Overview & Classification
Corticosteroids are among the most widely used agents in hematology/oncology — serving as chemotherapeutic backbones, supportive agents, anti-emetics, and immunosuppressants. They exert effects through both genomic (hours) and non-genomic (minutes) pathways.1,2
Relative Potency Comparison3,4
| Agent | Anti-inflammatory potency | Mineralocorticoid potency | Equivalent dose | Plasma half-life | Biologic half-life |
|---|---|---|---|---|---|
| Hydrocortisone | 1 (reference) | 1 | 20 mg | 1.5–2 h | 8–12 h |
| Prednisone | 4 | 0.25 | 5 mg | 3.4–3.8 h | 18–36 h |
| Prednisolone | 4 | 0.25 | 5 mg | 2–3 h | 18–36 h |
| Methylprednisolone | 5 | 0.5 | 4 mg | 1.8–5.2 h | 18–36 h |
| Dexamethasone | 25–30 | 0 (negligible) | 0.75 mg | 1.8–3.5 h | 36–54 h |
💡 Key concept
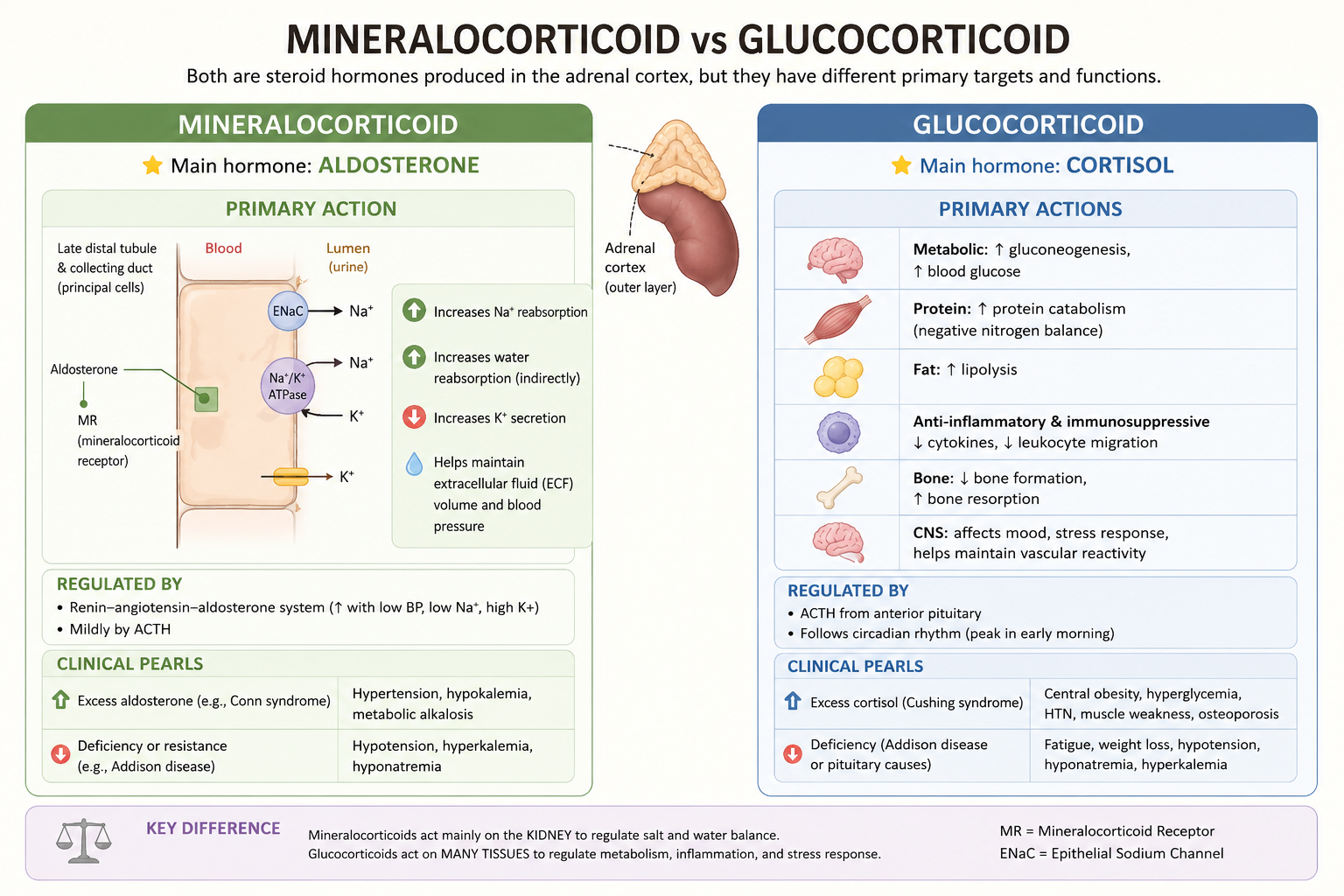
Dexamethasone has ZERO mineralocorticoid activity → less fluid retention than prednisone or hydrocortisone.
This matters in myeloma patients who are often elderly with cardiovascular comorbidities.
Why do steroids work in cancer?
