Based on NCCN Guidelines v3.2026 | ELN 2022
OVERVIEW & EPIDEMIOLOGY
APL represents ~10% of all AML cases. It is a medical emergency due to life-threatening coagulopathy at presentation but curable if treated appropriately and promptly.
- Median age at diagnosis: 44 years (significantly younger than AML median of 67 years)
- Age-adjusted annual incidence: ~0.23/100,000 (NCI SEER 1992–2007)
- De novo APL and therapy-related APL (t-APL, less common) have similar clinicopathology and are managed identically
- t-APL: most common antecedent cancers are breast, hematologic malignancy, genitourinary; topoisomerase II inhibitors and RT carry highest risk;
t-APL remission rate ~80%
- t-APL: most common antecedent cancers are breast, hematologic malignancy, genitourinary; topoisomerase II inhibitors and RT carry highest risk;
- WHO 2022 classifies APL molecularly as ‘APL with PML::RARA’ (includes cryptic/complex rearrangements), not purely cytogenetic t(15;17)
💎 Clinical Pearl: APL is one of the few hematologic malignancies where early mortality is primarily driven by coagulopathy and differentiation syndrome — not disease burden. Starting ATRA immediately upon clinical suspicion is lifesaving.
PATHOPHYSIOLOGY
Cell originality
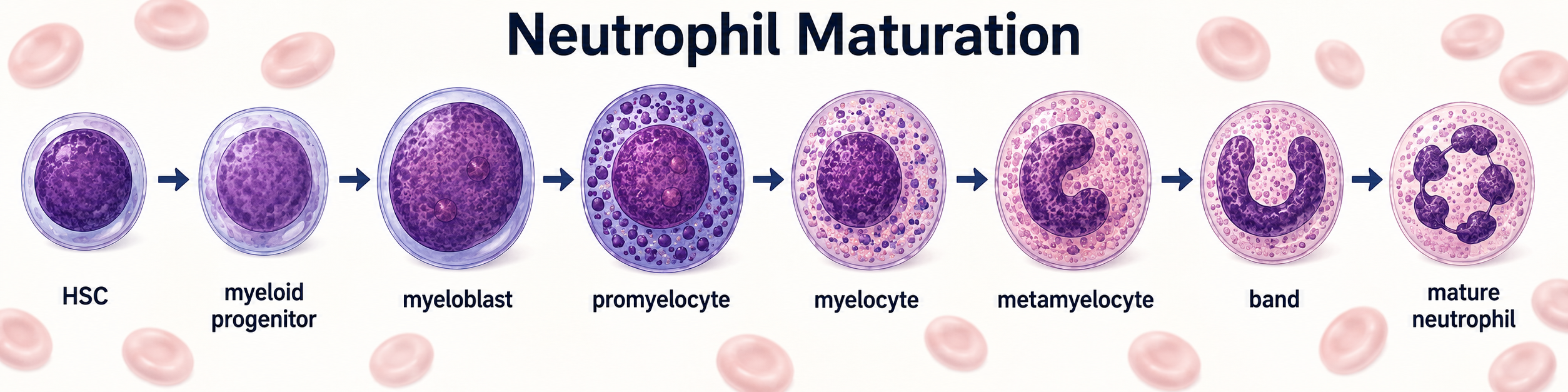

A promyelocyte is therefore not inherently malignant. It is a normal, temporary developmental stage.
In APL, the cell becomes genetically mutated and gets “stuck” at this point (immature white blood cells). This causes them to build up in the bone marrow and trigger a life-threatening, dual-natured bleeding and clotting disorder.
Promyelocytic Leukemia (PML) and Retinoic Acid Receptor Alpha (RARα) gene
PML (Promyelocytic Leukemia) gene acts as a tumor suppressor. It builds cellular structures that help regulate cell growth, prevent cancer, and control cell death.
RARA (Retinoic Acid Receptor Alpha) gene gives instructions for making a protein receptor that binds with retinoic acid (a form of Vitamin A). It tells your immature blood cells to grow up and mature into fully functioning white blood cells.
PML-RARA fusion causes the immature blood cells get “stuck” and never grow up, neither undergo apoptosis. These immature cells then multiply out of control, causing APL.
