Clinical Pearls
- Prevention is the key
- Emetogenicity Risk of chemotherapy
- Highly emetic risk chemotherapy IV: NK1 RA, 5-HT3 RA, dexamethasone ± lorazepam
- NK1 RA: Place in therapy is for prevention of CINV, not treatment of CINV. Largest benefit seen in delayed CINV setting.
- Corticosteroid antiemetic premedication should be avoided for 3–5 days prior to and 90 days after CAR T-cell therapies.
- Treat other underlying causes
- Consider H2 blockers or proton pump inhibitors to prevent dyspepsia – drug interaction with some anticancer medications
- Keep an eye on drug interactions with anticancer medications
Epidemiology
- Overall incidence of emesis (83%) with anticancer. With antiemetics, incidence is reduced to nausea (~35%) and vomiting (13%)
- Consequences of CINV: low QoL, dehydration, e- disturbance, anorexia/wt loss, low PS, low compliance
Clinical Presentation (Terminology)
| Nausea | Retching (dry heaves) | Vomiting (emesis) | Anticipatory vomiting | Breakthrough emesis | Refractory emesis |
| Awareness of discomfort that may or may not precede vomiting | Vomiting without the expulsion of vomitus | Ejection or expulsion of gastric contents through the mouth | Triggered by sights, smells, or sounds and is a conditioned response | (incidence 20%) Occurs despite prophylactic treatment or necessitates additional rescue medications | Emesis that occurs during treatment cycles when antiemetic prophylaxis or rescue therapy has failed in previous cycles |
Onset: Acute ≤24 hours and Delayed nausea >24h
Duration: at least 3 days for high-emetic risk and 2 days for moderate-emetic risk after the last dose of anticancer agents.
MOA:
- Nausea is accompanied by decreased gastric tone and decreased peristalsis
- Neurotransmitters: Serotonin, Substance P, Dopamine, Others (Neurokinin-1 (NK1), ACh, Corticosteroid, Histamine, Cannabinoid, Opioid)
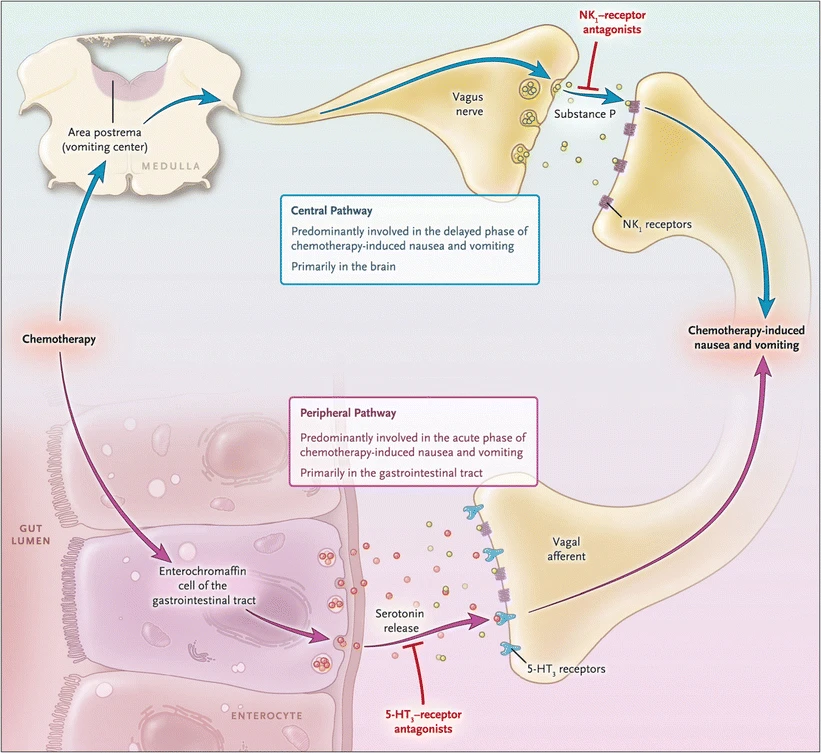
- Peripheral pathway (acute, serotonin, vomiting): Chemo triggers serotonin release in the GI tract, chemoreceptor trigger zone (CTZ), and pharynx, activating 5-HT3 and dopamine receptors on vagal afferents → signals the vomiting center (VC) in the medulla → vomiting + activation of salivation center, abdominal muscles, respiratory center, and cranial nerves.
