NCCN 2024-2025
Clinical Pearls
- Aggressive but with features of both indolent and aggressive NHL; incurable with conventional chemotherapy. Often diagnosed in late stages, and majority are elderly (ineligible for high intensity therapy). Goal of therapy is palliative.
- Evaluation: PE, ECOG, B symptoms, CBC, CMP, LDH, PET/CT, HBV/HCV screen, ECHO/MUGA (if anthracycline), pregnancy (if chemo/RT), endo/colonoscopy (SI-II), BM biopsy±aspirate, uric acid (TLS), β2 microglobulin, LP (blastic variant or CNS)
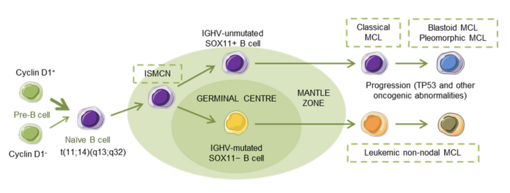
- Genomics: t(11;14)(q13;q32) (CCND1-IGH translocation) causing cyclin D1 overexpression (>95% MCL), CCND1- (<5% MCL); CD5+, CD20+, CD43+, CD23±, CD10±, LEF1- (CLL is +ve), TP53 mutation (poor response to chemoimmuno, HDT/ASCT), SOX11-
- Prognosis: MIPI (age, LDH, WBC, ECOG). Low (<5.7, 5y survival 60%), intermediate (5.7-<6.2, OS 51mo), high (≥6.2, OS 30mo)
- Other factors: POD24, blastoid/pleomorphic features (aggressive, CNS involvement), SOX-11–, Ki-67 (>20-40%), complex karyotype, high β2 microglobulin, and CNS involvement. Ki-67 (predictive biomarker): low (<10%, indolent), intermediate (10-29%), high (≥30%, aggressive). TP53 mutations (10-25%): aggressive, short survival, poor prognosis, BTKi resistance. SOX-11– (IGHV mutation) most common in indolent: leukemic non-nodal CLL-like with splenomegaly, low tumor burden, Ki-67 <10%.
| Variant | Features |
| Classic MCL | Most common, typical immunophenotype. |
| Indolent MCL | SOX11−, low Ki-67, often non-nodal, may be observed initially. |
| In situ MCL | Incidental, cyclin D1+ cells in mantle zones, often low-risk. |
| Leukemic non-nodal MCL | Blood/marrow involvement, SOX11−, less aggressive. |
| Blastoid/Pleomorphic | Aggressive, high Ki-67, TP53+, requires aggressive Rx. |
- Indolent MCL (asymptomatic, non-bulky lymphadenopathy, lack of cytopenia): observation (in few pts), treatment (symptomatic).
- No standard of care therapy (poor response with doxorubicin-based regimens), use chemoimmunotherapy ± ASCT
- TP53 mutation: clinical trials, BOVen, TRIANGLE (alter. RCHOP+ibrutinib/RDHAP if aggressive eligible), less aggressive induction
- Kumar et al (BOVen): ORR 96%, CR 88%, PFS 72%, DSS 91%, OS 76%. ADE diarrhea, neutropenia, infusion-reaction
- Localized Disease (very rare)
- Stage I-II, non-bulky, contiguous: ISRT alone, less aggressive induction ± ISRT
- MCL is the most radiosensitive of all NHLs with meaningful response rates (symptom relief >90%, CR upto 70%)
- Stage II, non-bulky, non-contiguous: less aggressive induction, active surveillance (in selected patients)
- Stage I-II, non-bulky, contiguous: ISRT alone, less aggressive induction ± ISRT
- Advanced Disease (Stage II bulky noncontiguous, Stage III-IV); young, fit, good ECOG PS (ASCT eligible if CR): clinical trial
- Aggressive induction (LyMA, NORDIC, TRIANGLE, BR f/b R+HiDAC, HyperCVAD, R-BAC500)
- LyMA (RDHAP): higher PFS and OS with oxaliplatin (vs cis/carboplatin in ITT; similar in PP). For eligible young patients
- NORDIC (R-maxi-CHOP alternating with R-HiDAC): ORR 96%, CR 54%, OS 70%, EFS 56%, PFS 66%,
- TRIANGLE (3 arms): arm B was superior to arm A (higher 3y FFS, heme-toxicity); Acala/Zanubrutinib wasn’t evaluated.