Lymphoid malignancies
(NHL, ALL, CLL, MM)5,6
- Direct lymphocytolytic effect via BIM upregulation → apoptosis
- Inhibit NF-κB → reduce pro-survival signals in lymphoma/myeloma cells
- Suppress IL-6 (critical myeloma growth factor)
- Enhance sensitivity to other chemotherapy agents
Supportive roles7,8
- Anti-emetic: dexamethasone (mechanism not fully elucidated, may involve prostaglandin inhibition)
- Anti-edema: reduce CNS/spinal cord edema (cord compression, brain mets)
- Reduce infusion reactions (premedication for rituximab, paclitaxel)
- Appetite stimulation in cancer cachexia
- Hypercalcemia of malignancy (inhibit calcitriol synthesis)
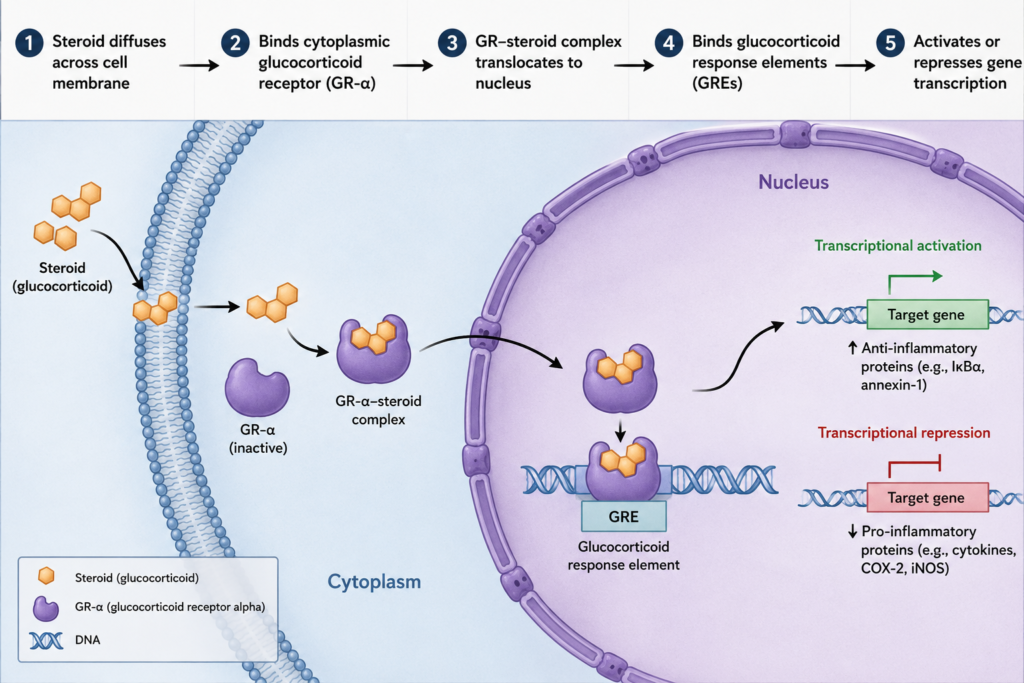
Mechanism of Action
Genomic pathway (primary)1
Key downstream effects in Hem/Onc5,6,9
| Effect | Mechanism | Clinical relevance |
|---|---|---|
| Lymphocyte apoptosis | Upregulates BIM (pro-apoptotic BH3-only protein); suppresses BCL-2 family | Core cytotoxic mechanism in ALL, DLBCL, MM, CLL |
| NF-κB inhibition | GR directly interacts with NF-κB subunits; upregulates IκBα | Anti-inflammatory + anti-tumor in lymphoid neoplasms |
| IL-6 suppression | Transcriptional repression of IL-6 gene | Critical in MM — IL-6 is primary myeloma growth/survival factor |
| VEGF suppression | Reduce VEGF transcription | Anti-angiogenic; reduces tumor vascularity |
| T-cell suppression | Reduce T-cell proliferation; shift Th1→Th2; reduce IL-2 | GVHD treatment; but also explains infectious risk |
| Myelopoiesis stimulation | Demargination of neutrophils; inhibit CXCR4 | Neutrophilia after steroid (can confuse CBC interpretation!) |
⚠️ Steroid resistance10
Emerges via GR mutations (GR-β isoform overexpression), upregulation of anti-apoptotic proteins (BCL-2, BCL-XL, MCL-1), or efflux pumps (MDR1/P-glycoprotein).
Common in relapsed ALL and MM.
Non-genomic pathway (rapid effects, minutes)11
Mediated via membrane-bound GRs and second messenger cascades. Explains rapid anti-emetic effects, rapid anti-inflammatory effects at high doses, and immediate hemodynamic effects in high-dose pulses.
Pharmacokinetics3,4,12
| Parameter | Prednisone | Prednisolone | Methylprednisolone | Dexamethasone |
|---|---|---|---|---|
| Prodrug? | Yes → prednisolone (hepatic 11β-HSD) | No (active) | No | No |
| Bioavailability PO | ~80% | ~80–90% | ~82–90% | ~70–80% |
| Protein binding | 70–90% (albumin, CBG) | 70–90% | ~40–90% | ~68% (albumin) |
| Volume of distribution | 0.4–1.0 L/kg | 0.5 L/kg | 1.2–1.5 L/kg | 0.8–1.0 L/kg |
| Metabolism | Hepatic (CYP3A4) | Hepatic (CYP3A4) | Hepatic (CYP3A4) | Hepatic (CYP3A4) |
| Plasma T½ | 3.4–3.8 h | 2–3 h | 1.8–5.2 h | 1.8–3.5 h |
| Biologic T½ (HPA effect) | 18–36 h | 18–36 h | 18–36 h | 36–54 h |
| CNS penetration | Moderate | Moderate | Good | Excellent (lipophilic) |
| Renal adjustment | Not required | Not required | Not required | Not required |
| Hepatic impairment | Avoid severe — impaired conversion | Use prednisolone (active) | Use with caution | Use with caution |
⚠️ Prednisone in liver failure13
Prednisone requires hepatic conversion to prednisolone
(active form). In severe hepatic impairment (cirrhosis, VOD/SOS post-transplant), use prednisolone directly to ensure adequate drug levels.
