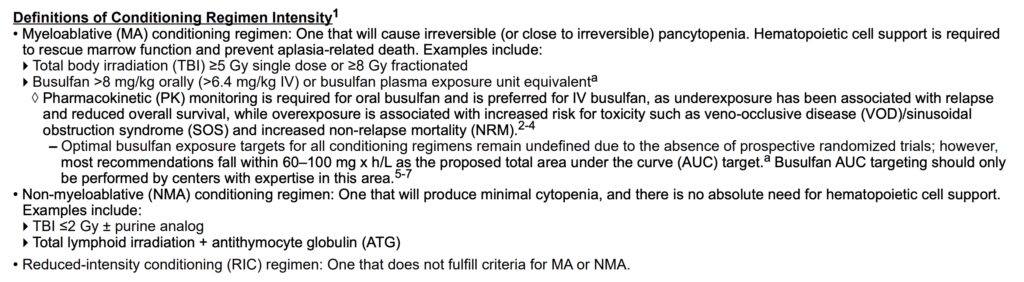
HCT Indication
Conditioning Regimens
Pre-Transplant Recipient Evaluation (NCCN HCT-2/HCT-3)
Clinical Assessment (Mandatory)
| Assessment | Details & Pharmacist Relevance |
|---|---|
| Histologic Diagnosis Confirmation | Confirm pathology, cytogenetics, molecular testing (MRD status, FLT3, IDH, NPM1 in AML) |
| Performance Status | ECOG or Karnofsky (KPS) — determines conditioning intensity tolerance |
| HCT-CI Score | Calculator: hctci.org — predicts NRM. Score 0 = low risk, ≥3 = high risk. Does NOT predict relapse. |
| PFTs (Spirometry, Lung Volumes, DLCO) | DLCO corrected for Hgb (Dinakara method). DLCO <60% → pulmonary consult. Caution with busulfan, carmustine, HD-TBI. |
| Cardiac Evaluation | ECG with QTc. LVEF by ECHO or MUGA. Consult if compromised LVEF (especially for anthracycline/cyclophosphamide risk). |
| Renal Function | CrCl/eGFR essential — CNIs cause renal failure, dose adjustments needed. 24-hr urine if borderline or low muscle mass. |
| Liver Function | LFTs, bilirubin. Cirrhosis with portal HTN = contraindication for allo-HCT. Baseline for VOD/SOS risk stratification. |
| Fertility Preservation | Discuss BEFORE conditioning (irreversible gonadal damage from HD-alkylators). Refer reproductive endocrinology. |
| Psychosocial Evaluation | Assess medication adherence, high-risk behaviors, caregiver availability. CNI compliance is CRITICAL. |
| Geriatric Assessment | For older adults — consider HCT-specific tools. Physiological not chronological age drives eligibility. Category 2B. |
Laboratory Tests (All Patients)
| Test | Purpose / Notes |
|---|---|
| CBC with differential | Baseline cytopenias, disease burden |
| ABO/Rh Typing | ABO-mismatch between donor/recipient → manage hemolysis risk |
| Comprehensive Metabolic Panel | Glucose, Cr/eGFR, electrolytes, LFTs (transaminases + bilirubin) |
| PT/PTT | Baseline coagulation — liver biopsy risk assessment if needed for VOD workup |
| Infectious Serology | CMV, HSV, VZV, HBV, HCV, HIV, syphilis, Toxoplasma (for allo-HCT) |
| HLA Typing | Per FACT-JACIE International Standards. High-resolution required for MUD search |
| STR Genotyping (Allo only) | Donor + recipient genotyping for post-transplant CHIMERISM analysis (NEW in v1.2026) |
| Anti-HLA Antibodies (if MMUD) | Donor-specific antibodies (DSA) → risk of primary graft failure |
Additional Evaluation (As Clinically Indicated)
| Test | When, Notes |
|---|---|
| Bone Marrow Biopsy | Confirm remission. For acute leukemia: within 4 WEEKS of conditioning start. |
| Lumbar Puncture/CSF | CNS disease workup in ALL, aggressive NHL |
| Pregnancy Test | All individuals of childbearing potential prior to conditioning |
| Iron Profile + Ferritin | Iron overload (esp. multiply transfused patients) — hepatic risk pre-HCT |
| Vitamin D level | Supplement if deficient — bone health especially with anticipated steroid use |
| TSH | Baseline prior to TBI-containing regimens (post-TBI hypothyroidism) |
| VOD/SOS Risk Calculator | CIBMTR tool: cibmtr.org — stratify VOD risk pre-conditioning |
PHARMACIST WATCHPOINT: DLCO CORRECTION: Always verify DLCO is corrected for hemoglobin using the Dinakara method. An uncorrected DLCO in an anemic patient will appear falsely low, potentially restricting busulfan or carmustine use inappropriately.