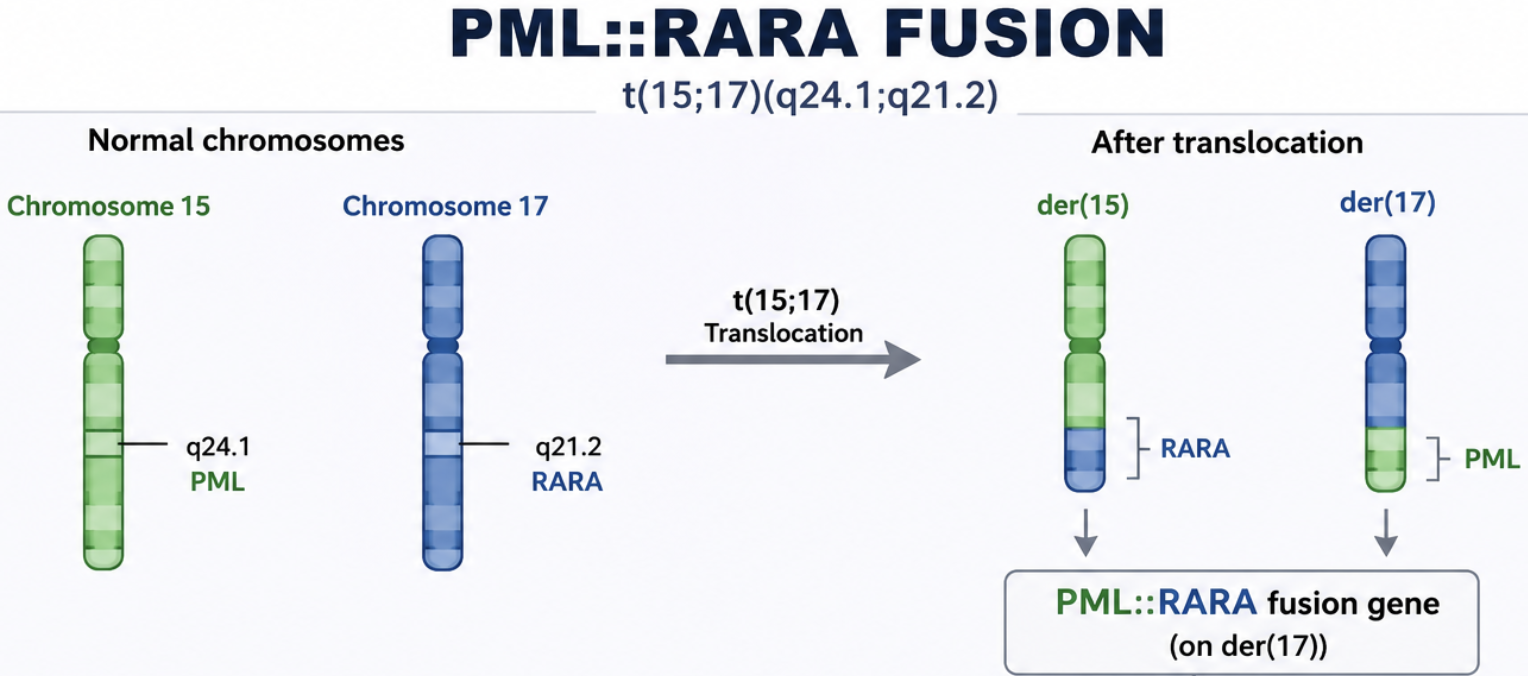
- The Translocation: t(15;17)
- The Fusion Gene: PML::RARA fusion gene, fuses the Promyelocytic Leukemia (PML) gene on chromosome 15 with the Retinoic Acid Receptor Alpha (RARA) gene on chromosome 17
Pathophysiology
- Maturation Arrest: The normal RARA gene helps immature promyelocytes mature into functional infection-fighting white blood cells (neutrophils) when exposed to retinoic acid (Vitamin A). [1, 2, 3, 4]
- Transcriptional Silencing: The PML::RARA fusion protein binds abnormally tightly to DNA. It recruits nuclear corepressors and histone deacetylases (HDACs), which lock down the genes responsible for maturation. [1, 2]
- Differentiation Block: Because they cannot mature, these promyelocytes are trapped in an immature, rapidly multiplying state and accumulate uncontrollably in the bone marrow and blood. [1]
What it Does: Clinical Effects & Coagulopathy
- Bone Marrow Failure (Pancytopenia): As the malignant promyelocytes crowd the bone marrow, the production of other essential blood cells drops. This leads to:
- Life-Threatening Clotting and Bleeding: The malignant promyelocytes themselves actively disrupt the body’s clotting system via two main mechanisms, often causing Disseminated Intravascular Coagulation (DIC):
- Widespread Clotting: The leukemia cells overexpress Tissue Factor (TF), which triggers the coagulation cascade to form excess thrombin and fibrin, setting off widespread, dangerous micro-clots throughout the body.
- Uncontrollable Bleeding (Hyperfibrinolysis): At the same time, the cells overexpress Annexin II, a protein that dissolves blood clots by converting plasminogen to plasmin. This simultaneous destruction of clots (while they are forming) leads to profound and often fatal internal bleeding, especially into the brain. [1, 2, 4]
APL is a medical emergency but is also considered one of the most highly curable forms of leukemia today. Targeted therapies like All-Trans Retinoic Acid (ATRA) (a form of Vitamin A) and Arsenic Trioxide (ATO) are used to break apart the PML::RARA protein, destroy the malignant cells, and force the immature promyelocytes to finally mature and die off. [1, 2, 3, 4, 5]
CLINICAL PRESENTATION & SIGNS/SYMPTOMS
Typical Presentation
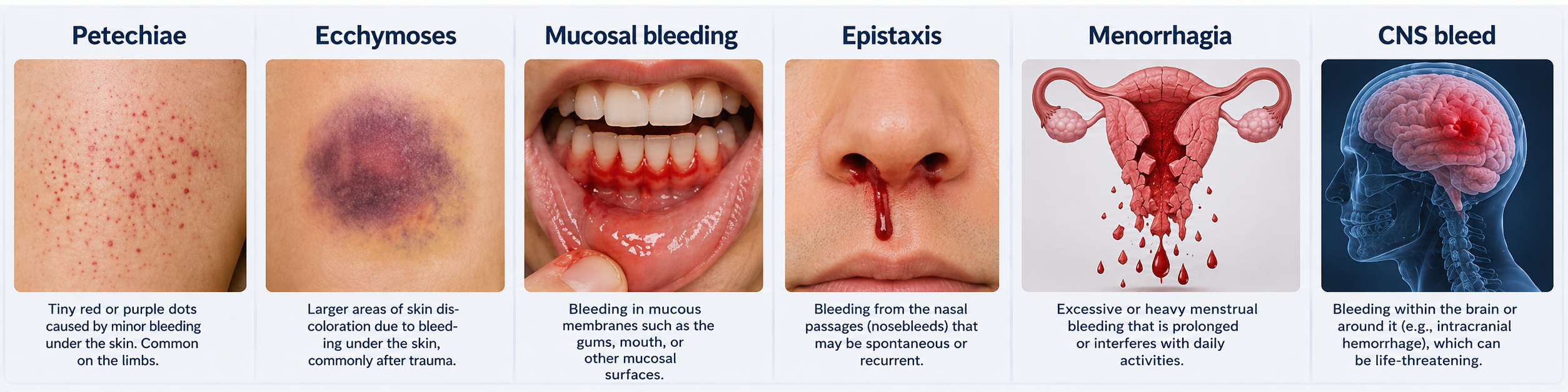
- Bleeding diathesis (most characteristic): petechiae, ecchymoses, mucosal bleeding, epistaxis, menorrhagia, CNS bleed
- DIC/coagulopathy screen positive: ↑ PT, ↑ PTT, ↓ fibrinogen, ↑ D-dimer, ↑ FDP
- Fatigue, pallor (anemia), fever (infection), bone pain
- Hyperleukocytosis: less common at presentation in APL vs other AML subtypes — but WBC > 10 ×10⁹/L = HIGH risk
- Thrombocytopenia disproportionate to anemia/leukopenia
Rare/Special Presentations
- CNS involvement: more common in HIGH-risk (WBC >10) — LP recommended before consolidation in high-risk patients
- Microgranular variant (FAB M3v): high WBC, less granularity, often misidentified — FISH/PCR essential
- t-APL may have biclonal/additional cytogenetic changes but behaves like de novo APL
