All dosing and clinical decisions require verification against current package inserts and institutional protocols.
| 1st gen | 2nd gen | 3rd gen |
|---|---|---|
| Imatinib (May 2001) | Dasatinib (June 2006) Nilotinib (Oct 2007) Bosutinib (Sept 2012) | Ponatinib (Dec 2012) Asciminib (Oct 2021; STAMP inhibitor, allosteric) |
KEY CLINICAL PARAMETERS
- Dose (ALL): 400–800 mg once daily
- Food: Take WITH food (reduces GI SE)
- CYP: CYP3A4 substrate + inhibitor
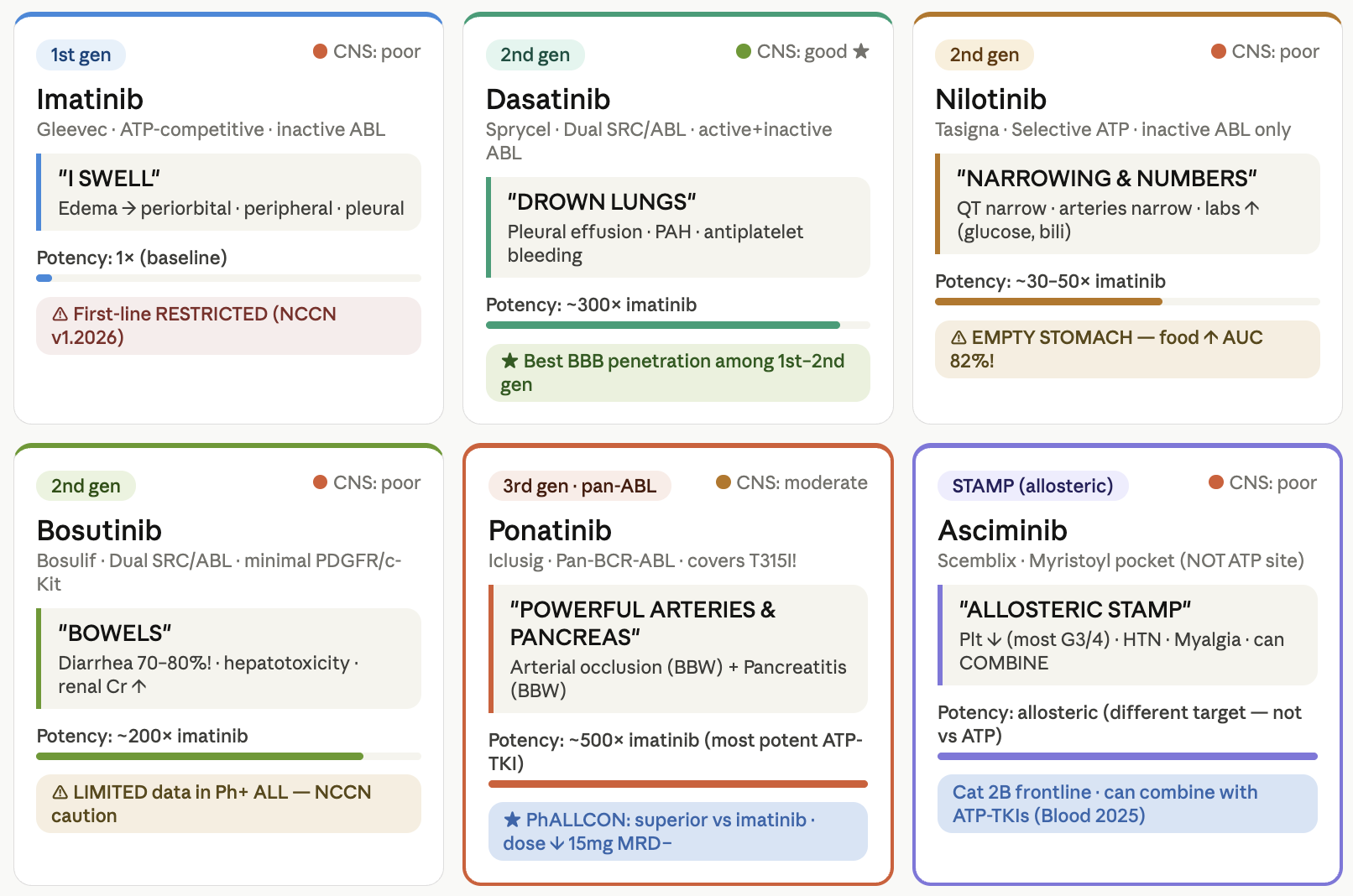
- CNS: Poor (~1–3% of plasma)
- BBW: Hepatotoxicity, edema/fluid
- NCCN 2026: Restricted — only if cannot tolerate broader TKIs
TOXICITIES
- Edema/weight gain ★★
- Nausea/vomiting
- Myalgia/cramps
- Hepatotoxicity (LFT ↑)
- Rash/dermatitis
- Myelosuppression
- Pleural effusion (rare)
RESISTANCE MUTATIONS (NCCN)
Too numerous to list (many point mutations across P-loop, T315I, and activation loop) — most other TKI resistance mutations also confer imatinib resistance. PhALLCON: inferior MRD vs ponatinib (Jabbour E, JAMA 2024).