- Central pathway (delayed, substance P, nausea): Chemo activates NK1 receptors in the CNS, leading to NV via a different mechanism.
- Anticipatory vomiting/nausea: triggered by sights, smells, or sounds, more common in patients with poor prior CINV control.
Risk factors
- Patient-related (< 50 [less exposure], female, motion sickness hx, morning sickness or N/V during pregnancy hx, poor control of NV in previous chemo cycles, little or no history of alcohol use)
- Emetogenicity (Hesketh model) – Choose highest risk in multi-cancer drugs
- Parenteral chemotherapy: minimal, low, moderate, high emetogenic risk
- Oral chemotherapy: prophylaxis recommended or as needed
- Radiation-induced NV: mild (head, neck, extremities), moderate (upper abdomen, pelvis, craniospinal radiation), high (total body irradiation, total nodal irradiation, upper-half-body irradiation))
Nonpharmacological therapy
- Lifestyle measures may help to alleviate nausea/vomiting, such as eating small frequent meals, choosing healthful foods, controlling the amount of food consumed, and eating food at room temperature.
- Avoid Greasing, spices.
- Aromatherapy (spearment)
- Seaband (motion sickness)
- BRAT (Bananas, rice, apple sauce, toast)
Pharmacological Therapy

Emetic Risk – Parenteral Emetic Risk Management
| Emetic Risk | Days | Option A (preferred) | Option B | Option C |
| High | Day1 | Olanzapine 2.5-10mg/day PO + NK1 RA (-pitant) + 5-HT3 RA (-setron) + Dexamethasone 12mg PO/IV | Olanzapine 2.5-10mg/day PO + Palonosetron 0.25mg IV + Dexamethasone 12mg PO/IV | NK1 RA (-pitant) + 5-HT3 RA (-setron) + Dexamethasone 12mg PO/IV |
| Day 2-4 | Olanzapine 2.5-10mg/day PO OR Aprepitant (if used on D1) 80mg/day PO D2-3 ± Dexamethasone 8mg/daily PO/IV | Olanzapine 2.5-10mg/day PO | Aprepitant (if used on D1) 80mg/day PO D2-3 OR Dexamethasone 8mg/daily PO/IV | |
| Moderate | Day1 | 5-HT3 RA (-setron) + Dexamethasone 12mg PO/IV | Olanzapine 2.5-10mg/day PO + Palonosetron 0.25mg IV + Dexamethasone 12mg PO/IV | NK1 RA (-pitant) + 5-HT3 RA (-setron) + Dexamethasone 12mg PO/IV |
| Day 2-3 | Dexamethasone 8mg/daily PO/IV OR 5-HT3 RA (-setron PO) | Olanzapine 2.5-10mg/day PO | Aprepitant (if used on D1) 80mg/day PO D2-3 ± Dexamethasone 8mg/daily PO/IV |
Low Emetic Risk: Dexamethasone, Metoclopramide, Prochlorperazine, or 5-HT3 RA
Minimal Emetic Risk: No routine prophylaxis
Dosing:
- Olanzapine 2.5-10mg/day PO
- NK1 RA
- Aprepitant 125 mg PO, Aprepitant 130 mg IV
- Fosaprepitant 150 mg IV
- Netupitant/palonosetron 300mg/0.5mg PO
- Fosnetupitant/palonosetron 235mg/0.25mg IV
- Rolapitant 180 mg PO
- 5-HT3 RA
- Dolasetron 100 mg PO
- Granisetron 10 mg SC or 2 mg PO or 0.01 mg/kg (max 1 mg) IV or 3.1 mg transdermal patch applied 24–48 h prior to first dose of anticancer therapy
- Ondansetron 16–24 mg PO or 8–16 mg IV once