⚠ PHARMACIST ALERT: If morphology + coagulopathy suggests APL: START ATRA IMMEDIATELY. Do NOT wait for FISH/PCR confirmation. If FISH/PCR ultimately negative → discontinue ATRA and initiate standard AML therapy.
DIFFERENTIAL DIAGNOSIS
- Other AML subtypes (particularly AML-M2 with t(8;21) which can also present with Auer rods)
- MDS with excess blasts transforming to AML
- Reactive promyelocytosis (e.g., G-CSF use, infections) — check morphology carefully; no PML::RARA
- DIC from other causes (sepsis, solid tumor) — lacks APL-specific morphology/cytogenetics
- MPAL or other acute leukemias of ambiguous lineage — immunophenotype and molecular testing essential
💎 Clinical Pearl: Key differentiator: Auer rods in BUNDLES (faggot cells) are virtually pathognomonic for APL. Auer rods appear in other AML subtypes but not in bundles. Confirm with FISH or RT-PCR for PML::RARA.
DIAGNOSIS & WORKUP
Morphology (BM Aspirate/Biopsy)
- Hypergranular promyelocytes with abundant azurophilic granules
- Bilobed or kidney-shaped nuclei
- Faggot cells (Auer rod bundles) — pathognomonic
- FAB classification: M3 (hypergranular) and M3v (microgranular/hypogranular variant)
📌 Note: NCCN recommendation: Initial diagnosis can be made on PERIPHERAL BLOOD to minimize invasive BM procedure during active coagulopathy. BM can wait until coagulopathy is controlled.
Cytogenetics / Molecular
- Conventional karyotype: t(15;17)(q24.1;q21.1)
- FISH: rapid turnaround, detects cryptic rearrangements
- RT-PCR for PML::RARA: gold standard; quantitative RT-PCR (RQ-PCR) used for MRD monitoring; sensitivity ≤10⁻⁴ recommended
- PML::RARA isoforms: BCR1 (long, intron 6), BCR2 (variant), BCR3 (short, intron 3) — all respond to ATRA; BCR3 more common in microgranular variant
Immunophenotype (Flow Cytometry)
- CD33+, CD13+, CD117+
- Typically HLA-DR⁻, CD34⁻ (distinguishes from other AML subtypes)
- CD11b⁻, CD16⁻ (immature granulocytes — differentiates from reactive promyelocytosis)
Additional Workup (NCCN-Recommended)
- CBC with differential, comprehensive metabolic panel
- Coagulation panel: PT, PTT, fibrinogen, D-dimer, FDP (daily until resolved)
- Type & screen, blood bank notification
- ECG for QTcF baseline before ATO initiation
- Electrolytes: Ca, K, Mg, Phosphorus, Creatinine (before and weekly during ATO)
- FLT3 mutation testing (ITD and TKD): prognostic in APL; FLT3-ITD associated with hyperleukocytosis and higher relapse risk but does NOT change front-line management
- LP: recommended ONLY for high-risk APL patients before consolidation (not routine for low-risk)
RISK STRATIFICATION (Sanz Score)
Risk in APL is based ENTIRELY on WBC and platelet count at diagnosis (Sanz Score). This drives treatment selection:
| Risk Group | WBC (×10⁹/L) | Platelet (×10⁹/L) |
| Low Risk | ≤10 | >40 |
| High Risk | >10 | Any |
- Low Risk: WBC ≤10 ×10⁹/L AND Platelets >40 ×10⁹/L
- High Risk: WBC >10 ×10⁹/L (regardless of platelet count)
- Intermediate Risk (original Sanz): WBC ≤10 AND Platelets ≤40 — NCCN v3.2026 groups with LOW RISK for treatment purposes
📌 Note: NCCN v3.2026 bifurcates treatment into LOW RISK (WBC ≤10) and HIGH RISK (WBC >10) only. The intermediate Sanz stratum is incorporated into low-risk treatment algorithms.