KEY CLINICAL PARAMETERS
- Dose (ALL): 140 mg daily; 70 mg BID (R/R)
- Food: No significant restriction
- CYP: CYP3A4 substrate
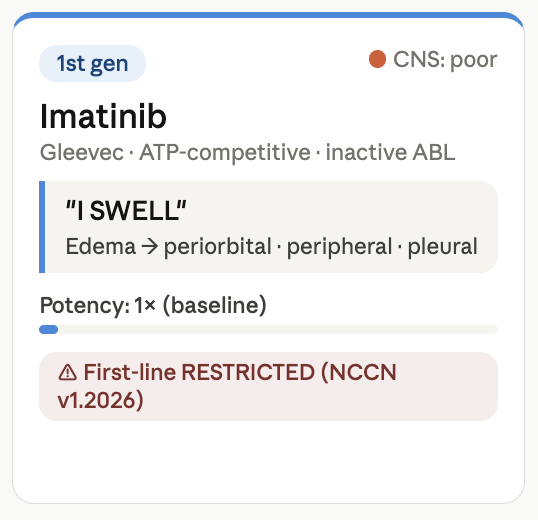
- CNS: GOOD ★ — best 1st/2nd gen BBB
- BBW: Bleeding; pulmonary HTN
- SRC inhibition: Yes — additional ALL benefit
- Correct before initiation: hypokalaemia, hypomagnesaemia, and uric acid.
TOXICITIES
- Pleural effusion ★★ (most distinctive)
- Pulmonary arterial HTN (PAH)
- Bleeding (antiplatelet effect)
- Thrombocytopenia
- Diarrhea
- QTc prolongation (mild)
- Peripheral edema
RESISTANCE MUTATIONS (NCCN)
T315I/A · F317L/V/I/C · V299L
Unique advantage in Ph+ ALL: CNS penetration + SRC kinase inhibition. CNS prophylaxis is mandatory in all ALL patients; dasatinib provides systemic CNS coverage, supplementing IT therapy.
KEY CLINICAL PARAMETERS
- Dose (ALL): 300–400 mg BID
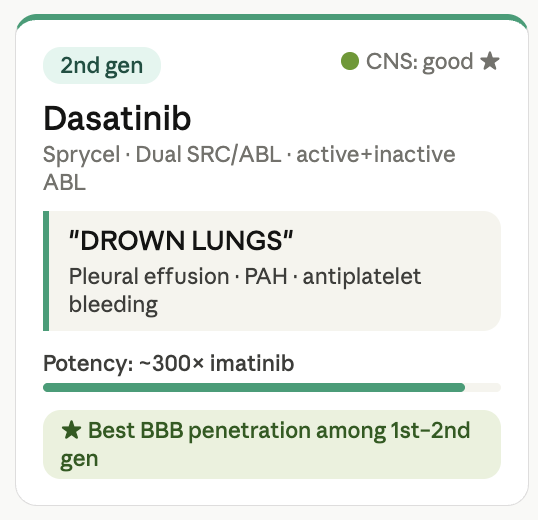
- Food: ⚠ EMPTY STOMACH: 2h before / 1h after food. Food ↑ AUC by 82%!
