min. Cerebellar symptom assessment.
- PEGASPARGASE: Verify dose does not exceed 1 vial (3750 IU). IV route preferred. Coagulation panel before each dose. Premedication orders if needed.
- CYCLOPHOSPHAMIDE: MESNA co-order verification at every cycle. Urine output monitoring every 4h during administration.
- BLINATUMOMAB: Dexamethasone premedication before cycle start and dose step-up. Continuous pump operation — check IV line integrity, pump programming, stabilizer compatibility.
18.2 Lab Monitoring Cutoffs (General Guidance — Always Verify per Protocol)
| Lab Parameter | Typical Hold/Action Threshold | Context |
| ANC | <500–1000/µL (hold myelosuppressive therapy/reduce dose per protocol) | Maintenance 6-MP/MTX: target ANC 1.5–3.0×10⁹/L for dose adjustment |
| Platelets | <50,000/µL (hold consolidation/maintenance agents typically) | Protocol-specific; some regimens hold at <75,000 |
| Creatinine / CrCl | CrCl <50: reduce/hold HD methotrexate, cytarabine adjustments | Check before each HD MTX cycle; methotrexate requires adequate renal clearance |
| Total Bilirubin | >3× ULN: hold asparaginase (>3.1 mg/dL), hold/reduce vincristine (>3.0 mg/dL hepatic) | Asparaginase-specific thresholds as per NCCN ALL-C |
| Direct Bilirubin | >3.0 mg/dL: continue Aspar | 3.1–5.0: hold until <2.0 | >5.0: hold or discontinue | SOS/VOD monitoring with InO |
| AST/ALT | Grade 3 (>5× ULN): hold asparaginase/6-MP | Grade 4 (>20× ULN): discontinue consideration | LFT monitoring each cycle |
| Fibrinogen | <100 mg/dL: consider cryoprecipitate replacement (especially with asparaginase) | DIC/coagulopathy monitoring |
| Uric Acid | >8 mg/dL (or >10 mg/dL in high-risk): rasburicase | otherwise allopurinol | TLS monitoring q8h during induction |
| Blood Glucose | >250–300 mg/dL Grade 3: hold asparaginase + steroids until controlled | Insulin management with endocrinology/pharmacy |
| Amylase/Lipase | Symptomatic elevation (Grade ≥2): hold asparaginase. Asymptomatic: monitor closely, do not auto-hold | Differentiate asymptomatic elevation from true pancreatitis |
| QTc | >480–500 ms: review all QTc-prolonging drugs; consider TKI hold/switch (nilotinib, ponatinib, asciminib) | EKG monitoring with QTc-prolonging TKIs |
| ECHO/LVEF | <50% or drop ≥10% from baseline: hold anthracyclines; cardiology consult | Serial monitoring during ALL therapy |
18.3 Critical Drug Interactions
| Drug Pair | Severity | Mechanism & Management |
| 6-MP + Allopurinol | CONTRAINDICATED / Severe | Allopurinol inhibits xanthine oxidase → 6-MP accumulates → fatal myelosuppression. Reduce 6-MP dose by 75% if unavoidable. Prefer febuxostat (enzyme not inhibited by febuxostat) OR avoid combination. |
| Azole antifungals (Posaconazole/Voriconazole) + Dasatinib/Nilotinib/Ponatinib | Major | Strong CYP3A4 inhibition → ↑ TKI exposure → toxicity. Use fluconazole or micafungin if possible. If azole required: reduce TKI dose per labeling/pharmacist guidance. |
| Methotrexate + NSAIDs | Major | NSAIDs ↓ renal excretion of MTX → MTX toxicity (mucositis, nephrotoxicity, myelosuppression). AVOID NSAIDs during HD MTX cycles. |
| Methotrexate + Trimethoprim (TMP-SMX) | Major | Additive folate antagonism → myelosuppression, mucositis. If TMP-SMX is PCP prophylaxis: hold during HD MTX cycles; restart after MTX clearance. |
| Dasatinib + Antacids (aluminum/magnesium-containing) | Moderate | Antacids ↑ gastric pH → ↓ dasatinib absorption. Separate dasatinib and antacids by ≥2 hours. |
| Nilotinib + Food | Major (pharmacokinetic) | Food ↑ nilotinib absorption by 80–112% → ↑ QTc + toxicity. Must take FASTING (2h before, 1h after meals). |
| Venetoclax + Strong CYP3A4 inhibitors (azoles) | Major | ↑ Venetoclax exposure significantly → severe TLS/myelosuppression risk. Dose reduce venetoclax by 75% with strong inhibitors. |
| Cyclophosphamide + QTc-prolonging agents | Moderate | Additive risk — screen medication list for QTc-prolonging drugs. |
| Corticosteroids + Vaccines (live) | Contraindicated during immunosuppression | Avoid live vaccines during active chemotherapy. MMR, varicella, zoster live vaccines contraindicated. |
19. SPECIAL POPULATIONS
19.1 Adults ≥65 Years or Substantial Comorbidities (NCCN ALL-D 3 of 29)
- Reduced-intensity regimens preferred: moderate-intensity multiagent, steroids + TKI.