- Palonosetron 0.25 mg IV
- Dexamethasone 12mg PO/IV (on D2-4: 8mg/day PO/IV)
Oral Emetic Risk Management
Moderate-High Emetic Risk (prophylaxis required): 5-HT3 RA or Olanzapine
Minimal-low Emetic Risk (PRN recommended): Metoclopramide, Prochlorperazine, or 5-HT3 RA
Serotonin receptor antagonist (5-HT3 RA; -setron)
- MOA: selective 5-HT3 receptor antagonist, blocking serotonin, both on vagal nerve terminals in the periphery and centrally in the chemoreceptor trigger zone
- Indication: acute, scheduled
- Administered prior to mod/severe emetogenic chemotherapy
- Side effects: headache and constipation
| Dose/Route | Pearls | |
| Palonosetron | IV: 0.25 mg once | • High efficacy for a 3-day chemo • Repeat doses is safe (0.25mg IV at 48-72h) but limited data on efficacy • Preferred in MEC without NK1 RA/olanzapine regimen • Substance P |
| Granisetron | ER SQ: 10 mg once weekly Oral: 2mg daily or 1 mg bid IV: 10 mcg/kg once Transdermal patch: 1 patch prior to and upto 24h after chemo – needs prior auth | • ER SQ once weekly (polymer-based drug delivery system) – administered in the clinic • ER SQ; preferred in MEC without NK1 RA/olanzapine regimen • Less headache than ondansetron due to more selective 5-HT • Patch: at home, a day before • Mostly paeds |
| Ondansetron | IV: 8 mg or 0.15 mg/kg (max 16 mg/day to avoid QT prolong (3-4 msec) Oral/ODT: 8 mg bid or 24 mg once IV:PO conversion 1:2 | • QT prolongation • Monitor LFT |
| Dolasetron | Oral: 100 mg within 1h prior | • Headache • QT prolongation (less but dose dependent) |
- Granisetron ER SQ:
- Single SQ 10 mg is non-inferior to single palonosetron 0.25mg IV for prevention of acute/delayed CINV post MEC/HEC; + dexamethasone.
- Single SQ 10 mg is superior to single ondansetron IV for prevention of delayed CINV post HEC; + fosaprepitant and dexamethasone.
- Clinical pearls:
- After receiving palonosetron, granisetron patch/ER SQ, breakthrough 5-HT3 RAs play a limited role in the delayed infusion period and breakthrough antiemetic should focus on a different MOA.
- Non-sedating; most common side effects are headache and constipation. Optimal effects seen with scheduled administration, not PRN use. Educate patients regarding constipation and its management.
- No further 5-HT3 therapy is required if palonosetron or granisetron ER SQ/patch is administered on day 1.
Neurokinin-1 receptor antagonists (NK1 RA; -pitant)
- MOA: inhibiting the substance P/neurokinin 1 (NK1) receptor; augments the antiemetic activity of 5-HT3 receptor antagonists and corticosteroids to inhibit acute and delayed phases of chemotherapy-induced emesis.
- Indication: Prevention (NOT ttt), delayed CINV; multiday admin
- DDI:
- All (except Rolapitant) inhibits metabolism of dexamethasone, thus increasing dexamethasone serum levels when administered concomitantly.