- CYP: Strong CYP3A4 inhibitor + substrate; UGT1A1
- QTc monitor: Baseline + periodic ECG required
- CNS: Poor (minimal BBB penetration)
- BBW: QT prolongation + sudden death; PAOD
TOXICITIES
- QTc prolongation ★★ (BBW)
- PAOD/PAD (BBW)
- Hyperglycemia / new-onset DM, Hyperbilirubinemia, Hyperlipidemia
- Pancreatitis, Hepatotoxicity
- Rash
RESISTANCE MUTATIONS (NCCN)
T315I · Y253H · E255K/V · F359V/C/I · G250E
Pharmacist critical: Avoid QT-prolonging drugs concurrently (ondansetron, azithromycin, fluoroquinolones, methadone, haloperidol). Avoid strong CYP3A4 inhibitors (azole antifungals — voriconazole, fluconazole). PPI interaction: per NCCN ALL guidelines, gastric acid suppression can affect bioavailability of certain BCR-ABL TKIs.
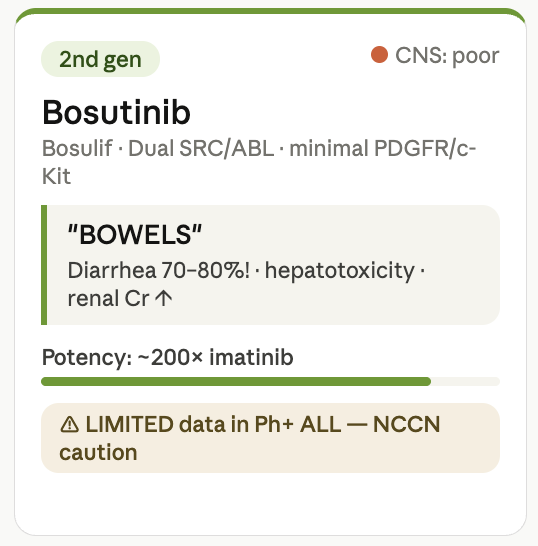
KEY CLINICAL PARAMETERS
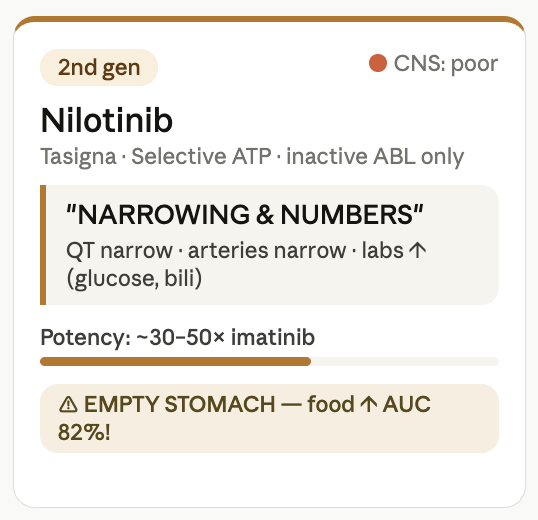
- Dose (ALL): 500 mg daily (CML-based; limited ALL data)
- Food: Take WITH FOOD (↓ GI toxicity) — opposite of nilotinib!
- CYP: CYP3A4 substrate
- CNS: Poor
- BBW :Hepatotoxicity (LFT monitoring)
- NCCN note: Limited data in Ph+ ALL specifically
TOXICITIES
- Diarrhea ★★ (70–80% incidence!)
- Nausea/vomiting
- Hepatotoxicity (ALT/AST ↑) — BBW
- Serum creatinine ↑
- Edema (less than imatinib)
- Rash
- Myelosuppression
RESISTANCE MUTATIONS (NCCN)
T315I · V299L · G250E · F317L
NCCN v1.2026 explicitly states: “limited data for bosutinib in Ph+ ALL.” Exercise caution when applying CML data directly. Diarrhea may worsen with concurrent antibiotics/gut-toxic regimens. Monitor LFTs closely q2 weeks for first 3 months.