💎 Clinical Pearl: FLT3-ITD is associated with high WBC count (leukocytosis) and is thus enriched in the high-risk group, but it is NOT an independent treatment modifier in current NCCN guidelines for front-line APL. Do not let a positive FLT3 change your ATRA+ATO decision.
GENOMICS & CYTOGENETICS
Defining Alteration
- t(15;17)(q24.1;q21.1) → PML::RARA fusion: present in >98% of APL
- RARA fusion partners other than PML (rare): PLZF, NPM1, NuMA, STAT5b, BCOR — generally do NOT respond to ATRA; require alternative approaches
Co-occurring Mutations (Prognostic, Not Treatment-Changing)
- FLT3-ITD: 30–40% of APL; associated with hyperleukocytosis; slightly higher relapse risk but does not modify ATRA+ATO therapy
- FLT3-TKD: less common; similar association
- WT1 mutations: less prognostic relevance in APL vs other AML
- Trisomy 8: most common secondary cytogenetic change; not independently prognostic
MRD Marker
- PML::RARA by RQ-PCR is the validated MRD marker for APL (sensitivity ≤10⁻⁴; most clinical labs at 10⁻⁴)
- Peripheral blood is acceptable for surveillance once BM MRD-negativity is established
💎 Clinical Pearl: Unlike other AML, APL MRD monitoring is REQUIRED (not optional) and is the primary tool for relapse detection. Use the SAME laboratory for serial testing to ensure consistent assay sensitivity.
⚠ PHARMACIST ALERT: If the molecular test at diagnosis identifies a RARE fusion partner (PLZF::RARA, etc.) instead of PML::RARA — ATRA may NOT induce differentiation and standard AML therapy should be considered. Escalate immediately to attending.
PHARMACOTHERAPY MANAGEMENT
Induction & Consolidation Regimens (NCCN v3.2026)
| Regimen | Induction Dosing | Consolidation Dosing |
|---|---|---|
| ATRA + daily ATO (Low Risk, Cat 1) | ATRA 45 mg/m² PO in 2 divided doses daily + ATO 0.15 mg/kg IV daily | ATO 0.15 mg/kg/d IV 5d/wk × 4 wks q8wks × 4 cycles ATRA 45 mg/m²/d × 2 wks q4wks × 7 cycles |
| ATRA + intermittent ATO (Low Risk, Cat 1) | ATRA 45 mg/m² PO in 2 divided doses daily × 60d or until CR + ATO 0.3 mg/kg IV days 1–5 wk1, then 0.25 mg/kg 2×/wk wks 2–8 | 3 × 56-day cycles: ATRA 45 mg/m²/d days 1–14 & 29–42 + ATO 0.3 mg/kg d1–5 wk1, 0.25 mg/kg 2×/wk wks 2–4 4th cycle (28-day): ATRA × 14d + ATO as above |
| ATRA + Idarubicin (Low/High Risk, Cat 1) | ATRA 45 mg/m² + Idarubicin 12 mg/m² days 2,4,6,8 (days 2,4,6 if age >70y) | Cycle 1: ATRA ×15d + Idarubicin 5 mg/m² ×4d Cycle 2: ATRA ×15d + Mitoxantrone 10 mg/m²/d ×3d Cycle 3: ATRA ×15d + Idarubicin 12 mg/m² ×1d |
| ATRA + GO (Useful, if ATO unavailable/contraindicated) | ATRA 45 mg/m²/d + GO 6 or 9 mg/m² single dose on day 5 | ATRA 45 mg/m²/d wks 1–2, 5–6, 9–10, 13–14, 17–18, 21–22, 25–26 + GO 6 or 9 mg/m² monthly until molecular CR |
📌 Note: ‘Mixing and matching’ induction from one trial with consolidation from another trial is explicitly warned against by NCCN (footnote d, APL-2). Use the complete protocol from one study.
⚠ PHARMACIST ALERT: Cardiac issues + High Risk APL: If low EF or prolonged QTcF at baseline, preferred regimen = ATRA + ATO + GO (single dose 9 or 6 mg/m²) OR ATRA + daunorubicin + cytarabine OR AIDA. Flag this scenario proactively at tumor board.
Drug-Specific Dosing Details
All-Trans Retinoic Acid (ATRA / Tretinoin)
- Standard adult dose: 45 mg/m²/day PO in 2 divided doses (with or after meals, fatty food enhances absorption)
- Pediatric/adolescent dose: 25 mg/m²/day in divided doses (NCCN footnote f, Kutny et al., JCO 2017)
- Available as: 10 mg capsules (Vesanoid)
- Continue until clinical remission criteria met (morphologic CR)
⚠ PHARMACIST ALERT: ATRA is a teratogen (Category X). Mandatory counseling and contraception for ALL women of childbearing potential. Two forms of contraception required. Verify at every encounter.