- Avoid high-dose cytarabine (≥3 g/m²) — use 1 g/m²; omit or reduce asparaginase.
- TKI monotherapy (steroids + TKI): may be appropriate as induction for very frail/elderly Ph+ patients; CR rates reasonable.
- CNS prophylaxis: liposomal cytarabine IT may be an option in older patients (reduces treatment frequency).
- Anthracycline dose reduction for cardiac comorbidities — baseline ECHO essential.
- G-CSF support: more liberal use in elderly.
- Allogeneic HCT: consider for appropriate fit elderly individuals achieving remission (updated v1.2026).
- Safety of full-intensity R/R salvage regimens in adults ≥65 yrs not established — individualize.
19.2 AYA Patients (15–39 years)
- NCCN defines AYA as 15–39 years (not a firm cutoff — some regimens not tested across full range).
- Pediatric-inspired regimens (CALGB 10403, COG-based): significantly superior OS vs traditional adult regimens.
- Higher asparaginase tolerance vs. older adults — core component of AYA regimens.
- Fertility preservation: discuss gonadotoxicity before initiation. Refer to reproductive endocrinology when feasible. Sperm banking, oocyte/embryo cryopreservation.
- Long-term toxicities: avascular necrosis (cumulative steroids), neurotoxicity, cardiotoxicity (anthracyclines), secondary malignancies (alkylators).
- Psychosocial: refer to AYA oncology program/NCCN AYA guidelines.
19.3 Ph-Like (BCR::ABL1-Like) ALL
- ~20–25% of AYA/adult B-ALL — BCR::ABL1 NEGATIVE but gene expression profile similar to Ph+ ALL.
- Must use comprehensive NGS for identification — not detectable by standard FISH.
- Actionable fusions:
- JAK-STAT pathway (CRLF2r, JAK1/2r, EPORr): ruxolitinib (JAK1/2 inhibitor) sensitivity. Add ruxolitinib to induction/consolidation (clinical trial context preferred).
- ABL-class fusions (ABL1r, ABL2r, PDGFRAr, PDGFRBr, FGFRr): TKI-sensitive — dasatinib or ponatinib can be added.
- Currently, NCCN recommends clinical trial enrollment for Ph-like ALL when possible.
19.4 Down Syndrome ALL
- Increased sensitivity to methotrexate and cytarabine → requires dose adjustments.
- Increased risk of infections and treatment-related toxicity.
- NEW v1.2026: Increased risk of seizures with blinatumomab in Down syndrome patients — antiepileptic prophylaxis SHOULD BE CONSIDERED.
20. SURVEILLANCE (NCCN ALL-7)
| Time Point / Frequency | Recommended Assessments |
| During therapy (each cycle) | CBC with differential, CMP, LFTs, coagulation studies (esp. with asparaginase). MRD assessment per protocol time points. ECG for QTc-prolonging TKIs. |
| Post-induction CR | Bone marrow biopsy + MRD assessment. BCR::ABL1 qPCR (Ph+). Cytogenetics if needed. |
| End of consolidation | BM biopsy + MRD. Restaging imaging if extramedullary disease. Reassess HCT candidacy. |
| During maintenance | CBC q2–4 weeks (dose adjust 6-MP/MTX to target ANC). LFTs q1–3 months. MRD q3–6 months (protocol-dependent). |
| Post-therapy completion | CBC, LFTs, CMP q3 months × 2 yrs, then annually. Long-term: annual ECHO (anthracycline exposure), DEXA scan (steroids), neurocognitive assessment. Late toxicity surveillance per COG LTFU guidelines. |
| Ph+ ALL off TKI | Increased MRD frequency monitoring — monthly × 3 months, then q3 months. |
| Relapse surveillance | Any new cytopenias, symptoms → prompt BM evaluation. |
21. KEY PATIENT COUNSELING POINTS
Induction Phase Counseling
- Explain treatment phases (induction → consolidation → maintenance) and overall duration (~2.5–3 years).