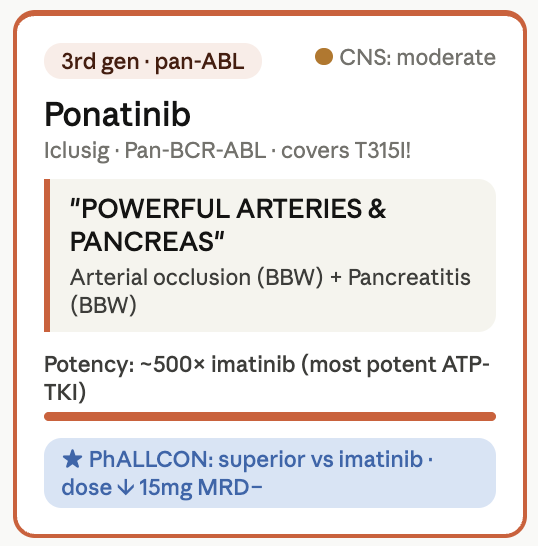
KEY CLINICAL PARAMETERS
- Dose (ALL): 30–45 mg daily initially
- NCCN dose ↓: Reduce to 15 mg once MRD-negative to minimize vascular risk
- Food: No significant restriction
- CYP: CYP3A4 substrate; P-gp inhibitor
- CNS: Moderate (better than nilotinib)
- Trial PhALLCON: superior MRD vs imatinib (JAMA 2024)
- T315I: Covers T315I — no resistance mutations per NCCN
TOXICITIES
- Arterial occlusion: MI/stroke/PAD ★★ (BBW)
- Pancreatitis ★ (BBW)
- Hypertension, Venous thrombosis, Heart failure
- Hepatotoxicity
- Myelosuppression
- Rash/dry skin
RESISTANCE MUTATIONS (NCCN)
NONE — covers all known BCR-ABL mutations including T315I at standard dosing per NCCN v1.2026
Pre-existing cardiovascular disease, hypertension, hyperlipidemia, DM, or smoking history are HIGH-RISK features. Assess cardiovascular risk before initiating. Monitor BP closely. The dose de-escalation to 15mg once MRD-negative is a NCCN-mandated strategy to minimize vascular toxicity (referenced from package insert).
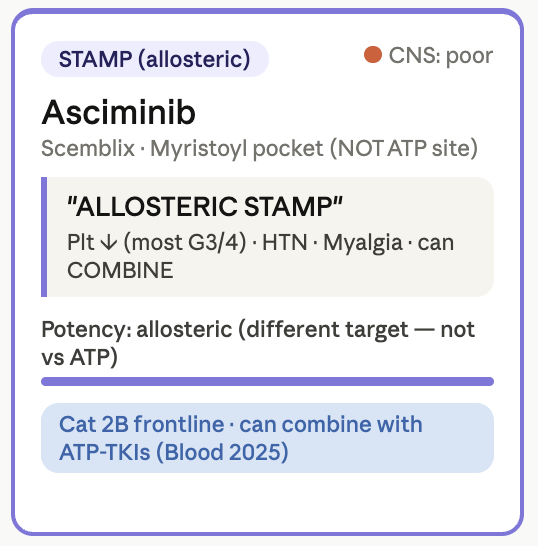
KEY CLINICAL PARAMETERS
- Dose (standard): 40 mg BID (fasting)
- Dose (T315I): 200 mg BID (with or without food)
- NCCN ALL (FL): Cat 2B — intolerance/CI to multiple other TKIs
- NCCN ALL (R/R): Recommended ± another TKI
- Combination: Can add to other TKIs (Luskin, Blood 2025)
- CYP: CYP3A4 inhibitor (moderate)
- CNS Poor (limited data)
TOXICITIES
- Thrombocytopenia ★ (most common G3/4)
- Hypertension
- Pancreatitis
- Rash
- Myalgia/arthralgia
- Fatigue
- Neutropenia, URTI (infections)
RESISTANCE MUTATIONS (NCCN)
A337T · P465S · M244V · F359V/I/C — entirely different from ATP-competitive TKI resistance mutations. Mutation profiling is critical before/during therapy.