💎 Clinical Pearl: ATRA capsules can be opened and the contents suspended in oil/peanut butter for patients unable to swallow; this is not FDA-labeled but is done in pediatric practice. Absorption is fat-dependent — take with high-fat meal.
Arsenic Trioxide (ATO / Trisenox)
- Induction dose: 0.15 mg/kg IV daily (daily schedule) OR 0.3 mg/kg days 1–5 wk1, then 0.25 mg/kg 2×/wk wks 2–8 (intermittent schedule)
- Consolidation dose: per protocol (see dosing table above)
- ATO dose cap for obesity: Retrospective data suggest doses >15 mg/day associated with significant AKI (15.8% vs 0%, p=0.001). NCCN v3.2026 acknowledges ‘capped dose of 15 mg may be reasonable for patients with obesity’ — use pharmacist judgment and institutional protocol.
- Infusion: IV over 1–2 hours (can extend to 4 hours if vasomotor reaction); no incompatibilities noted with most standard infusion bags
- Renal adjustment: Not formally specified in labeling; NCCN notes renal monitoring required; data limited for CrCl <30
⚠ PHARMACIST ALERT: ATO dose cap consideration in obesity is a v3.2026 addition. Proactively calculate actual dose — if >15 mg/day, flag for prescriber discussion. Do not assume high body weight warrants proportionally higher dose.
Idarubicin (AIDA-based regimens)
- Induction: 12 mg/m² IV on days 2, 4, 6, 8 (AIDA regimen); age >70y: days 2, 4, 6 only (3 doses)
- Consolidation Cycle 1: 5 mg/m² IV × 4 days
- Consolidation Cycle 3: 12 mg/m² IV × 1 day
- Cumulative anthracycline tracking: Sum all idarubicin (and mitoxantrone) doses across all cycles. NCCN recommends reassessing cardiac function before each anthracycline/mitoxantrone-containing consolidation course when high cumulative doses are used.
- Idarubicin is not renally adjusted per NCCN templates but hepatic dose reduction warranted if LFTs significantly elevated
Mitoxantrone (AIDA consolidation Cycle 2)
- Dose: 10 mg/m²/day IV × 3 days (AIDA Consolidation Cycle 2)
- Cardiac monitoring required; cumulative anthracycline tracking must include mitoxantrone-equivalent conversion (mitoxantrone ×4 = doxorubicin equivalent for rough comparison)
Gemtuzumab Ozogamicin (GO / Mylotarg)
- APL use: Single dose 6 or 9 mg/m² on day 1 (or day 2–5) of induction; additional doses in consolidation until molecular CR
- GO in APL is ‘Useful in Certain Circumstances’ (non-preferred; preferred regimens include ATO-based or ATRA+IDA)
- GO is CD33-targeted: Confirm CD33 expression on flow cytometry before ordering
- Premedicate: diphenhydramine 25–50 mg IV, acetaminophen 650–1000 mg PO, methylprednisolone 1 mg/kg IV (30–60 min before); per institutional protocol
- SOS/VOD risk: monitor LFTs; avoid concomitant hepatotoxins
⚠ PHARMACIST ALERT: GO and leukapheresis: Leukapheresis is CONTRAINDICATED in APL due to risk of coagulopathy exacerbation. If a patient is on GO and leukapheresis is considered (by another team) — intervene.
Dose Modification Framework
ATO Dose Modifications
- QTcF >500 msec: Interrupt ATO; aggressively correct K⁺ and Mg²⁺; obtain cardiology consult; resume when QTcF <460 msec with caution
- Hepatotoxicity (Grade 3–4): Hold ATO; rechallenge at reduced dose per clinical judgment
- Renal toxicity / AKI: Monitor closely; dose cap at 15 mg if obese (see above)
ATRA Dose Modifications
- Differentiation syndrome (severe): Interrupt ATRA until hypoxia resolves; may restart at same dose
- Pseudotumor cerebri (headache, papilledema, vision changes): Reduce ATRA dose or hold; acetazolamide for management
- Hepatotoxicity (Grade 3–4): Hold ATRA; rechallenge when enzymes recover
SUPPORTIVE CARE FOR APL
Coagulopathy Management (CRITICAL)
| Parameter | Target/Threshold | Action |
|---|---|---|
| Platelets | Maintain ≥50 ×10⁹/L | Transfuse |
| Fibrinogen | Maintain >150 mg/dL | Cryoprecipitate ± FFP |
| PT/PTT | Close to normal | FFP |
| QTcF (on ATO) | <500 msec | Hold ATO; correct K/Mg; cardiology consult if unable to calculate QTcF |
| K⁺ / Mg²⁺ (on ATO) | Middle-upper normal range | Supplement aggressively |
| WBC (differentiation syndrome risk) | >10 ×10⁹/L = HIGH RISK | Start steroid prophylaxis |
- Monitor coagulation panel DAILY until coagulopathy resolves
- AVOID tunneled catheters / port placement in early induction (coagulopathy risk)
- If IV access needed: use peripheral IV; if PICC necessary, defer to after coagulopathy controlled; avoid arterial lines if possible
- ATRA itself can reverse coagulopathy by inducing differentiation — starting ATRA is an active coagulopathy treatment
💎 Clinical Pearl: One of the most important pharmacist roles in APL: ensure ATRA is initiated as soon as APL is suspected. A delay of even 24–48 hours can lead to fatal intracranial hemorrhage. This is a true oncologic emergency.