- Pre-chemo induction (R-Ibrutinib) before HyperCVAD to limit cycles # of R-HyperCVAD in newly diagnosed MCL ≤65y.
- Maintenance therapy (if CR/PR postHDT/ASCT, aggressive induction): Rituximab q8wk x3y (LyMA [categ 1] postHDT/ASCT) and/or Ibrutinib x2yrs (TRIANGLE [category 2A]; acalabrutinib and Zanubrutinib [category 2B])
- LyMa (Rituximab vs observation; <66yo, after ASCT): prolonged EFS, PFS, OS
- LYSA/LYMA (Rituximab): higher EFS, PFS, OS; median PFS and OS was not reached (full population).
- TRIANGLE (Ritux, Ibrutinib, or R-Ibrutinib): comparable outcomes (improved PFS), slightly higher toxicity in R-Ibrutinib
- Historically, standard of care for MCL patients included high-dose chemotherapy followed by ASCT for eligible patients, followed by three years of maintenance rituximab. However, in 2024, an interim analysis of the phase 3
- EA4151 (2024interim analysis; consolidation ASCT+R v R): no survival difference in uMRD status with induction.
- Aggressive induction (LyMA, NORDIC, TRIANGLE, BR f/b R+HiDAC, HyperCVAD, R-BAC500)
- Advanced Disease (Stage II bulky noncontiguous, Stage III-IV); old, frail, poor ECOG PS (ASCT ineligible): clinical trial
- Less aggressive induction (BR, BR-Acalabrutinib, VR-CAP, R-CHOP, R2, R-Acalabrutinib [chemo-free])
- StiL NHL1 (BR vs R-CHOP): longer PFS, TTNT; better tolerated (lower alopecia, heme, infection, PN, stomatitis), higher erythematous skin reaction
- BRIGHT (BR vs R-CHOP or R-CVP): longer PFS and DOR (not OS).
- SHINE (BR-Ibrutinib f/b Ibrutinib vs BR-placebo): higher PFS, ADE; lower OS (nonlymphoma death)
- ECHO (BR-Acalabrutinib vs BR-placebo): higher PFS, ORR, CR; similar OS; slightly higher G3+ ADE
- Acala 100 mg BID indefinitely; Benda 90mg/m2 D1-2, Ritux 375 mg/m2 D1 x6 cycles; f/b Ritux maintenance x2y