Unique advantage: can combine with any ATP-competitive TKI for dual-site BCR-ABL inhibition. The combination targets both the ATP pocket and myristoyl pocket simultaneously — different resistance profiles mean combining may overcome resistance to either agent alone (Luskin MR, Blood 2025;145:577-589).
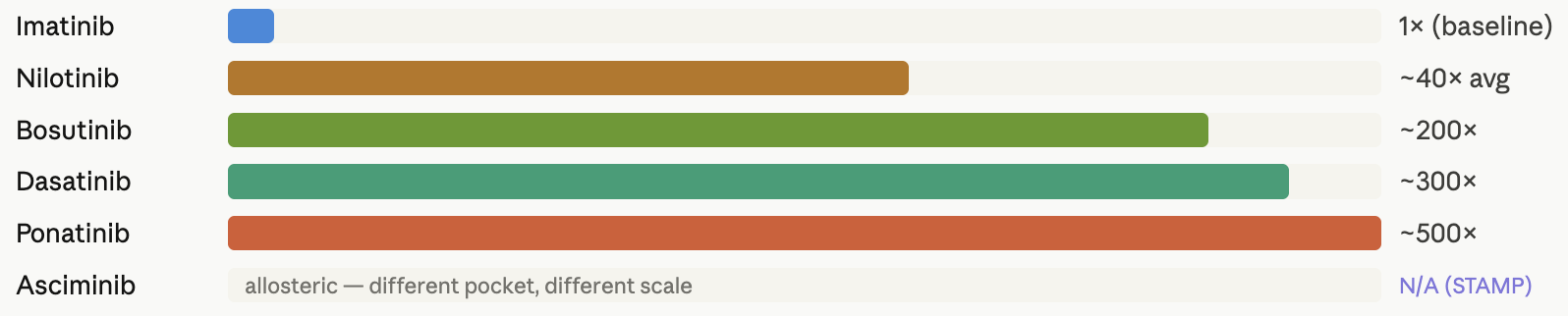
Potency Comparison
BCR-ABL mutation resistance profile (NCCN v1.2026 — ALL-D 2 of 29)
| TKI | Mutations associated with resistance (NCCN ALL v1.2026) | T315I covered? |
|---|---|---|
| Imatinib | Too numerous to list (many P-loop, activation loop mutations) | No |
| Dasatinib | T315I/A · F317L/V/I/C · V299L | No (T315I resists) |
| Nilotinib | T315I · Y253H · E255K/V · F359V/C/I · G250E | No |
| Bosutinib | T315I · V299L · G250E · F317L | No |
| Ponatinib | None — covers all known mutations | YES ★★ (only 1) |
| Asciminib | A337T · P465S · M244V · F359V/I/C (different profile; T315I covered at 200mg BID) | Yes — at 200 mg BID only |
Interactions
| TKI | Food effect | PPI/antacid interaction | Key CYP interaction |
|---|---|---|---|
| Imatinib | Take WITH food (↓ GI SE) | Minimal (pH-independent absorption) | CYP3A4 sub + inhibitor; CYP2D6 inhibitor |
| Dasatinib | No restriction | PPIs/antacids reduce absorption (pH-dependent). Separate by 2h if unavoidable. | CYP3A4 substrate (strong); avoid azole antifungals |
| Nilotinib | FAST: 2h before / 1h after food. AUC ↑82%! | PPIs ↓ absorption. Avoid if possible. NCCN ALL highlights this interaction. | Strong CYP3A4 inhibitor + substrate; UGT1A1 inhibitor → bilirubin ↑ |
| Bosutinib | Take WITH food (500-calorie meal; ↓ diarrhea) | Minimal data | CYP3A4 substrate |
| Ponatinib | No restriction (with/without food) | Minimal | CYP3A4 substrate; P-gp inhibitor; mild CYP3A4 inhibitor |
| Asciminib | 40mg BID: fasting preferred. 200mg BID (T315I): with or without food | Minimal data | CYP3A4 inhibitor (moderate); CYP2C9 inhibitor |
Pharmacist Critical Watchouts
1. NCCN v1.2026 — Imatinib restriction (NEW): First-line use should be RESTRICTED to patients who cannot tolerate broader-acting TKIs. Do NOT default to imatinib as “safer” — it is now the option of last resort for upfront Ph+ ALL. Challenge any prescription of imatinib as first-line in a patient who could tolerate dasatinib or ponatinib.