Dexamethasone: why it dominates in myeloma and CNS disease3,14
- Longer biologic half-life (36–54 h) → less frequent dosing
- Highest anti-inflammatory potency (25–30× hydrocortisone)
- Zero mineralocorticoid activity → less fluid retention (crucial in elderly MM patients)
- Excellent CNS penetration (lipophilic) → CSF levels ~4× higher than prednisone equivalent dose
- No prodrug conversion needed
Regimens by Disease
R-CHOP-21 (standard frontline): Prednisone 40 mg/m²/day orally, days 1–5 every 21 days × 6–8 cycles (with Rituximab, Cyclophosphamide, Doxorubicin, Vincristine).
GELA trial (n=399) — R-CHOP improved 5-yr OS 58% vs CHOP 45% in elderly DLBCL15
DA-EPOCH-R: Prednisone 60 mg/m²/day, days 1–5 (dose-adjusted etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin + rituximab)16,17
BEACOPP escalated: Prednisone 40 mg/m²/day, days 1–14 per cycle18
Salvage ICE: Dexamethasone 40 mg/day, days 1–4 (Ifosfamide, Carboplatin, Etoposide)19
Salvage DHAP: Dexamethasone 40 mg/day IV/PO, days 1–42
Landmark trial — LD-Dex vs HD-Dex (ECOG E4A03, n=445): Low-dose dexamethasone (40 mg days 1,8,15,22 = weekly) vs High-dose dexamethasone (40 mg days 1-4, 9-12, 17-20 per 28-day cycle). LD-Dex significantly superior 1-yr OS (96% vs 87%, p=0.0002) with less toxicity → LD-Dex is now standard.21
| Regimen22,23,24,25 | Dexamethasone dose | Key trial | Setting |
|---|---|---|---|
| VRd (Bortezomib+Len+Dex)22 | 40 mg days 1,8,15,22 (cycles 1–8); 40 mg weekly thereafter | SWOG S0777 (NEJM 2017) | Frontline transplant/non-transplant eligible |
| Dara-RVd | Same as RVd | PERSEUS (NEJM 2024) | Frontline transplant eligible |
| Rd (Len+Dex) | 40 mg days 1,8,15,22 | FIRST trial (NEJM 2014) | Frontline non-transplant eligible |
| Dara-Rd23 | Same as Rd | MAIA (NEJM 2019) | Frontline non-transplant eligible |
| VMP (Bortezomib+Melphalan+Prednisone) | Prednisone 60 mg/m² days 1–4 | VISTA (NEJM 2008) | Frontline non-transplant eligible (now less common) |
| KRd (Carfilzomib+Len+Dex) | 40 mg weekly | ASPIRE (NEJM 2015) | Relapsed/refractory |
| DVd (Dara+Bortezomib+Dex) | 20 mg pre-Dara days 1,2,8,9 then 40 mg weekly | CASTOR (NEJM 2016) | Relapsed/refractory ≥1 prior line |
| DPd (Dara+Pomalidomide+Dex) | 40 mg weekly | APOLLO (JCO 2021) | Relapsed/refractory ≥2 prior lines |
Age >65 or frail patients: Consider reducing dexamethasone to 20 mg weekly due to increased toxicity (infections, DVT, psychiatric effects). No landmark trial mandates 40 mg in frail elderly.26,27
Dexamethasone vs Prednisone — the key debate
Dexamethasone has better CNS penetration (CSF levels ~4× higher than prednisone), superior lymphocytolytic effect, and is preferred in pediatric ALL and pediatric-inspired adult regimens.28,29
| Regimen30,31 | Steroid | Dose | Reference |
|---|---|---|---|
| CALGB 10403 (ped-inspired) | Dexamethasone | 6 mg/m²/day × 28 days induction; pulses in maintenance | Stock W et al. Blood. 2019 |
| Hyper-CVAD (Part A) | Dexamethasone | 40 mg/day days 1–4, 11–14 | Kantarjian HM et al. JCO 2004 |
| GRAALL-2005 | Prednisone 60 mg/m²/day induction phase | Days 1–7 (steroid prephase), then reinduction | Huguet F et al. JCO 2009 |
| BFM-like (pediatric) | Dexamethasone | 6–10 mg/m²/day × 28 days | Pui CH et al. Lancet. 2008 |
⚠️ Dexamethasone in adults with ALL: Associated with more avascular necrosis and psychiatric toxicity compared to prednisone. Risk-benefit must be considered in adults >40 years.28
CODOX-M/IVAC: Prednisone component within the CODOX-M phase32
HyperCVAD/MA: Dexamethasone 40 mg/day days 1–4 and 11–14 (Part A)33
High-dose methylprednisolone (HDMP) ± Rituximab: Methylprednisolone 1 g/m²/day × 5 days — used in del(17p)/TP53-mutated relapsed/refractory CLL. Not first-line per NCCN (BTK inhibitors preferred).34,35
Acute GVHD — first-line: Methylprednisolone 1–2 mg/kg/day IV (or prednisone 1–2 mg/kg/day PO). Steroids remain standard first-line for grade II–IV acute GVHD despite modest efficacy (~50% CR rate).36,37
Steroid-refractory acute GVHD: Ruxolitinib (JAK1/2 inhibitor) is FDA-approved for steroid-refractory aGVHD based on REACH2 trial (ORR 62% vs 39% BAT, p<0.001).38
Chronic GVHD — first-line: Prednisone 1 mg/kg/day ± cyclosporine, taper over months.39
| Regimen40,41 | Dose | Expected Response | Notes |
|---|---|---|---|
| Prednisone | 1–2 mg/kg/day PO × 2–4 weeks then taper | ~70–80% initial response; ~20–30% durable | Standard first-line (ASH 2019 ITP Guidelines) |
| Dexamethasone pulse | 40 mg/day × 4 days PO (repeat q2–4 weeks × 1–3 cycles) | ~80–90% initial CR; ~50% sustained at 6 months | Higher initial CR, faster response than prednisone |
| Methylprednisolone IV | 1 g/day × 3 days (emergency/hospitalized) | Rapid platelet rise within 24–48 h | For life-threatening bleeding |
Prednisone 1–1.5 mg/kg/day PO × 1–3 weeks, then slow taper over 3–6 months. Target: Hgb ≥10 g/dL or ≥2 g/dL above baseline.42
| Emetogenic risk43,44 | Dexamethasone dose | Combination |
|---|---|---|
| High emetic risk (HEC) | 12 mg IV/PO day 1; then 8 mg days 2–4 | +5HT3 antagonist + NK1 antagonist ± olanzapine |
| Moderate emetic risk (MEC) | 8 mg IV/PO day 1; ± days 2–3 | +5HT3 antagonist ± NK1 antagonist |
| Low emetic risk | 4–8 mg IV/PO day 1 (single dose, optional) | Single agent sufficient |
⚠️ Dexamethasone anti-emetic dose reduction: Consider reducing to 8 mg (HEC) or 4 mg (MEC) if combined with NK1 antagonist (aprepitant/netupitant) due to CYP3A4 inhibition by NK1 antagonists increasing dex exposure by ~2-fold.43
Dexamethasone 10–16 mg IV loading dose, then 4–8 mg IV/PO q6h. Reduces peritumoral edema rapidly. Begin RT/surgical decompression urgently in parallel.45,46
Toxicities
In hematologic malignancies, patients often receive prolonged, high-dose steroids in combination with immunosuppressants — this dramatically amplifies all toxicities below.