- LYM-3002 (VR-CAP vs R-CHOP): longer OS, PFS, CR, TTP; higher G3+ thrombocytopenia, neutropenia, infections (manageable); lower death due disease progression
- Jain 2023 (R-Acala): ORR 94%, CR 90%; PFS and OS NR (2y 92%, 96%); ADE fatigue, myalgia, HA, bruising, AF (2%)
- Maintenance therapy (if CR/very good PR): Rituximab q8wk x2-3y (RCHOP [cat1], BR [cat2A], untested VR-CAP, RBAC500), Acalabrutinib (post BR-Acalabrutinib or R-Acalabrutinib), Lenalidomide (post R2)
- Less aggressive induction (BR, BR-Acalabrutinib, VR-CAP, R-CHOP, R2, R-Acalabrutinib [chemo-free])
- Relapsed MCL
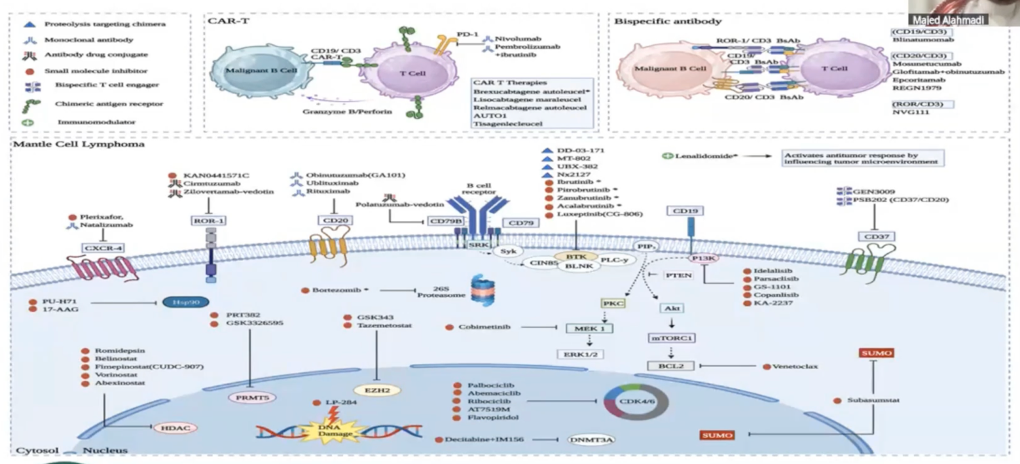
- 2L and subsequent: cBTKi (Acalabrutinib, Zanubrutinib), R-Ibrutinib, Lenalidomide±Rituximab (if BTKi is CI), BR, R-BAC500, Bortezomib±Rituximab, R-DHAP, R-GemOx, Ibrutinib+Venetoclax, Venetoclax±Rituximab, ISRT
- ACE-LY-004 (Acalabrutinib): ORR 81%, CR 43%, DOR (26mo), PFS 20mo, OS NR. Patients with low/intermediate MIPI, classical MCL, Ki-67 <50% had longer DOR, PFS, and higher 24-month OS rates.
- Song 2020 (Zanubrutinib 160mg BID): ORR 84%, CR 68.6%, DOR 19.5mo, PFS 22.1mo; neutropenia, pneumonia
- RAY (R-Ibrutinib vs temsirolimus): ↑ OS, ORR (2x CR if 1L prior), DOR (3x CR if 1L prior); diarrhea, fatigue, cough, AF
- PINNACLE (Bortezomib±Rituximab; synergistic apoptosis): TTP 6.7mo, TTNT 7.4mo, OS 23.5mo
- Obrador-Hevia 2016 (GemOx): ORR 83%. Oxaliplatin has profound effect on cell viability (preferred platinum)
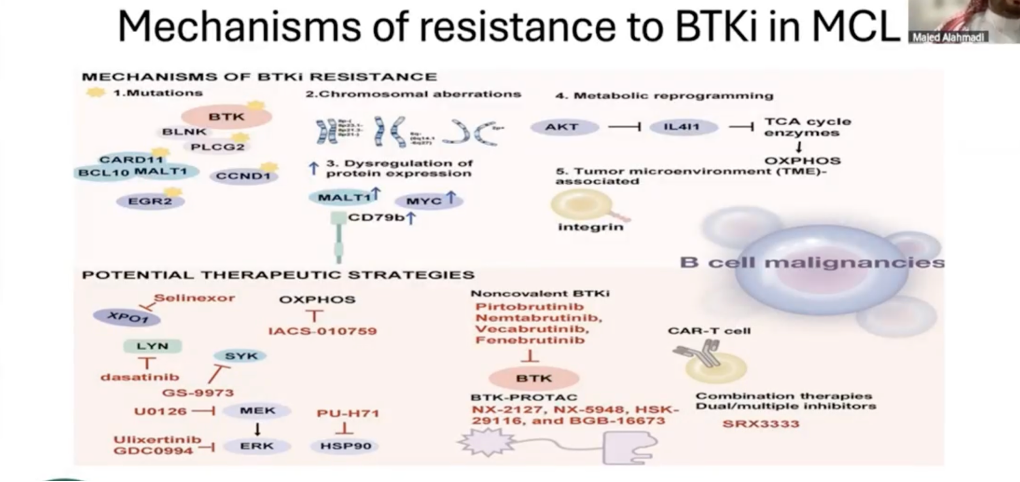
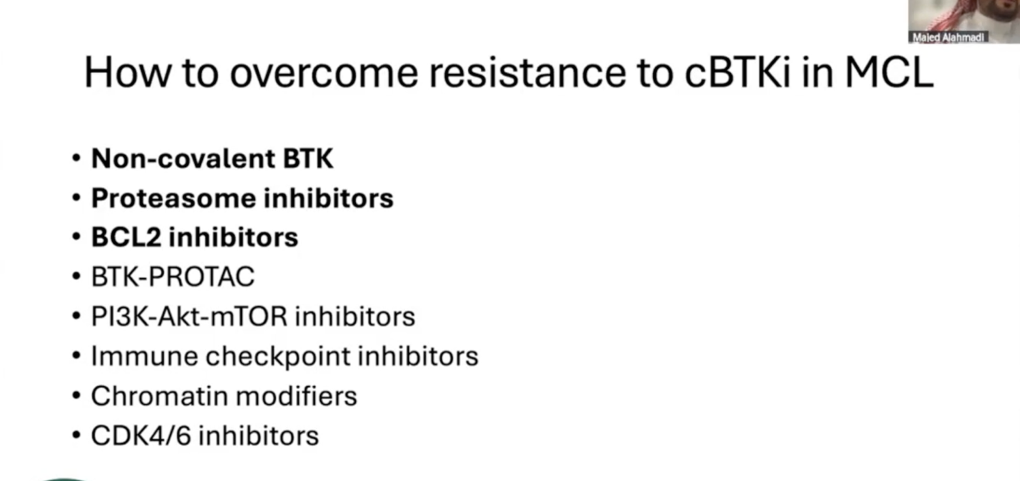
- 3L (after covalent BTKi): Pirtobrutinib (in C481S mutation, covalent BTKi resistance), CAR-T cell (Tecartus, Breyanzi, post chemoimmunotherapy, BTKi), clinical trial, 2L f/b alloSCT (if SC mobilization failure or persistent BM involvement) ±ISRT