Differentiation Syndrome (DS) Management
Incidence: ~15–25% of patients on ATRA-containing regimens. DS occurs with ATRA, ATO, or both.
| Prophylaxis | Treatment (active DS) | |
|---|---|---|
| Indication | WBC >10 ×10⁹/L at presentation OR any patient receiving ATRA+ATO regimen | Fever + rising WBC + respiratory compromise (hypoxia, pulmonary infiltrates, effusions) |
| Steroid Regimen | Prednisone 0.5 mg/kg/day from day 1 (APL0406 protocol) OR Dexamethasone 10 mg q12h from day 1 (APL 2000 protocol) | Dexamethasone 10 mg IV/PO q12h × 3–5 days, then taper over 2 weeks Switch from prednisone prophylaxis → dexamethasone at first signs |
| ATRA/ATO Management | Continue ATRA and ATO during prophylaxis (do not hold for prophylaxis alone) | Consider HOLDING ATRA (not ATO) if severe hypoxia; resume when symptoms resolve |
| Adjunct | Hydroxyurea for leukocytosis rising during ATRA/ATO therapy | Hydroxyurea for leukocytosis; diuresis for fluid overload Do NOT perform leukapheresis (increases mortality risk in APL) |
📌 Note: The optimal duration of steroid PROPHYLAXIS is unknown per NCCN v3.2026. Follow the protocol-specific recommendation (e.g., APL0406 used prednisone 0.5 mg/kg from day 1 until end of induction). Do not extrapolate from one protocol to another.
⚠ PHARMACIST ALERT: Do NOT perform leukapheresis in APL for high WBC. Unlike other AML, leukapheresis does not improve outcomes and increases coagulopathy risk. Hydroxyurea is the preferred cytoreduction strategy for rising WBC during ATRA/ATO-based therapy.
ATO Cardiac Monitoring Protocol
| Timepoint | Test | Goal/Action |
|---|---|---|
| Baseline (before ATO) | ECG (QTcF), BMP (Na, K, Mg, Ca, Phos, Cr) | Establish baseline QTc; correct electrolytes BEFORE starting |
| Weekly during induction | ECG, BMP | QTcF <500 msec; K & Mg in upper-normal range |
| Before each consolidation cycle | ECG, BMP | Proceed only if QTcF <500 msec |
- QTcF is the PREFERRED correction formula for QT assessment on ATO
- If QTcF cannot be calculated (e.g., bundle branch block, pacing), obtain cardiology consult before proceeding
- Target K⁺ and Mg²⁺: MIDDLE to UPPER range of normal (not just within normal — higher end preferred)
- Avoid all concurrent QT-prolonging agents (see DDI table below)
- Palonosetron or granisetron preferred over ondansetron for antiemesis during ATO therapy
Growth Factor (G-CSF) Restrictions
- G-CSF is CONTRAINDICATED during APL induction — may exacerbate differentiation syndrome and confound blast assessment
- G-CSF may be CONSIDERED during consolidation ONLY for life-threatening infections or sepsis (no prophylactic data to support routine use)
⚠ PHARMACIST ALERT: If another team orders G-CSF during APL induction: FLAG IMMEDIATELY. This is one of the most common prescribing errors in APL management.
Infection Prophylaxis
- Antimicrobial prophylaxis: per institutional protocol and NCCN infection guidelines; standard neutropenia precautions apply
- Antifungal prophylaxis: during neutropenic phases — azole prophylaxis (e.g., posaconazole, fluconazole per institution) BUT be aware of DDI with ATRA (azoles inhibit CYP26A1, potentially ↑ ATRA levels)
- PJP prophylaxis: consider TMP-SMX or alternatives during consolidation with prolonged immunosuppression
- Avoid live vaccines during therapy
KEY DRUG INTERACTIONS (Pharmacist Watchout)
| Drug | Interacting Agent | Mechanism/Risk | Management |
|---|---|---|---|
| ATO | Fluoroquinolones, azoles, antipsychotics, ondansetron | Additive QTc prolongation → TdP risk | Avoid QT-prolonging agents; use ECG before each drug; use granisetron or palonosetron instead of ondansetron |
| ATRA | Azole antifungals (strong CYP inhibitors) | ↑ ATRA plasma levels; may worsen differentiation syndrome | Monitor for differentiation syndrome; adjust prophylactic steroids accordingly |
| ATRA | Vitamin A supplements | Additive hypervitaminosis A toxicity (pseudotumor cerebri, hepatotoxicity) | Counsel patient to STOP vitamin A / multivitamins with vitamin A during ATRA therapy |
| GO (gemtuzumab) | Hepatotoxic drugs, prior liver disease | Risk of SOS/VOD; additive hepatotoxicity | Monitor LFTs; avoid concomitant hepatotoxins; ursodiol is institutional practice (not NCCN-specified) |
💎 Clinical Pearl: During tumor board or chemo review: always scan the medication list for QT-prolonging agents before approving ATO orders. The most commonly missed culprits are fluoroquinolones (especially ciprofloxacin, levofloxacin), azole antifungals, haloperidol, and methadone.