- Infection precautions during neutropenia: hand hygiene, avoid crowds/sick contacts, no live vaccines.
- When to call/go to ER: fever >38°C (100.4°F) — IMMEDIATE — do not wait.
- Blood transfusion support: may need platelet/RBC transfusions during aplasia.
- Hair loss (alopecia): temporary; common with anthracyclines and cyclophosphamide.
- Contraception: avoid pregnancy during therapy (teratogenic drugs). Discuss fertility preservation BEFORE starting.
Maintenance Phase Counseling
- 6-MP: Take on EMPTY STOMACH at BEDTIME. Avoid dairy within 1 hour. Do not take with allopurinol without provider guidance.
- Weekly oral methotrexate: Take same day each week. Avoid alcohol (additive hepatotoxicity). Use reliable contraception.
- Continue PCP prophylaxis (TMP-SMX) throughout entire maintenance.
- Report: fatigue, unusual bruising/bleeding, jaundice, severe mouth sores, nausea/vomiting.
TKI Counseling (Ph+ B-ALL)
- Dasatinib: Take once daily; food does not significantly affect absorption. Avoid antacids within 2h. Monitor for dyspnea/peripheral edema (pleural effusion). Report immediately.
- Nilotinib: Take FASTING (2h before, 1h after meals). Strict adherence — food significantly increases exposure and QTc risk.
- Ponatinib: Once daily with or without food. Report chest pain, stroke symptoms (arterial events), jaundice (hepatotoxicity).
- Missed dose: do NOT double-dose. Take as soon as remembered if within same day; skip if close to next dose.
- TKIs interact with many OTC drugs and supplements — review ALL medications (including herbal/supplements) with pharmacist.
22. CONSOLIDATED CLINICAL PEARLS — PHARMACIST EDITION
| # | Domain | Clinical Pearl |
| 1 | Diagnosis | ETV6::RUNX1 is CRYPTIC by karyotype — always verify with FISH/PCR. Missing it changes risk stratification. |
| 2 | Diagnosis | BCR::ABL1 transcript type (p190 vs p210) matters for MRD monitoring — track consistently throughout therapy. |
| 3 | Risk Strat. | Near-haploid cells can DOUBLE and appear hyperdiploid — confirm with SNP array. Misclassification = under-treatment of poor-risk disease. |
| 4 | Risk Strat. | Ph-like ALL is actionable — MUST identify JAK-STAT vs ABL-class fusion for targeted therapy. NGS is required. |
| 5 | Ph+ ALL | Imatinib in frontline Ph+ ALL: RESTRICTED to patients intolerant of broader TKIs (per NCCN v1.2026). Dasatinib or ponatinib preferred. |
| 6 | Ph+ ALL | ABL1 KD mutation testing is less sensitive at minimal disease burden — interpret cautiously when MRD is low. |
| 7 | Ph+ ALL | Blinatumomab + TKI is now PREFERRED in consolidation for BOTH MRD+ AND MRD− Ph+ B-ALL (if not previously used). |
| 8 | Asparaginase | Dose CAP: 1 vial (3750 IU) regardless of BSA. Flag any orders exceeding this. |
| 9 | Asparaginase | TDM is HIGHLY RECOMMENDED when premedicating — premedication masks neutralizing antibodies. Target activity >0.1 IU/mL. |
| 10 | Asparaginase | Anticoagulation prophylaxis should be CONSIDERED with asparaginase — depletes fibrinogen, AT, protein C/S. |
| 11 | 6-MP | TPMT/NUDT15 genotyping BEFORE starting 6-MP — poor metabolizers have fatal myelosuppression risk at standard doses. |
| 12 | 6-MP | Take on EMPTY STOMACH at bedtime. Allopurinol interaction is SEVERE — reduce 6-MP by 75% if co-prescribed. |