- ZUMA-2 (Tecartus): ORR 91%, CR 73%, DOR 28.2mo, PFS 25.8mo, OS 46.6mo
- TRANSCEND NHL 001 (Breyanzi): ORR 83.1%, CR 72.3%, DOR 15.7mo, PFS 15.3mo; ADE heme, CRS 61%, NE 31%
- BRUIN (Pirto, previous cBTKi): ORR 57.8%, CR 20%, DOR 21.6mo; ADE (fatigue, diarrhea, dyspnea; less bleed, AF)
- 4L (after CAR-T, Pirtobrutinib; CAR-T ineligible): Glofitamab-gxbm (if CD20+, category 2B), CAR T, Pirtobrutinib, clinical trial, palliative ISRT, best supportive care
- Phillips 2024: (Glofitamab): overall (ORR 85%, CR 78.3%, DoCR 15.4mo, PFS 16.8mo), postBTKi (ORR 74.2%, CR 71%, DoCR 12.6mo, PFS 8.6mo); CRS 70% (less with 2g Obinu vs 1g Obinu)
- 2L and subsequent: cBTKi (Acalabrutinib, Zanubrutinib), R-Ibrutinib, Lenalidomide±Rituximab (if BTKi is CI), BR, R-BAC500, Bortezomib±Rituximab, R-DHAP, R-GemOx, Ibrutinib+Venetoclax, Venetoclax±Rituximab, ISRT
- Fertility preservation: sperm banking, semen cryopreservation, IVF, ovarian tissue or oocyte cryopreservation
- Follow-up: H&P/labs q3-6mo x5y then annually/PRN. Imaging (C/A/P CT contrast) q6mo x2y then annually
- Supportive Care Considerations for Oncology Pharmacists
- Infusion-reaction (Rituximab, Obinutuzumab): APAP, dexamethasone, diphenhydramine
- Febrile Neutropenia ppx (age≥65): G-CSF (filgrastim 5mcg/kg SC daily D6+ until ANC >0.5 x109/L of nadir). Use broad-spectrum antibiotics if febrile.
- TLS Prophylaxis (high risk due to rapid cell turnover, bulky, Venetoclax, Obinutuzumab, Bortezomib): Allopurinol 100 mg/m2/dose q8h upto 300-800mg/day (intermediate risk) or Rasburicase 0.2mg/kg/day (or flat dose 3-7.5 mg – 6mg) upto 5 days (high risk).
- Cardiotoxicity (Doxorubicin): monitor LVEF by ECHO/MUGA at baseline, then when needed.