POST-CONSOLIDATION THERAPY & MRD MONITORING
PCR Monitoring Schedule (NCCN v3.2026)
| Timepoint | Sample | Action if Positive |
|---|---|---|
| End of induction (d28–35) | BM aspirate (morphologic assessment; PCR not required for decision) | <5% blasts, no abnormal promyelocytes → proceed to consolidation |
| After consolidation cycle 1 (ATRA+ATO regimen: check at 3–4 mo) | Blood (RT-PCR for PML::RARα) | Repeat BM if blood PCR positive; consider HCT or clinical trial |
| End of ALL consolidation | Blood RT-PCR (mandatory; BM if equivocal) | PCR positive → confirm in 2–4 wks → if confirmed, treat as relapse |
| Post-consolidation surveillance (high-risk / age >60 / long interruptions) | Blood RT-PCR every 3 months × 2 years (low-risk in molecular remission: may individualize per NCCN v3.2026) | Confirm positivity in same lab × 1 within 2–4 wks; treat if confirmed |
- Low-risk patients in molecular remission after consolidation: individualized monitoring; NCCN v3.2026 states ‘monitoring may not be necessary outside clinical trial’ — clinical experience-based decision
- PCR laboratory sensitivity must be stated in the report: most clinical labs at 10⁻⁴. If result is equivocal, consult molecular diagnostics expert
- Wait 2–3 weeks after last ATO dose before PCR to avoid false positives (ATO-induced differentiation can yield positive PCR temporarily)
📌 Note: NCCN v3.2026 update: For ATRA+ATO regimen, consider earlier PCR sampling at 3–4 months DURING consolidation (not just at end).
Maintenance Therapy
- Maintenance is included in some protocols (e.g., ATRA ± oral 6-mercaptopurine/methotrexate in older AIDA-based approaches)
- With ATRA+ATO regimens: maintenance is generally NOT required based on APL0406 and AML17 data
- The benefit of maintenance depends on what induction/consolidation was used — do not extrapolate across protocols
- Oral azacitidine-based maintenance is NOT indicated in APL (this is an AML/MDS tool)
MANAGEMENT OF RELAPSED APL
| Scenario | Treatment | Post-Remission |
|---|---|---|
| 1st relapse (prior ATRA + chemo) | ATO-based regimen (preferred) (ATO ± ATRA ± GO) | If mol CR → auto-HCT (preferred) If no CR → allo-HCT or clinical trial |
| No mol remission after consolidation cycle 1 | Treat as relapse → ATO-based salvage | Consider matched sibling or alternative donor HCT |
| 2nd relapse or post-ATO induction failure | GO monotherapy, or clinical trial | Allo-HCT; if 2nd CR + HCT contraindicated → ATO 6 cycles |
- ATO as single agent in relapse: CR rate 80–90%; molecular remission rate 70–80%
- For patients in 2nd molecular CR post-relapse: auto-HCT preferred over allo-HCT (excellent outcomes if PCR-negative before HCT)
- CNS involvement at relapse: IT chemotherapy for CNS prophylaxis before consolidation for patients in 2nd morphologic remission
- GO as single agent (Cimino regimen): useful for molecularly relapsed APL (PCR+ only)
- Outcomes are uncertain when re-treating with ATO-based regimens if patient received ATO in initial induction/consolidation (footnote k, NCCN)
💎 Clinical Pearl: Key tumor board point: Before labeling relapse as ‘ATO-refractory,’ confirm the PCR was not drawn <3 weeks after last ATO dose (risk of false-positive from differentiation). Repeat in same lab, same assay.
KEY CLINICAL TRIALS (PICO Summary)
| Trial | Population | Intervention | Comparator | Key Results |
|---|---|---|---|---|
| APL0406 (Lo-Coco, NEJM 2013) | Newly diag. low/int-risk APL, age 18–71 | ATRA + ATO (daily) | AIDA (ATRA + Idarubicin) | EFS 97% vs 86% (p=0.02); non-inferior OS; no chemo required for non-high-risk APL |
| AML17 (Burnett, Lancet Oncol 2015) | All-risk newly diagnosed APL | ATRA + ATO (intermittent) | ATRA + chemotherapy (AIDA-like) | OS superior in ATRA+ATO arm (p=0.009); benefit extended to high-risk group |
| APML4 (Iland, Blood 2012) | Newly diag. APL (all risk) | ATRA + Idarubicin + ATO (IV) induction | Historical AIDA control | CRR 95%; 2-yr EFS 88%; fewer relapses vs historical; prednisone prophylaxis used universally |
| GIMEMA-SAL-AMLSG (Lo-Coco, NEJM 2013 – same APL0406) | Low/intermediate-risk APL | ATRA + ATO | AIDA | ATRA+ATO arm: 2-yr EFS 97% vs 86%; confirms chemotherapy-free regimen feasibility |
Additional landmark trials
- C9710 (Powell, Blood 2010): Addition of ATO to ATRA+anthracycline in North American INT study → improved EFS and OS, establishing ATO role in all risk groups
- APML3 (Iland, Haematologica 2012): ATRA + idarubicin ± ATO; established combined induction utility
- QUAZAR APL-001 equivalent: APL maintenance trials — benefit of maintenance depends on induction used; not universally recommended in the ATO era
SPECIAL SITUATIONS & CLINICAL NUANCES
High-Risk APL with Cardiac Contraindications (Low EF / Prolonged QTcF)
- Avoid standard anthracycline-based regimens if EF significantly reduced
- Preferred: ATRA + ATO (daily or intermittent) + GO (single dose 6 or 9 mg/m²) OR ATRA + daunorubicin + cytarabine OR AIDA alone (footnote, APL-4 algorithm)