Short-term toxicities (days to weeks)
| Toxicity | Incidence | Management | Reference |
|---|---|---|---|
| Hyperglycemia | ~40–50% in non-diabetics; higher in diabetics | FSBS monitoring; insulin correction scales; consider insulin regimen in persistent hyperglycemia. Dexamethasone causes prolonged post-prandial hyperglycemia. | Kwon S & Hermayer KL. Am J Med Sci. 2013;345(4):274–277 |
| Insomnia / neuropsychiatric | Up to 50% (mood changes, anxiety, depression, mania) | Take AM doses (avoid PM); consider low-dose olanzapine or quetiapine; dose reduction if severe. Dexamethasone > prednisone for CNS effects. | Bhatt M et al. Oncology. 2018;32(1) |
| Fluid retention / edema | Common with prednisone (mineralocorticoid effect) | Dietary sodium restriction; loop diuretics PRN. Dexamethasone has minimal effect. | UpToDate 2024 |
| GI distress / ulceration | Increased when combined with NSAIDs (~15-fold risk increase) | PPI (omeprazole 20 mg daily) if concurrently on NSAIDs or anticoagulants. Steroids alone do NOT routinely require PPI. | Piper JM et al. Ann Intern Med. 1991;114(9):735–740 | ACG Guidelines 2022 |
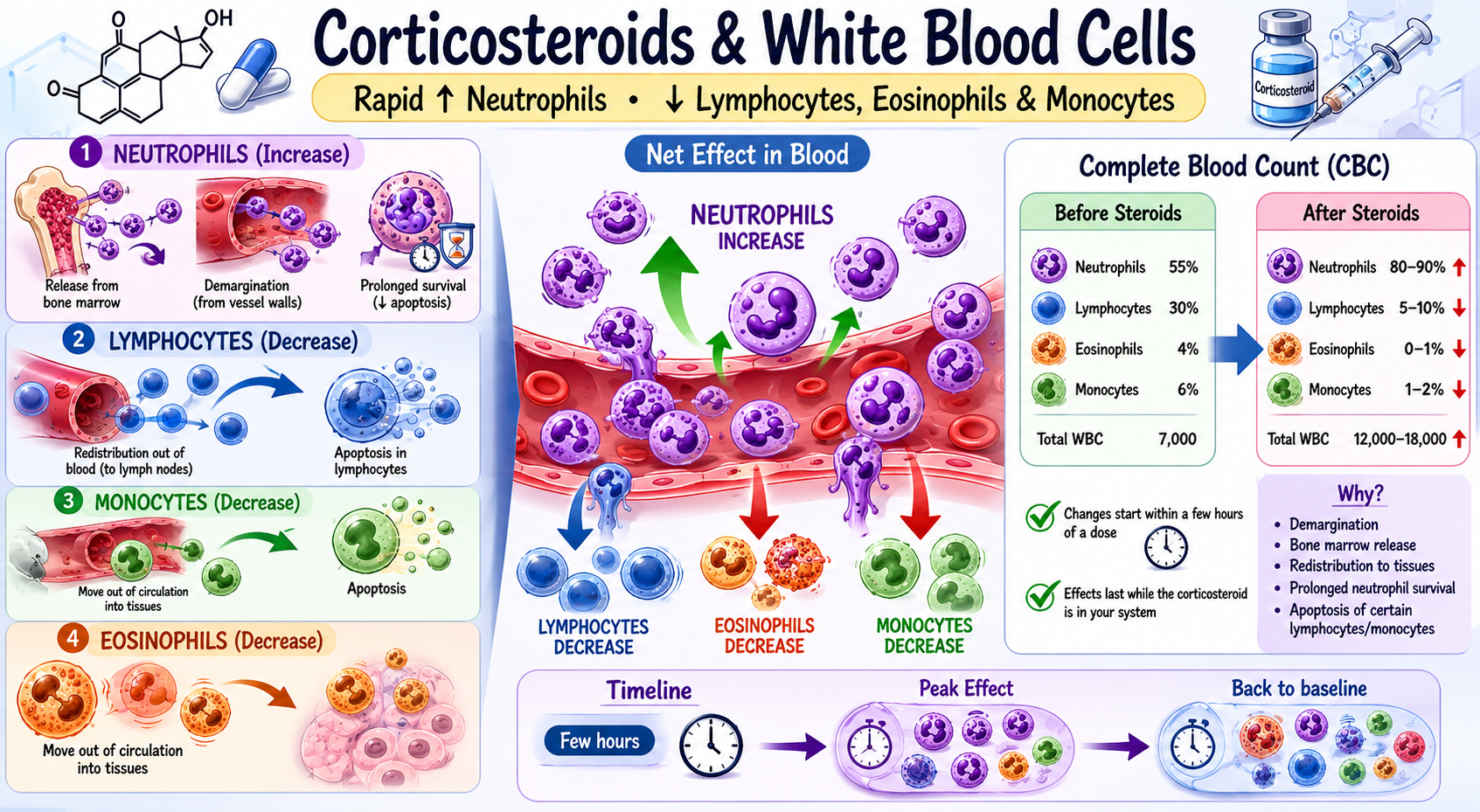
| Leukocytosis (neutrophilia) | WBC may rise 5,000–20,000/μL within 24–48 h | Do NOT interpret as infection if temporally related to steroid initiation. Lymphopenia also common. | Shoenfeld Y et al. JAMA. 1981;245(15):1545–1549 |
| Hypertension | Common; dose-dependent | BP monitoring; antihypertensives as needed | UpToDate 2024 |
| Appetite increase / weight gain | Very common | Dietary counseling | FDA PI |
| Hypokalemia | More with hydrocortisone/prednisone (mineralocorticoid); less with dexamethasone | Electrolyte monitoring; oral KCl supplementation | UpToDate 2024 |
Long-term toxicities (weeks to months)
| Toxicity | Threshold / Risk factors | Management / Prevention | Reference |
|---|---|---|---|
| Osteoporosis / fractures | Any dose >5 mg prednisone equivalent /day >3 months | Calcium 1000–1200 mg/day + Vitamin D 600–800 IU/day + Bisphosphonate (alendronate, zoledronic acid) for moderate/high fracture risk per FRAX. DEXA scan at baseline and every 1–2 years. | ACR Glucocorticoid-Induced Osteoporosis Guidelines 2022 (Buckley L et al.) |
| Avascular necrosis (AVN / osteonecrosis) | Cumulative dose, high single doses; dexamethasone in MM patients >40 y/o | No proven prevention. Early MRI if hip/shoulder/knee pain. Orthopedics consult. Core decompression for early AVN. | Miller KD et al. Ann Intern Med. 1998;128(3):207–213 | Shah M et al. Leukemia. 2004 |
| HPA axis suppression / adrenal insufficiency | ≥20 mg prednisone eq./day for ≥3 weeks | Gradual tapering. Stress dosing during surgery/illness (hydrocortisone 50–100 mg IV q8h). Morning cortisol or ACTH stimulation test if concerned. | Dinsen S et al. Eur J Intern Med. 2013;24(6):499–503 |