- Aprepitant/Fosaprepitant also inhibits/induce metabolism of Ifosfamide leading to increased neurotoxicity and decreased efficacy.
| Dose/Route | Pearls | |
| Aprepitant | IV: 130 mg 0.5h prior Oral: 125 mg 1h prior followed by 80 mg once daily | • Monitor LFT, INR, PT • Germline cancer on 5-day cisplatin regimen: aprepitant (125 mg D3, 80 mg D4–7) + 5-HT3 RA (D1–5) + dexamethasone (20 mg days 1, 2) • Limited data for PO on days 4-5 |
| Fosaprepitant | IV: 150 mg 0.5h prior (prodrug) | • Generic better/cheaper • Infusion-site reaction (Polysorbate 80) |
| Netupitant/ palonosetron | Oral: 1 capsule regimen | • Monitor LFT, RF • No need for 5-HT3 RA |
| Fosnetupitant/ palonosetron | IV: 235 mg/0.25 mg 0.5h prior | • Monitor LFT, RF • No need for 5-HT3 RA |
| Rolapitant | IV: 166.5 mg 2h prior Oral: 180 mg 2h prior Every 2 weeks | • DDI: CYP2D6 inhibitor (warfarin , OCP) • Extended t½ (q2w) – can be used in ifosfamide • Doesn’t inhibit dexamethasone metabolism (others do) • Infusion reaction |
- Aprepitant IV emulsion is a unique formulation of aprepitant and is NOT interchangeable with the IV formulation of fosaprepitant.
- NO available studies investigating repeat dosing of aprepitant IV emulsion, fosaprepitant, netupitant, fosnetupitant, and rolapitant.
Corticosteroids – Dexamethasone
- MOA of antiemesis is unknown – long-acting corticosteroids
- Dose (IV:PO):
- Day 1: 12 mg (with NK1 RA) or 20 mg (without NK1 RA)
- Day 2+: 8 mg once daily (with NK1 RA) or BID (without NK1 RA) in significant delayed emesis.
- IV >8mg: perianal itching – so give it as IV drip
- Administered in the morning (to minimize insomnia) and is given on chemo days
- Side effects: hyperglycemia (caution in DM), dyspepsia (H2RA for short duration, PPI for long duration), hiccups
- If intolerant to dexamethasone: consider olanzapine
- Dexamethasone-sparing strategies: For patients receiving MEC or non-cisplatin HEC, especially those patients with few identifiable (CINV) risk factors or who are intolerant to corticosteroids, limiting the administration of dexamethasone to day 1 only is an option that may not be associated with a significant reduction in antiemetic control.
- Clinical pearl: Extended delayed CINV: consider extending the course of delayed dexamethasone as clinically appropriate.
- Avoid corticosteroids for 3–5 days prior to and 90 days after CAR T-cell therapies. Upon disease progression, corticosteroids may be resumed if needed.
- CAR T cells’ ability to proliferate and work properly (Liu S et al. Blood Cancer J. 2020 Feb 6;10(2):15)
- Steroids may inhibit CAR T-cell persistence and their antimalignancy efficacy (Liu S et al. Blood Cancer J. 2020 Feb 6;10(2):15)
- Lower doses, given for shorter durations, or even elimination of dexamethasone on subsequent days (for delayed nausea and emesis prevention) may be acceptable based on patient characteristics.
Olanzapine (DA antagonist)
- MOA: second generation thienobenzodiazepine antipsychotic, antagonism of D2, 5-HT2C, and 5-HT3 receptors. Some cholinergic effect
- Indication: severe nausea, significant delayed emesis, intolerant to dexa – (AC Bca instead of dexa; antifungal DDI dexa)
- Side effects: sedation, dystonic reaction, QT prolongation; postural hypotension, anticholinergic side effects, fatigue
- DDI with Metoclopramide (category X)
- Dose is dependent on sedation: 10 mg > 5 mg > 2.5 mg – 5 mg is efficacious at bedtime (sedative)
- Suggest lower dose in high fall-risk patient, debilitated, frail, risk for orthostatic hypotension
- Give higher dose if ineffective, give lower dose if ADE
- Most notable on day 2 and improves over time
- Olanzapine may stimulate appetite, may consider 2.5 mg of olanzapine for patients experiencing concurrent chemotherapy-related anorexia [new addition to NCCN 2024, Sandhya 2023]
Benzodiazepines
- MOA: Binds to stereospecific BDZ R on the postsynaptic GABA neuron at several sites within the CNS (limbic system, reticular formation); shifts in Cl-, results in hyperpolarization (a less excitable state) and stabilization.