CLINICAL PEARL: HCT-CI vs. AGE: The HCT-CI predicts NRM MORE ACCURATELY than age alone. A 70-year-old with HCT-CI 0 may tolerate MA conditioning better than a 55-year-old with HCT-CI ≥5. Don’t let age alone decide.
POST-TRANSPLANT FOLLOW-UP & COMPLICATIONS (NCCN HCT-C)
Post-Transplant Monitoring Framework
| Phase | Monitoring Focus | Pharmacist Actions |
|---|---|---|
| Early (<Day 30) | • Engraftment (ANC >500 × 2 days) • Mucositis, infections (bacterial esp.) • Organ toxicity (renal, liver, cardiac) • VOD/SOS risk surveillance • Hemorrhagic cystitis (if PTCy/Cy) | • Daily CBC, CMP, Mg, CMV PCR • Mucositis scale assessment • Dose-adjust CNIs, antimicrobials • Busulfan AUC if applicable • Mesna dosing if PTCy/Cy used |
| Day 30–100 | • GVHD (skin, GI, liver) • CMV/EBV/viral reactivations • Graft rejection/chimerism • Immune reconstitution | • CNI TDM, taper per protocol • CMV preemptive therapy if needed • Adjust immunosuppression • GVHD supportive care management |
| Late (>Day 100) | • Chronic GVHD • Late infections (PCP, Aspergillus) • Secondary malignancy • Endocrinopathies (thyroid, adrenal) • Bone health (DEXA) • Cardiovascular risk | • cGVHD medication management • Immunization schedule (avoid live vaccines) • Steroid-related AEs management • Survivorship medications |
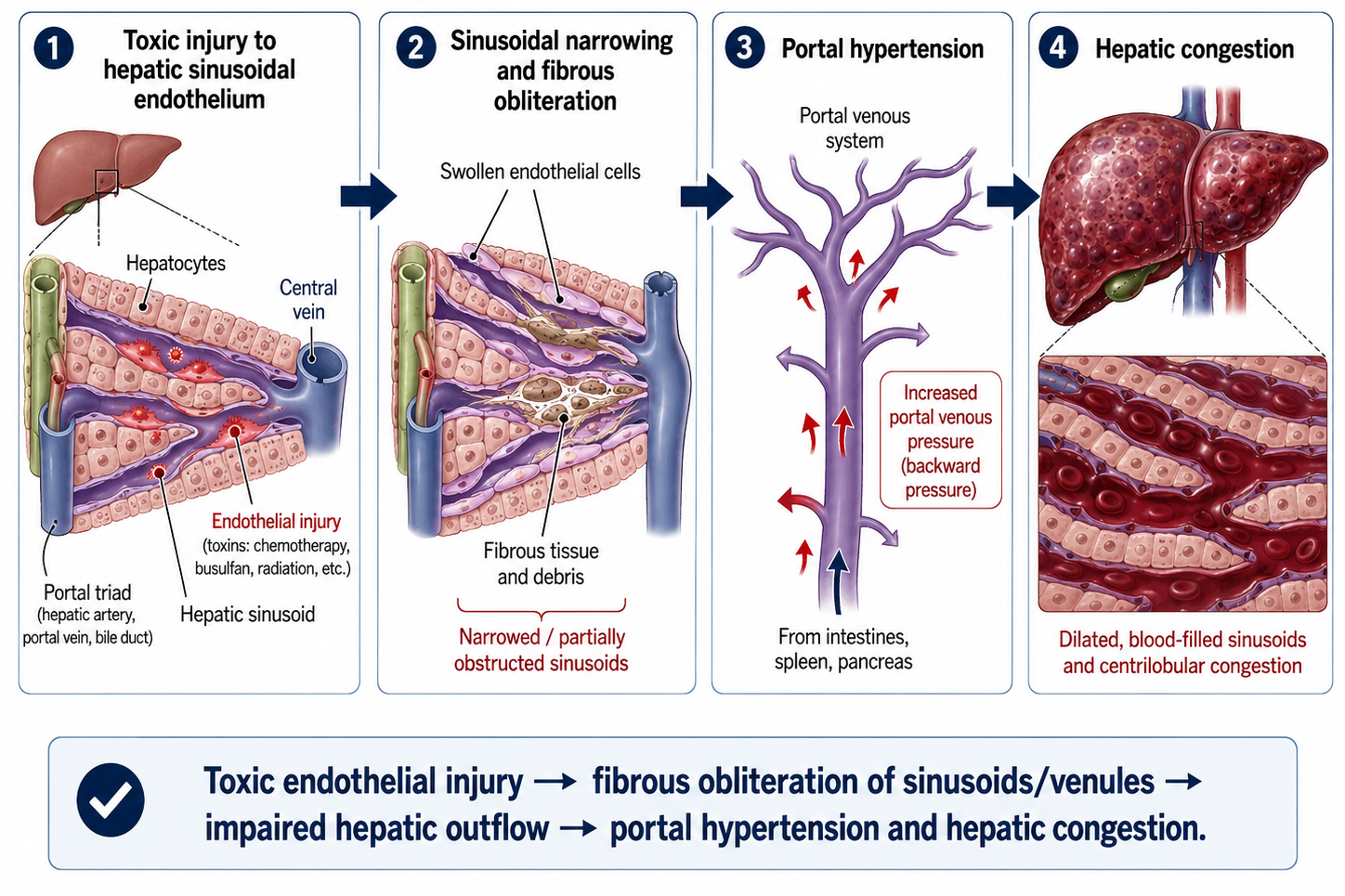
VOD/SOS (Veno-Occlusive Disease / Sinusoidal Obstruction Syndrome)
| Parameter | Details |
|---|---|