| Myopathy (proximal) | Higher risk with fluorinated steroids (dexamethasone, triamcinolone) >weeks | Dose reduction; physical therapy. Distinguishing from disease-related weakness can be challenging. | Pereira RM & Freire de Carvalho J. Autoimmune Rev. 2011;10(9):563–570 |
| Cataracts (posterior subcapsular) | Duration-dependent | Annual ophthalmology evaluation in patients on prolonged steroids | Cumming RG et al. NEJM. 1997;337(1):8–14 |
| Cushing’s syndrome | Prolonged moderate-high dose | Dose minimization; use lowest effective dose | UpToDate 2024 |
| Immunosuppression / infections | Prednisone ≥20 mg/day ≥4 weeks; combined immunosuppression | See Prophylaxis tab | ASCO OI Prevention Guidelines 2018 |
| VTE (with IMiDs) | IMiD + steroid → HIGH VTE risk (up to 25% without prophylaxis) | See Prophylaxis tab | Palumbo A et al. Leukemia. 2008;22(2):414–423 |
AVN in myeloma: High-dose dexamethasone regimens (old HD-Dex) carried ~7–10% cumulative AVN risk. Even with low-dose dex, AVN occurs in ~5–7% of MM patients over their disease course. Educate patients to report new joint pain immediately.47
Prophylaxis with Steroids
When to start: Steroids ≥20 mg prednisone equivalent/day for ≥4 weeks, especially when combined with alkylating agents, fludarabine, anti-CD20 agents, or in GVHD patients on immunosuppression.
| Agent48,49,50 | Dose | Notes |
|---|---|---|
| TMP-SMX DS (preferred) | 1 DS tab PO 3×/week OR 1 SS tab daily | Also provides prophylaxis against Toxoplasma. Check for G6PD, sulfa allergy. |
| Dapsone | 100 mg PO daily | If sulfa allergy. Check G6PD first (risk of hemolytic anemia in G6PD deficiency). |
| Atovaquone | 1500 mg PO daily with food | Best tolerated but most expensive. Good if sulfa allergy + G6PD deficient. |
| Aerosolized pentamidine | 300 mg via Respirgard II inhaler monthly | Least preferred; does not cover extrapulmonary PCP; requires respiratory isolation for administration. |
Indicated in patients on prolonged high-dose steroids, especially in AML induction, HSCT, and severely immunocompromised states.
| Population51,52 | Agent | Notes |
|---|---|---|
| AML induction / high-risk MDS (neutropenia expected) | Posaconazole 300 mg PO daily (preferred) | NCCN recommended. ASPECT trial showed superiority over fluconazole/itraconazole for invasive fungal infections (IFI) and mortality. |
| Prolonged steroids, lower risk | Fluconazole 100–200 mg PO daily | Covers Candida, NOT molds. Cost-effective for low mold-risk patients. |
| HSCT, active GVHD on steroids | Posaconazole or Voriconazole or Micafungin | Per institutional protocol; Aspergillus coverage critical |
Lenalidomide or thalidomide + dexamethasone without prophylaxis: VTE incidence up to 25%. This is one of the most important safety issues in myeloma management.