- Pancreatic cancer with other meds in BDZ
- Side effects: CNS depression (use caution in elderly, frail and those at high risk of fall)
- Indication: anticipatory CINV or when breakthrough CINV has an anxiety component
| Lorazepam | |
| Dose/Route | PO/IV/SL: 0.5–2 mg every 6 hours on days 1–4 |
| Pearls | • Anticipatory /anxiety • Caution with opioid (resp depression) • Caution with high fall risk/old/frail/dependence (CNS depression) |
Phenothiazine (DA antagonist)
- MOA: muscarinic-blocking effect may be responsible for antiemetic activity
- Side effects: CNS depression (use caution in elderly, frail and those at high risk of fall), dystonic reaction (give diphenhydramine 25–50 mg PO/IV q4-6h
| Promethazine | Prochlorperazine (COMPAZINE) | |
| Dose/Route | Suppository (rectum): 25 mg every 6 h Oral: 12.5–25 mg every 4–6 h | Suppository (rectum): 25 mg every 12 h Oral/IV: 10 mg every 6 h |
| Pearls | • More histamine blockage ~ more sedating • IV: severe tissue injury | Gives 2 weeks to give real effect |
Metoclopramide (DA antagonist): PO/IV: 10–20 mg every 4-6h PRN
- MOA: blocks DA R and (when given in higher doses) also blocks serotonin R in CTZ of the CNS
- Indication: gastroparesis (increases gut motility), parenteral/oral LEC, breakthrough
- Side effects:
- CNS depression (use caution in elderly, frail and those at high risk of fall)
- Dystonic reaction: give diphenhydramine 25–50 mg PO/IV either every 4 or every 6 h
- QT prolongation
- Tardive dyskinesia: risk increases with increasing cumulative doses and duration of treatment FDA recommends <12 weeks therapy
Haloperidol (DA antagonist): PO/IV: 0.5-2 mg every 4-6h
- MOA: butyrophenone antipsychotic that nonselectively blocks postsynaptic D2 R in the brain
- Indication: breakthrough, refractory
- Lower doses to produce antiemetic compared to antipsychotic doses
- Side effects:
- CNS depression (use caution in elderly, frail and those at high risk of fall)
- Dystonic reaction: give diphenhydramine 25–50 mg PO/IV either every 4 or every 6 h
- QT prolongation (some data: lower doses don’t prolong QT)
Scopolamine: Transdermal patch: 1 patch (1.5 mg) every 72 h
- MOA: Blocks the action of ACh at parasympathetic sites in smooth muscle, secretory glands and the CNS; increases CO, dries secretions, antagonizes histamine and serotonin
- Indication: breakthrough, motion issues (positional changes, movement, or excessive secretions are triggering episodes of N/V)
- Positional changes, movement, or excessive secretion
- Side effects:
- CNS depression (use caution in elderly, frail and those at high risk of fall)
Cannabinoid
- MOA: activates cannabinoid receptors CB1 and CB2.
- Central cannabinoid receptors (CB1): analgesia, appetite enhancement, muscle relaxation, hormonal actions
- Indication: refractory N/V with no response to other regiments; stimulate appetite
- Side effects:
- CNS depression (use caution in elderly, frail and those at high risk of fall)
- To minimize ADE, start lower doses (especially in older or marijuana-naïve) and titrate to effect.
- Excessive cannabinoid use can lead to cannabinoid hyperemesis.
- Dronabinol PO solution (Marinol as Rx) has greater PO bioavailability than dronabinol capsules; 2.1 mg PO solution = 2.5 mg capsules.