| Risk Factors | HD busulfan/TBI, prior liver disease, inotuzumab/gemtuzumab exposure, sirolimus + tacrolimus + MA conditioning, CIBMTR VOD score ≥2 |
| Classic Triad | 1. Painful hepatomegaly 2. Weight gain/ascites (>2% above baseline) 3. Jaundice (bilirubin >2 mg/dL) — within first 30 days post-HCT |
| EBMT Criteria (2016) | Classic VOD: <21 days post-HCT. Late-onset VOD: >21 days if etiology confirmed. Classic Triad OR 2 of 3 + histologic confirmation. |
| Treatment | DEFIBROTIDE (FDA-approved): For hepatic VOD/SOS with renal or pulmonary dysfunction. Dose: 6.25 mg/kg IV q6h × minimum 21 days. Duration: until resolution or up to Day +60 |
| Defibrotide Monitoring | • Hypotension (most common) • Bleeding risk (hold if active bleeding) • Drug interactions: anticoagulants (additive bleed risk) • No formal dose adjustment for hepatic/renal dysfunction in package insert |
DEFIBROTIDE: Do NOT confuse with deferiprone or deferoxamine. Defibrotide has thrombolytic/anti-inflammatory activity. Watch for CONCURRENT anticoagulants (heparin flushes, prophylactic heparin). If patient needs heparin, discuss with team — defibrotide + anticoagulants = high hemorrhage risk.
Chimerism Monitoring (Allo-HCT)
- Complete donor chimerism: >95% donor cells in myeloid + lymphoid compartments
- Mixed chimerism: 5–95% donor cells
- Absent donor chimerism: <5% — high graft rejection/failure concern
- Declining chimerism in AML/MDS → signals relapse risk → alert team
- Monitor by peripheral blood PCR (STR-based, per NCCN HCT-2 update: STR genotyping required pre-transplant)