| Risk stratification53,54,55 | Risk factors | Recommended prophylaxis |
|---|---|---|
| Low risk | IMiD + Dex alone, no additional risk factors | Aspirin 81–325 mg/day PO |
| High risk | ≥1 additional risk factor (prior VTE, immobility, active infection, cardiac disease, DM, obesity, EPO use, high-dose dex, multi-agent chemo) | LMWH (enoxaparin 40 mg SC daily) OR warfarin (INR 2–3) |
Initiate calcium + vitamin D + consider bisphosphonate for any patient on glucocorticoids ≥5 mg prednisone equivalent/day expected to last ≥3 months.
| Agent56,57 | Dose | Indication threshold |
|---|---|---|
| Calcium carbonate | 1000–1200 mg/day elemental Ca (divide doses ≤600 mg) | All patients on chronic steroids |
| Vitamin D | 600–800 IU/day (or higher if deficient) | All patients on chronic steroids |
| Alendronate (preferred oral) | 70 mg PO weekly | Moderate/high fracture risk (FRAX ≥10% major osteoporotic fracture) |
| Zoledronic acid (IV) | 5 mg IV once yearly | Cannot tolerate oral BP or esophageal disease. Also standard in MM. |
| Denosumab | 60 mg SC q6 months (osteoporosis) or 120 mg q4 wk (bone mets) | If renal insufficiency (avoid bisphosphonates if eGFR <30–35) |
Steroids alone do NOT significantly increase GI bleed risk. PPI prophylaxis is recommended ONLY when steroids are combined with NSAIDs or anticoagulants.58,59
Common practice to routinely prescribe PPI with ALL chemotherapy steroid regimens, but evidence supports it specifically when NSAIDs or anticoagulants co-prescribed. Be mindful of PPI-related risks (C. diff, hypomagnesemia, drug interactions).
Steroid Taper / Adrenal Insufficiency Prevention+
If steroids ≥20 mg prednisone equivalent/day for ≥3 weeks: taper gradually rather than abrupt discontinuation to allow HPA axis recovery.60,61
- Reduce by 10 mg/day every 1–2 weeks until reaching 20 mg/day, then reduce by 2.5–5 mg every 2–4 weeks
- Physiologic replacement dose: ~5–7.5 mg prednisone/day (or 10–20 mg hydrocortisone/day)
- Stress dose steroids (surgery/illness): hydrocortisone 50–100 mg IV q8h → taper over 1–3 days
Drug Interactions
Dexamethasone is a moderate CYP3A4 INDUCER. This is highly relevant in myeloma where many novel agents are CYP3A4 substrates.
| Drug / class62,63,64,65,66 | Interaction with steroids | Mechanism | Clinical action |
|---|---|---|---|
| Azole antifungals (posaconazole, voriconazole, itraconazole, fluconazole) | ↑ Steroid levels 2–6× | CYP3A4 inhibition → reduced steroid metabolism | Reduce steroid dose when adding azoles (e.g., dexamethasone anti-emetic dose halved when NK1 used concomitantly). Monitor for Cushingoid features. |
| Ibrutinib (BTK inhibitor) | Dex ↓ ibrutinib levels | Dex induces CYP3A4 → ↑ ibrutinib metabolism | Avoid concomitant use if possible; if necessary, monitor clinical response |
| Venetoclax | Dex ↓ venetoclax levels by ~50% | CYP3A4 induction | Avoid strong CYP3A4 inducers with venetoclax. Use alternative steroid (prednisolone less inducing) or timing separation if unavoidable. |
| Warfarin | Variable; may ↑ or ↓ INR | Multiple mechanisms | Increase INR monitoring frequency when steroids started/stopped |
| NSAIDs | ↑ GI ulceration and bleeding risk (~15×) | Synergistic mucosal injury | Avoid combination; if necessary, add PPI |
| Live vaccines | Risk of disseminated vaccine infection | Immunosuppression | Contraindicated in patients on immunosuppressive steroid doses (>20 mg prednisone/day for >2 weeks) |
| Insulin / antidiabetics | Reduced hypoglycemic effect; ↑ blood glucose | Steroid-induced insulin resistance / gluconeogenesis | Increase insulin doses; monitor glucose. Dexamethasone causes predominantly post-prandial hyperglycemia → NPH insulin or rapid-acting prandial insulin preferred over basal-only adjustment. |
| Fluoroquinolones (ciprofloxacin, levofloxacin) | ↑ tendon rupture risk | Synergistic tendinopathy | Counsel patients; avoid prolonged combination if possible |
| Cyclosporine / tacrolimus | ↑ Immunosuppression; cyclosporine levels variable (CYP3A4 interaction) | CYP3A4 interaction; additive immunosuppression | Monitor calcineurin inhibitor levels; monitor for opportunistic infections |
| Amphotericin B | ↑ Hypokalemia | Additive electrolyte wasting | Frequent electrolyte monitoring; KCl supplementation |
| Diuretics (loop, thiazide) | ↑ Hypokalemia | Additive electrolyte loss | Monitor K+; supplement PRN |
Dexamethasone + posaconazole (commonly co-prescribed in AML or HSCT patients): Posaconazole inhibits CYP3A4 → dexamethasone AUC increases significantly. This combination is frequently used but requires dose reduction of dexamethasone (e.g., for anti-emesis or anti-inflammatory use) and careful monitoring for steroid side effects.67,68
Monitoring Parameters
Inpatient — acute/intensive phase69,70,71
- Blood glucose: Q6–8h (or per sliding scale); daily in stable patients
- Blood pressure: Q shift
- Weight / fluid balance: Daily (fluid retention, especially prednisone)
- Electrolytes (K+, Na+, Mg2+): Daily if receiving amphotericin, loop diuretics, or vomiting
- CBC: Monitor for stress leukocytosis (can mislead) and lymphopenia
- Neuropsychiatric symptoms: Daily assessment; note sleep quality
- Infection signs: Temperature, CRP, signs of fungal/bacterial infection
Outpatient — chronic therapy69,70,71
- HbA1c + fasting glucose: Baseline, then every 3–6 months
- Blood pressure: Every visit
- Weight: Every visit
- DEXA scan: Baseline (if on steroids ≥3 months expected); repeat every 1–2 years
- Ophthalmology: Annual (cataracts, glaucoma)
- Lipid panel: Annually (steroid dyslipidemia)
- Morning cortisol / ACTH stim test: If adrenal insufficiency suspected
- Hip/shoulder/joint pain assessment: Each visit (AVN early detection)
Hyperglycemia management in inpatient setting
Steroid-induced hyperglycemia pattern differs by steroid type. This has major implications for insulin selection.