- Prefer edible preparation
- Smoking can cause aspergillosis, heavy metal toxins
- Vaping: popcorn lungs
- Vaporing (tincture): gives faster effect but not for a long time and less ADE compared to other routes (vaping/smoking)
- Different shops provides different tincture %
- Non-prescription, provider certification, taxed less
| Dronabinol | |
| Dose/Route | Oral (capsule): 5–10 mg/m2 3–4 times daily Oral solution (5mg/mL): 2.1–4.2 mg/m2 3–4 times daily |
| Pearls | Oral solution BA > oral capsules; 2.1 mg solution = 2.5 mg capsules. |
Anticipatory, Anxiety-related, or Breakthrough nausea
- Consider adding lorazepam 0.5–1 mg PO/IV/SL every 6 hours PRN on days 1-4.
- Use the lowest effective dose and interval.
- May be administered with or without H2 blocker or PPI if patient exhibits reflux symptoms
Anticipatory Emesis (PREVENTION IS THE KEY)
- Use optimal antiemetic therapy during every cycle
- Avoid strong smells that may trigger emesis; cognitive distraction
- Consider anxiolytic therapy:
- lorazepam 0.5–2 mg PO beginning on the night before treatment and then repeat next day 1–2h before chemotherapy begins
- Complementary/alternative therapy (Category 2A)
- Behavioral therapy: Relaxation/systematic desensitization, hypnosis, relaxation exercises (guided imagery, progressive muscle relaxation, biofeedback, music therapy)
- Yoga (if proven by physician)
- Acupuncture/acupressure
Breakthrough Emesis
- Add one agent from a different class to the current regimen
- Routine/scheduled/around-the-clock admin should be considered
- Oral route is not feasible if patient is vomiting; consider IV/rectal – neutropenic (ANC<500) avoid rectal meds
- Dopamine antagonists (phenothiazines, olanzapine, metoclopramide, haloperidol), corticosteroids, and agents such as lorazepam may be required.
- Treat any underlying cause and correct any electrolyte imbalance
- Adequate hydration or fluid repletion
- Reassess patients for breakthrough N/V reasons prior to next cycle:
- Brain metastases
- Electrolyte abnormalities
- Tumor infiltration of the bowel or other GI abnormality
- Other comorbidities
- Managements:
- Add an NK1 RA if not previously included.
- Consider changing from NK1-RA–containing regimens to an olanzapine-containing regimen, or vice versa.
- Consider combining an NK1 RA regimen with olanzapine
- Consider changing to a different NK1 RA with different PK/PD profile (No head-to-head clinical trial but anecdotal evidence suggests it may be helpful)
- Add other concomitant antiemetics (metoclopramide or haloperidol), if applicable.
- Possibly adjust dose(s), either intensity or frequency, of the 5-HT3 RA (maybe anticancer therapy regimen is more emetogenic than generally classified)
- Possibly switch to a different 5-HT3 RA (anecdotal and limited investigational trial suggest it may be efficacious)
- 5-HT3 RAs have different PK/PD and different routes of metabolism that may account for different efficacy in certain populations.
- If goal of anticancer therapy is non-curative, consider other appropriate regimens, if any, that might be less emetogenic.
- It may be beneficial to add an anxiolytic agent in combination with the antiemetic agents.
- Consider antacid if dyspepsia (H2RA or PPI)
Drug-drug interactions between antiemetics used in cancer patients Article
Parenteral Emetic Risks
NCCN Guideline. Antiemesis. Version 2.2025. May 12, 2025.