- If prolonged QTcF at baseline: first-line preferred = ATRA + GO 9 mg/m²; or ATRA + daunorubicin + Ara-C
Pregnancy
- ATRA: Category D — avoid in first trimester; may use after first trimester if life-threatening
- ATO: Category D — avoid in pregnancy; arsenic crosses the placenta
- If diagnosis occurs in pregnancy: multidisciplinary decision; ATRA alone used in 2nd/3rd trimester as bridge; delivery before full treatment when feasible
Elderly / Reduced Performance Status
- Age >70: Idarubicin dose reduction (days 2, 4, 6 only vs standard 4 doses in AIDA)
- ATO-based (ATRA+ATO): preferred in elderly — avoids anthracycline toxicity; excellent outcomes reported
- Cytarabine dose reduction warranted if CrCl <50 or age >60 in cytarabine-containing regimens
Community Center vs. Academic Center
- NCCN v3.2026 cites JAMA Oncol 2025 (Jillella et al.) recommending collaboration with APL-expert center for community hospital cases — 24/7 support model reduces induction mortality
PHARMACIST CLINICAL CHECKLIST
At Diagnosis / Induction Start
- ATRA initiated as soon as APL suspected (do not wait for molecular confirmation)
- Baseline ECG obtained before ATO start; QTcF calculated
- Electrolytes (K, Mg, Ca, Phos) corrected before ATO start; target upper-normal range
- Coagulopathy management ordered: platelet goal ≥50, fibrinogen >150, FFP for PT/PTT
- No central line placed in active coagulopathy
- G-CSF NOT ordered during induction
- Leukapheresis NOT ordered (contraindicated in APL)
- Steroid prophylaxis ordered if WBC >10 ×10⁹/L or patient on ATRA+ATO regimen
- Antiemetic choice: NOT ondansetron (use palonosetron or granisetron with ATO)
- Vitamin A/multivitamin with vitamin A discontinued
- Contraceptive counseling documented (ATRA teratogenicity)
During Treatment
- Weekly ECG + BMP during induction ATO; before each consolidation cycle
- Daily coagulation panel until DIC resolved
- Cumulative anthracycline tracking (idarubicin + mitoxantrone all cycles)
- Cardiac reassessment before each anthracycline/mitoxantrone consolidation cycle
- Medication list scanned for QT-prolonging agents (fluoroquinolones, azoles, antipsychotics)
- PPI/azole interaction: PPIs reduce posaconazole suspension absorption; ensure patient is NOT on PPI with posaconazole suspension (if used for antifungal prophylaxis)
- Differentiation syndrome monitoring: fever, WBC rise, dyspnea, weight gain
Post-Consolidation / Surveillance
- Blood PCR (RQ-PCR for PML::RARA) obtained at end of consolidation to confirm molecular remission
- PCR done ≥2–3 weeks after last ATO dose (avoid false positive)
- Surveillance PCR every 3 months × 2 years for high-risk patients; individualized for low-risk
- Same laboratory used for serial PCR testing
- Positive PCR confirmed by second test in same lab within 2–4 weeks before treatment change
- If cytopenias + PCR negative → BM aspirate to rule out secondary MDS/AML (treatment-related)
CLINICAL PEARLS TAKEAWAYS
💎 Clinical Pearl: APL is the ONLY AML subtype treated emergently before histologic confirmation. Clinical diagnosis (morphology + coagulopathy) mandates ATRA initiation NOW.
💎 Clinical Pearl: Sanz score (WBC/platelet at diagnosis) = only risk stratifier in APL. No ELN score, no TP53, no complex karyotype — just WBC >10 triggers high-risk management.
💎 Clinical Pearl: ATRA+ATO is chemotherapy-free for low/intermediate risk APL (APL0406 data). If a patient with low-risk APL is receiving cytarabine — question why.
💎 Clinical Pearl: Never give leukapheresis in APL. Unlike CML or hyperleukocytic AML, leukapheresis does not help and increases bleeding risk.
💎 Clinical Pearl: The QTcF correction formula is preferred for ATO monitoring. If the physician is using uncorrected QT or QTcB, intervene and request QTcF — this changes management.
💎 Clinical Pearl: Ondansetron + ATO = avoidable QT risk. Suggest granisetron (weak QT effect) or palonosetron instead. Flag this during chemo review.
💎 Clinical Pearl: Vitamin A supplements are absolutely contraindicated with ATRA — hypervitaminosis A (pseudotumor cerebri) can occur. Screen OTC medications at every counseling visit.
💎 Clinical Pearl: PCR timing matters: draw blood sample ≥2–3 weeks after last ATO dose; arsenic-induced differentiation can produce a false-positive PML::RARA signal.
💎 Clinical Pearl: ‘Mixing induction from one APL trial with consolidation from another’ is explicitly warned against by NCCN. At chemo review, verify the consolidation protocol matches the induction trial used.
💎 Clinical Pearl: Secondary MDS/AML can occur after APL therapy. If a patient develops cytopenias in follow-up with a negative PCR — do not assume it is benign. Order BM aspirate with cytogenetics/NGS.
Reference: NCCN Guidelines v3.2026, AML/APL sections. ELN 2022. Key trials: APL0406 (Lo-Coco NEJM 2013), AML17 (Burnett Lancet Oncol 2015), APML4 (Iland Blood 2012), C9710 (Powell Blood 2010).