| Steroid72,73,74 | Hyperglycemia pattern | Preferred insulin approach |
|---|---|---|
| Prednisone (daily AM dose) | Post-lunch and afternoon peak; normal fasting | NPH insulin in AM (peaks 4–6 h, covers PM) OR prandial rapid-acting insulin at lunch/dinner |
| Dexamethasone (long-acting, 36–54 h biologic T½) | Prolonged, all-day elevation; fasting hyperglycemia also common | Basal insulin (glargine/ detemir) + prandial correction; avoid NPH only |
| Methylprednisolone IV (pulse) | Severe acute hyperglycemia, all-day | Insulin drip (ICU) or aggressive subcutaneous correction scale; basal-bolus regimen |
Pharmacist Watchouts
Prednisone requires hepatic activation → use prednisolone in liver failure
Prednisone is a prodrug converted by hepatic 11β-HSD1 to prednisolone. In significant hepatic dysfunction (e.g., SOS/VOD post-HSCT, cirrhosis, severe liver metastases), this conversion is impaired → inadequate active drug. Switch to prednisolone 1:1 (same dose in mg).13
Low-dose dexamethasone is the standard in MM — do NOT use HD-Dex regimens
ECOG E4A03 demonstrated LD-Dex (40 mg weekly) superior OS (1-yr OS 96% vs 88%, p<0.01) and significantly less toxicity vs HD-Dex (40 mg days 1-4, 9-12, 17-20). HD-Dex was associated with higher rates of DVT, serious infections, and early deaths. If you see a HD-Dex order in a newly diagnosed MM patient, question it.21
Dexamethasone + azole antifungals = significantly increased steroid exposure
Posaconazole/voriconazole inhibit CYP3A4 → dexamethasone AUC ↑ 2–6×. This is common in myeloma (dex + len + posaconazole). Patients present with Cushingoid features, worsening hyperglycemia, severe insomnia. Reduce dex dose when adding azoles.68
Dexamethasone reduces venetoclax levels (CYP3A4 induction)
This is critical for venetoclax-based regimens. In AML (Ven-AZA) or CLL (Ven-R), concurrent use of dexamethasone (even for anti-emesis) can reduce venetoclax efficacy. If steroid anti-emesis needed, consider short course or alternative agents.
In patients with relapsed or refractory multiple myeloma, an increase in mortality was noted when venetoclax was added to bortezomib and dexamethasone (in patients without the t(11;14) translocation [Kumar 2020]). Relapsed/refractory t(11;14) multiple myeloma is an off-label use for venetoclax.75,76
VTE prophylaxis in IMiD-based regimens is mandatory — not optional
Lenalidomide/thalidomide + dexamethasone combinations carry up to 25% VTE risk without prophylaxis. Always verify VTE prophylaxis order. Risk-stratify: aspirin 81–325 mg (low risk) vs LMWH/warfarin (high risk: prior VTE, immobility, multi-agent, obesity, EPO, high-dose dex).53,25
PCP prophylaxis thresholds in steroid-containing regimens
Trigger: ≥20 mg/day prednisone equivalent for ≥4 weeks AND + another immunosuppressant (rituximab, alkylator, fludarabine). TMP-SMX DS 3×/week is first-line. Check: sulfa allergy, G6PD status before choosing alternative (dapsone → hemolysis in G6PD deficiency).48,50
Steroid-induced hyperglycemia: type of steroid determines insulin strategy
AM prednisone → afternoon peak → NPH AM preferred. Dexamethasone → all-day effect → basal-bolus preferred. Do NOT assume one sliding scale works for all steroids. Coordinate with endocrinology/diabetes team for patients with known DM or persistent FSBS >180 mg/dL.72
Steroid taper is required if ≥3 weeks at ≥20 mg prednisone — abrupt stop = adrenal crisis risk
Gradual taper schedule required. In emergency (patient unable to take PO, surgery, illness, sepsis): stress-dose hydrocortisone 50–100 mg IV q8h. Always provide a written taper schedule to patients on discharge. Educate: do not stop suddenly.60
Bone protection → initiate at therapy start, not retrospectively
If patient will be on ≥5 mg prednisone equivalent for ≥3 months: start calcium + Vit D + assess FRAX score at initiation. In myeloma: zoledronic acid (or denosumab if eGFR <30) is standard regardless of steroids for bone protection. Do not wait for osteoporosis to be “documented.”56,77
10. Steroid leukocytosis ≠ infection
WBC can rise 5,000–20,000/μL within 24–48 h of steroid initiation due to neutrophil demargination (not shift in production). Concurrent lymphopenia is expected. Alert prescribers who may incorrectly diagnose and treat “infection.” Context is everything.78