2. Ponatinib — mandatory dose de-escalation (NCCN): Once MRD-negative remission is achieved, reduce ponatinib to 15 mg daily. Failure to de-escalate = unacceptable cardiovascular risk. Per NCCN: “Reducing ponatinib to the lowest effective dose per protocol (15 mg) once MRD-negative remission is achieved is an appropriate strategy to minimize cardiac and/or vascular toxicity.” Verify dose reduction occurred — flag if patient remains on 30–45 mg post-MRD negativity.
3. Nilotinib — food = toxicity trap: Food (especially high-fat meal) increases nilotinib AUC by 82% and Cmax even more. This is NOT a “take with food to reduce SE” situation — it is an overdose risk. Educate every patient and caregiver. Document fasting requirement explicitly on discharge prescription. Separate from all medications requiring food.
4. PPI/antacid interaction with dasatinib and nilotinib: NCCN explicitly highlights this. PPIs significantly reduce absorption of pH-dependent TKIs. If acid suppression is required, use lowest-frequency PPI possible or switch to H2 blocker (with 12h separation from nilotinib). Flag at every medication reconciliation and discharge review.
5. Mutation profiling before and during TKI therapy: ABL1 kinase domain mutation testing is mandatory per NCCN at diagnosis AND with resistance/progression. Testing may be less sensitive with minimal disease burden. Without mutation data, TKI selection is empiric. T315I = only ponatinib or asciminib at 200mg BID. V299L on dasatinib = switch to bosutinib or nilotinib. F317L on bosutinib = switch to dasatinib or nilotinib.
6. Asciminib — Category 2B in ALL frontline (know when it applies): Only indicated frontline if intolerance or contraindication to MULTIPLE other TKIs. In R/R setting, can be used alone or in combination with another TKI (Luskin, Blood 2025). The 40mg BID dose does NOT reliably cover T315I — escalate to 200mg BID if T315I confirmed.
7. Dasatinib for CNS-involved Ph+ ALL: All ALL patients require CNS prophylaxis. Dasatinib is the TKI with best CNS penetration among 1st–2nd gen TKIs. If patient has CNS disease or is at high CNS risk, dasatinib + IT therapy should be strongly considered. Ponatinib has moderate CNS penetration as an alternative if T315I or CNS-resistant disease.
8. Cardiovascular risk stratification before ponatinib: Pre-existing CAD, stroke history, PAD, uncontrolled HTN, DM, hyperlipidemia, or active smoking are major risk factors for ponatinib vascular events. Perform CV risk assessment (and document) at every tumor board. Ensure BP controlled before initiating. Monitor lipid panel, glucose, BP throughout.
9. Bosutinib diarrhea management: Prophylactic antidiarrheal therapy (loperamide) should be considered from cycle 1. Ensure patient takes WITH food. Aggressive electrolyte monitoring (K+, Mg2+) with persistent diarrhea. Dose reduction algorithm: Grade 2 = interrupt; Grade 3–4 = interrupt + reduce when recovered.
10. QTc monitoring for nilotinib (and dasatinib): Obtain baseline ECG for ALL patients before nilotinib. Repeat after 7–14 days and after dose changes. QTcF >480ms = withhold; >500ms = discontinue. Create a list of all QT-prolonging co-medications on every chemo review. Hypokalemia and hypomagnesemia AMPLIFY QTc risk — correct electrolytes aggressively.