| 13 | HD MTX | Leucovorin rescue timing is critical. NSAIDs and TMP-SMX increase MTX toxicity — HOLD during HD MTX cycles. |
| 14 | HD Ara-C | Steroid eye drops are NON-NEGOTIABLE with high-dose cytarabine. Place order proactively. |
| 15 | InO | SOS/VOD is life-threatening post-InO + allogeneic HCT. Double-alkylator conditioning STRONGLY DISCOURAGED. Flag at HCT planning. |
| 16 | Blinatumomab | Down syndrome patients: antiepileptic prophylaxis SHOULD BE CONSIDERED (NCCN v1.2026 update). Levetiracetam recommended. |
| 17 | CAR T-cell | Minimize corticosteroid use BEFORE CAR T-cell infusion — steroids impair CAR T expansion and efficacy. |
| 18 | Drug Interactions | Azole antifungals + TKIs = MAJOR CYP3A4 interaction. Alert the team and recommend dose adjustments or alternative antifungal. |
| 19 | TLS | Rasburicase CONTRAINDICATED in G6PD deficiency — check G6PD status before prescribing in high-TLS-risk patients. |
| 20 | MRD | NGS-based assay is now the PREFERRED MRD method per NCCN v1.2026. Understand the method used at your institution. |
| 21 | Supportive Care | Vincristine: NEVER in the refrigerator. NEVER IT. 2 mg CAP. Bowel regimen mandatory. |
| 22 | Supportive Care | PCP prophylaxis (TMP-SMX): Hold during HD MTX cycles — additive folate antagonism causes severe myelosuppression. |
| 23 | Transplant | Germline predisposition testing BEFORE HCT — pathogenic germline variants may affect DONOR selection. |
| 24 | Surveillance | Post-HCT TKI maintenance in Ph+ ALL: ensure TKI is ordered and approved at discharge — this is standard of care. |
| 25 | Counseling | Fever ≥38°C during neutropenia = MEDICAL EMERGENCY. Counsel every patient explicitly — do not wait, go directly to ER. |
ABBREVIATIONS
| Abbreviation | Meaning | Abbreviation | Meaning |
| ALL | Acute Lymphoblastic Leukemia | MRD | Measurable (Minimal) Residual Disease |
| AYA | Adolescent & Young Adult (15–39 yrs) | NGS | Next-Generation Sequencing |
| B-ALL | B-cell ALL | TKI | Tyrosine Kinase Inhibitor |
| T-ALL | T-cell ALL | HCT | Hematopoietic Cell Transplant |
| Ph+ | Philadelphia chromosome-positive (BCR::ABL1+) | IT | Intrathecal |
| CR | Complete Remission | HD MTX | High-Dose Methotrexate |
| CRi | CR with Incomplete Hematologic Recovery | 6-MP | 6-Mercaptopurine |
| ETP | Early T-cell Precursor | PEG | Pegaspargase (Oncaspar®) |
| SOS/VOD | Sinusoidal Obstruction Syndrome / Veno-Occlusive Disease | InO | Inotuzumab Ozogamicin |
| CRS | Cytokine Release Syndrome | BiTE | Bispecific T-cell Engager |
| ICANS | Immune Effector Cell-Associated Neurotoxicity Syndrome | TDM | Therapeutic Drug Monitoring |
| FISH | Fluorescence In Situ Hybridization | MPAL | Mixed Phenotype Acute Leukemia |
| BM | Bone Marrow | LP | Lumbar Puncture |
| CSF | Cerebrospinal Fluid | TLS | Tumor Lysis Syndrome |
| TPMT | Thiopurine S-methyltransferase | NUDT15 | Nudix hydrolase 15 (affects 6-MP metabolism) |
— END OF GUIDE —
Based on NCCN Clinical Practice Guidelines in Oncology — Acute Lymphoblastic Leukemia, Version 1.2026 (April 8, 2026)
For educational and pharmacotherapy reference use only. Always verify with current guidelines and institutional protocols.