Handouts
📖 References
- Coutinho AE & Chapman KE. Mol Cell Endocrinol. 2011;335(1):2–13
- Oakley RH & Cidlowski JA. J Biol Chem. 2013;288:22361–22369
- Czock D et al. Clin Pharmacokinet. 2005;44(1):61–98
- UpToDate: “Pharmacology of corticosteroids” 2024
- Herold MJ et al. Blood. 2006;108(11):3609–3616
- Hideshima T et al. Oncogene. 2001;20:4519
- ASCO/MASCC Antiemesis Guidelines 2020
- Roila F et al. Ann Oncol. 2016;27(suppl 5):v119–v133
- Newton R. Thorax. 2000;55:603–613
- Schmidt S et al. Leukemia. 2004;18:1835–1845
- Löwenberg M et al. Steroids. 2008;73:1016–1021
- FDA Prescribing Information: Decadron, Solu-Medrol, Deltasone
- Frey BM & Frey FJ. Clin Pharmacokinet. 1990;19(4):285–308
- Veal GJ et al. Clin Pharmacokinet. 2003;42(6):557–574
- Coiffier B et al. NEJM. 2002;346(4):235–242
- Wilson WH et al. NEJM. 2012;367(15):1397–1408
- NCCN B-Cell Lymphomas v5.2024
- Engert A et al. NEJM. 2010;363(7):640–652 (HD18 GHSG trial)
- Moskowitz CH et al. Blood. 1999;93(10):3469–3477
- Josting A et al. Ann Oncol. 2002;13(10):1628–1635
- Rajkumar SV et al. Lancet Oncol. 2010;11(1):29–37
- Durie BGM et al. SWOG S0777. NEJM 2017
- Facon T et al. MAIA. NEJM 2019
- Dimopoulos M et al. CASTOR. NEJM 2016
- NCCN Multiple Myeloma v4.2025
- IMWG Frailty Score
- Palumbo A et al. Leukemia. 2015;29(9):1820–1827
- Bostrom BC et al. CCG-1961. Blood. 2003;101(10):3809–3817
- Mitchell C et al. Blood. 2005;106(7):2428–2433
- NCCN Acute Lymphoblastic Leukemia v1.2025
- Stock W et al. Blood. 2019;133(14):1548–1559
- Magrath I et al. JCO. 1996;14(3):925–934
- Kantarjian HM et al. JCO. 2004;22(7):1209–1218
- Castro JE et al. Leukemia. 2008;22(11):2048–2053
- NCCN CLL/SLL v2.2025
- Ruutu T et al. Bone Marrow Transplant. 2014;49(2):168–173 (EBMT/ELN guidelines)
- Martin PJ et al. Biol Blood Marrow Transplant. 2012;18(8):1150–1163
- Zeiser R et al. REACH2. NEJM. 2020;382(19):1800–1810
- Flowers MED & Martin PJ. Hematology ASH Education Book. 2015;2015(1):98–107
- Neunert C et al. ASH ITP Guidelines. Blood. 2019;133(23):2386–2393
- Provan D et al. Blood Adv. 2019;3(22):3780–3817
- Jäger U et al. ASH AIHA Guidelines. Blood Adv. 2020;4(7):1559–1577
- Hesketh PJ et al. ASCO Antiemesis Guidelines. JCO. 2020;38(24):2782–2797
- MASCC/ESMO Antiemetic Guidelines 2023
- Loblaw DA et al. JCO. 2005;23(9):2028–2037 |
- NCCN Palliative Care v1.2024
- Shah M et al. Br J Haematol. 2004;126(6):756–761
- Baden LR et al. ASCO OI Prevention Guidelines. JCO. 2013;31(31):e400–e427
- Maret-Ouda J et al. JAMA Intern Med. 2018
- NCCN Prevention of Infections v1.2025
- Cornely OA et al. ASPECT trial. NEJM. 2007;356(4):348–359
- NCCN Prevention and Treatment of Cancer-Related Infections v1.2025
- Palumbo A et al. Leukemia. 2008;22(2):414–423
- NCCN Multiple Myeloma v4.2025
- Lyman GH et al. ASH VTE Guidelines. Blood. 2021;138(4):344–380
- Buckley L et al. ACR GIO Guidelines. Arthritis Rheumatol. 2017;69(8):1521–1537
- NCCN Bone Health v2.2024
- Piper JM et al. Ann Intern Med. 1991;114(9):735–740
- American College of Gastroenterology (ACG) Guidelines 2022
- Dinsen S et al. Eur J Intern Med. 2013;24(6):499–503
- Nieman LK. UpToDate. 2024 “Glucocorticoid withdrawal”
- Lexicomp Drug Interactions 2024
- Micromedex 2024
- Lexi-interact
- FDA Prescribing Information (Decadron, Deltasone)
- Löscher W & Potschka H. Prog Neurobiol. 2005;76:22–76
- NCCN Prevention of Infections v1.2025
- Krishna G et al. Clin Pharmacol Ther. 2009;86(2):187–194
- Saag KG et al. NEJM. 1994;330(25):1776–1781
- ACR GIO Guidelines 2022
- NCCN Supportive Care v2.2024
- Kwon S & Hermayer KL. Am J Med Sci. 2013;345(4):274–277
- Jacobs DM et al. Endocr Pract. 2014
- AACE/ADA Consensus on Inpatient Hyperglycemia 2009
- Kumar SK, Harrison SJ, Cavo M, et al. Venetoclax or placebo in combination with bortezomib and dexamethasone in patients with relapsed or refractory multiple myeloma (BELLINI): a randomised, double-blind, multicentre, phase 3 trial. Lancet Oncol. 2020;21(12):1630-1642. doi:10.1016/S1470-2045(20)30525-8 [PubMed 33129376]
- FDA Venclexta PI 2024
- Raje N et al. Lancet Oncol. 2018
- Shoenfeld Y et al. JAMA. 1981;245(15):1545–1549
Leave a Reply