Clinical pearls — step-by-step competency builder
The TKI selection algorithm in Ph+ ALL is mutation-driven, not default-based. Per NCCN v1.2026: use of a specific TKI should account for anticipated/prior TKI intolerance, dose used, BCR-ABL1 mutations, and disease-related features. Always check mutation status before selecting or switching TKI.
Imatinib is now LAST LINE in first-line Ph+ ALL (NCCN v1.2026). Restricted to patients who cannot tolerate broader-acting TKIs. Do not use imatinib upfront if the patient can tolerate dasatinib, nilotinib, bosutinib, or ponatinib. PhALLCON confirmed ponatinib is superior to imatinib (Jabbour, JAMA 2024).
T315I (“gatekeeper mutation”) = only ponatinib (standard dose) or asciminib 200mg BID. All other TKIs are resistant to T315I. If T315I is detected at any point, switch immediately. T315I is the most important resistance mutation to recognize clinically.
Blinatumomab + TKI is PREFERRED in consolidation for MRD-positive Ph+ ALL (NCCN v1.2026). Also strongly considered even in MRD-negative patients who have not previously received blinatumomab. TKI backbone continues throughout. As pharmacist: ensure TKI is bridged appropriately during blinatumomab infusion and dose interruptions.
Ponatinib dose de-escalation to 15mg once MRD-negative is a NCCN-mandated patient safety strategy. This is not a discretionary clinical decision — it is in the NCCN guideline. Failure to reduce dose is a medication safety issue. Verify at every refill and chemo review post-MRD negativity.
Asciminib is the only allosteric TKI — its power is in COMBINATION. Because it binds the myristoyl pocket (not the ATP site), combining it with any ATP-competitive TKI targets BCR-ABL at two binding sites simultaneously. This combination strategy is emerging as a tool to prevent/overcome resistance. Luskin et al., Blood 2025;145:577-589 supports asciminib combinations in ALL.
CNS prophylaxis is mandatory in ALL — factor in TKI CNS penetration. Per NCCN: “ALL treatment regimens include CNS prophylaxis.” While IT therapy is the cornerstone, dasatinib provides meaningful systemic CNS TKI coverage. In CNS-positive disease or high CNS risk (CNS-3, high WBC), dasatinib is pharmacologically preferred over nilotinib or imatinib.
Myelosuppression from TKI can confound treatment — NCCN specifically flags this. Per NCCN footnote bb: “Assess for myelosuppression secondary to TKI and consider dose reduction” before concluding marrow failure. Do not automatically attribute cytopenia to disease — it may be TKI-induced. Dose reduction may be appropriate before changing antileukemic strategy.
Nilotinib + food is an overdose scenario, not a comfort measure. The food effect (82% AUC increase) is clinically dangerous. This is in sharp contrast to bosutinib (must take WITH food to reduce GI toxicity). Knowing which TKI to take WITH food vs WITHOUT is a fundamental pharmacist competency point for counseling and preventing medication errors.
Asciminib resistance mutations are completely different from ATP-TKI resistance mutations. This is a critical strategic point: if a patient develops resistance to dasatinib (e.g., F317L), they may retain sensitivity to asciminib. If they develop asciminib resistance (A337T), they may retain sensitivity to ATP-competitive TKIs. Combining both eliminates this vulnerability — the rationale for combination therapy.
PhALLCON regimen is now in NCCN v1.2026 as an “other recommended” option. Ponatinib + mini-HCVD showed superior MRD responses vs imatinib + mini-HCVD. Jabbour E, JAMA 2024;331:1814-1823. Know this trial when discussing frontline TKI selection at tumor board.
ABL1 kinase domain mutation testing timing matters. Per NCCN: less sensitive in minimal disease burden. Optimal testing = at diagnosis (bone marrow), at resistance/progression, and when switching TKI. Results guide TKI selection and should be part of every tumor board discussion for Ph+ ALL patients with inadequate response.
References
- NCCN ALL Guidelines v1.2026 (April 8, 2026)
- Jabbour E et al. JAMA 2024;331:1814-1823 (PhALLCON)
- Luskin MR et al. Blood 2025;145(6):577-589 (asciminib combinations)
- Mutation profile: NCCN ALL-D 2 of 29.
Leave a Reply