- Neuropathy (Vincristine, Cisplatin, Oxaliplatin, Bortezomib [IV>SC]): dose reduction/interruption if severe. Gabapentin 300mg/day (adjust dose per response)
- Cold-induced neuropathy (Oxaliplatin): Avoid cold exposure for 7-10d after dose
- Nephrotoxicity/hemorrhagic cystitis (Cyclophosphamide, Cisplatin, MTX): aggressive hydration (1.5-3 mL/kg/h), mesna (Ifosfamide, cyclophos >1200mg/m2)
- Methotrexate toxicity: leucovorin (if MTX >500-1000 mg/m2), Na bicarb IV (to alkalinize urine and excrete MTX; 1.5-2mEq/kg for 15 mins), hydration (≥3 L/day), Glucarpidase ($$$, if 36h MTX >10uM. 50 units/kg IV x1). Monitor MTX levels (if high risk patients, high dose (>12 mg/m2)), renal function (renal dosing), electrolytes.
- Constipation ppx (Vincristine [neurological]): stool softener (docusate 100mg daily or BID) or osmotic laxative (senna 1 tablet at bedtime); lactulose if refractory
- Conjunctivitis ppx (Cytarabine systemic): prednisolone 1% 2 drops to each eye 4 times daily during first day, until 24-72h post-completion.
- CRS (Glofitamab, CAR T): Obinutuzumab 1g IV (7d prior Glofitamab as CRS mitigation); premeds of APAP, diphenhydramine, dexamethasone (Glofitamab, CAR T-cell therapy)
- Anticoagulation prophylaxis (Lenalidomide)
- HBV/HCV reactivation (Rituximab, Obinutuzumab): screen at baseline, treat when needed. Entecavir or Tenofovir ppx if receiving rituximab.
- PJP Prophylaxis (Bendamustine, Glofitamab, prolonged steroids): TMP-SMX or Dapsone.
- HSV ppx (Bendamustine, prolonged steroids, Bortezomib): acyclovir 400mg PO BID; Acyclovir/Valacyclovir in rituximab-regimen.
- VZV/shingles (Glofitamab):
- Magnesium and Potassium wasting (Cisplatin, Carboplatin): Mg/K supplement replenishment.
- Secondary malignancy (Cyclophosphamide, Bendamustine): screen
- REMS: CAR-T (CRS/ICANS), Lenalidomide (fetal-embryonic toxicity)
| Regimens | Medications |
| BOVen | Zanubrutinib (Brukinsa), Obinutuzumab, Venetoclax |
| R-DHAP | Rituximab, Dexamethasone, High-dose Cytarabine (Ara-C), Platinum (carboplatin, cisplatin, oxaliplatin) |
| R-CHOP | Rituximab, Cyclophosphamide, doxorubicin (Hydroxydaunorubicin), vincristine (Oncovin), Prednisone |
| LyMA (Lymphome Mantellique de l’Adulte) | Induction: R-DHAP x4, f/b R-CHOP if CR not achieved Consolidation: ASCT Maintenance: Rituximab q2 months for 3 years |
| NORDIC (Nordic Lymphoma Group) | Dose-intensified induction: R-maxi-CHOP alternating with Rituximab + HD cytarabine Consolidation: ASCT |
| TRIANGLE (3 trial arms) | Alternating below (category 2A for ibrutinib, category 2B for acalabrutinib or zanubrutinib) Arm A (standard): R-CHOP/R-DHAP → ASCT Arm B (ibrutinib-enhanced care): R-CHOP/R-DHAP + ibrutinib → ASCT → ibrutinib Arm C (transplant-free): R-CHOP/R-DHAP + ibrutinib |
| R-HyperCVAD | Rituximab, Hyperfractionated (smaller doses but more frequent), Cyclophosphamide, Vincristine, doxorubicin (Adriamycin), Dexamethasone Alternating with rituximab, high-dose MTX and cytarabine; (pretreatment to reduce R-HyperCVAD/Rituximab maintenance cycles) |
| BR | Bendamustine, Rituximab |
| VR-CAP | Bortezomib (Velcade), Rituximab, Cyclophosphamide, Doxorubicin (Adriamycin), Prednisone |
| R-BAC500 | Rituximab (375mg/m2 IV D1), Bendamustine (70mg/m2 IV D2-3), Ara-C, (500mg/m2 IV D2-4); q4wk x6cy |
| R2 | Lenalidomide (Revlimid), Rituximab |
| R-GemOx | Rituximab, Gemcitabine, Oxaliplatin |