| High emetic risk (>90%) | ||
| • Any AC regimens • Carboplatin AUC ≥4 • Carmustine >250 mg/m2 • Cisplatin • Cyclophosphamide >1500 mg/m2 • Dacarbazine | • Datopotamab deruxtecan-dlnk • Doxorubicin ≥60 mg/m2 • Epirubicin >90 mg/m2 • Fam-trastuzumab deruxtecan-nxki • Ifosfamide ≥2 g/m2/dose | • Mechlorethamine • Melphalan ≥140 mg/m2 • Sacituzumab govitecan-hziy • Streptozocin • Zolbetuximab-clzb |
| Moderate emetic risk (>30%–90%) | ||
| • Aldesleukin >12–15 million IU/m2 or 600,000 IU/kg • Amifostine >300 mg/m2 • Bendamustine • Busulfan • Carboplatin AUC <4 • Carmustine ≤250 mg/m2 • Clofarabine • Cyclophosphamide ≤1500 mg/m2 • Cytarabine >200 mg/m2 | • Dactinomycin • Daunorubicin • Dinutuximab • Doxorubicin <60 mg/m2 • Dual-drug liposomal encapsulation of cytarabine and daunorubicin (Vyxeos; CPX-351) • Epirubicin ≤90 mg/m2 • Idarubicin • Ifosfamide <2 g/m2/dose • Irinotecan | • Irinotecan (liposomal) • Lurbinectedin • Melphalan <140 mg/m2 • Methotrexate ≥250 mg/m2 • Mirvetuximab soravtansine-gynx • Naxitamab-gqgk • Oxaliplatin • Romidepsin • Temozolomide • Trabectedin |
| Low emetic risk (10%–30%) | ||
| • Ado-trastuzumab emtansine • Aldesleukin ≤12 million IU/m2 • Amifostine ≤300 mg/m2 • Amivantamab-vmjw • Arsenic trioxide • Axicabtagene ciloleucel (Yescarta) • Azacitidine • Belinostat • Brentuximab vedotin • Brexucabtagene autoleucel (Tecartus) • Cabazitaxel • Carfilzomib • Ciltacabtagene autoleucel (Carvykti) • Copanlisib • Cytarabine (low dose) 100–200 mg/m2 • Docetaxel • Doxorubicin (liposomal) • Elranatamab-bcmm • Enfortumab vedotin-ejfv | • Epcoritamab-bysp • Eribulin • Etoposide • Floxuridine • 5-Fluorouracil (5-FU) • Gemcitabine • Gemtuzumab ozogamicin • Idecabtagene vicleucel • Inotuzumab ozogamicin • Isatuximab-irfc • Ixabepilone • Lifileucel • Lisocabtagene maraleucel (Breyanzi) • Loncastuximab tesirine-lpyl • Methotrexate >50 – <250 mg/m2 • Mitomycin • Mitomycin pyelocalyceal solution • Mitoxantrone • Mogamulizumab-kpkc | • Mosunetuzumab-axgb • Moxetumomab pasudotox-tdfk (Lumoxiti) • Necitumumab • Omacetaxine • Paclitaxel • Paclitaxel-albumin • Pemetrexed • Pentostatin • Polatuzumab vedotin-piig • Pralatrexate • Tafasitamab-cxix • Tagraxofusp-erzs • Talimogene laherparepvec • Tebentafusp-tebn • Thiotepa • Tisagenlecleucel (Kymriah) • Tisotumab vedotin-tftv (Tivdak) • Topotecan • Ziv-aflibercept |
| Minimal emetic risk (<10%) | ||
| • Alemtuzumab • Asparaginase • Atezolizumab • Atezolizumab and hyaluronidase-tqjs • Avelumab • Betibeglogene autotemcel • Belantamab mafodotin-blmf (Blenrep) • Bevacizumab • Bleomycin • Blinatumomab (Blincyto) • Bortezomib (Velcade) • Cemiplimab-rwlc • Cetuximab • Cladribine • Cytarabine <100 mg/m2 • Daratumumab • Daratumumab and hyaluronidase-fihj • Decitabine • Degarelix • Dexrazoxane • Dostarlimab-gxly • Durvalumab | • Elotuzumab • Fludarabine • Fulvestrant • Glofitamab-gxbm • Goserelin • Histrelin • Imetelstat • Ipilimumab • Lanreotide • Leuprolide • Lovotibeglogene autotemcel (Lyfgenia) • Luspatercept-aamt • Margetuximab-cmkb • Methotrexate ≤50 mg/m2 • Nelarabine • Nivolumab • Nivolumab and hyaluronidase-nvhy • Nivolumab/relatlimab-rmbw • Obinutuzumab • Octreotide • Ofatumumab • Panitumumab • Pembrolizumab • Pertuzumab | • Pertuzumab/trastuzumab and hyaluronidase-zzxf • Ramucirumab • Retifanlimab-dlwr • Rituximab • Rituximab and hyaluronidase • Siltuximab • Sirolimus-albumin • Talquetamab-tgvs • Tarlatamab-dlle • Teclistamab-cqyv • Temsirolimus • Tislelizumab-jsgr • Toripalimab-tpzi • Trastuzumab • Trastuzumab and hyaluronidase-oysk • Tremelimumab-actl • Triptorelin • Valrubicin • Vinblastine • Vincristine • Vincristine (liposomal) • Vinorelbine |
High emetic Risk
| Chemo Day | Option 1 | Option 2 | Option 3 |
|---|---|---|---|
| Day 1 | Olanzapine PO 2.5-10mg + NK1 RA (-pitant) + 5-HT3 RA (-setron) + Dexamethasone PO/IV 12mg | Olanzapine PO 2.5-10mg + Palonosetron IV 0.25mg + Dexamethasone PO/IV 12mg | NK1 RA (-pitant) + 5-HT3 RA (-setron) + Dexamethasone PO/IV 12mg |
| Day 2-4 | Olanzapine PO 2.5-10mg OR Aprepitant PO (if on D1) 80mg D2-3 ± Dexamethasone PO/IV 8mg | Olanzapine PO 2.5-10mg | Aprepitant PO (if on D1) 80mg D2-3 OR Dexamethasone PO/IV 8mg¨ |
Moderate Emetic Risk
| Chemo Day | Option 1 | Option 2 | Option 3 |
|---|---|---|---|
| Day 1 | 5-HT3 RA (-setron) + Dexamethasone PO/IV 12mg | Olanzapine PO 2.5-10mg + Palonosetron IV 0.25mg + Dexamethasone PO/IV 12mg | NK1 RA (-pitant) + 5-HT3 RA (-setron) + Dexamethasone PO/IV 12mg |
| Day 2-3 | Dexamethasone PO/IV 8mg OR 5-HT3 RA (-setron PO) | Olanzapine PO 2.5-10mg | Aprepitant PO (if on D1) 80mg D2-3 ± Dexamethasone PO/IV 8mg/day |
Low Emetic Risk
Dexamethasone, Metoclopramide, Prochlorperazine, or 5-HT3 RA
Minimal Emetic Risk
No routine prophylaxis
Oral Emetic Risks
NCCN Guideline. Antiemesis. Version 2.2025. May 12, 2025.
| Moderate to high emetic risk (≥30%): Prophylaxis required on days of oral anticancer | ||
| • Azacitidine • Busulfan ≥4 mg/day • Ceritinib • Cyclophosphamide ≥100 mg/m2/day | • Fedratinib • Lomustine (single day) • Midostaurin • Mitotane • Mobocertinib | • Selinexor • Temozolomide >75 mg/m2/day • Temozolomide ≤75 mg/m/day with concurrent RT |
| Moderate to high emetic risk (≥30%): PRN dosing is initially appropriate on days of oral anticancer | ||
| • Abemaciclib • Adagrasib • Avapritinib • Binimetinib • Bosutinib >400 mg/day • Cabozantinib • Crizotinib | • Dabrafenib • Elacestrant • Enasidenib • Encorafenib • Estramustine • Etoposide • Imatinib >400 mg/day | • Lenvatinib >12 mg/day • Niraparib • Olaparib • Procarbazine • Rucaparib • Tovorafenib • Trifluridine/tipiracil |
| Minimal to low emetic risk (<30%) | ||
| • Abiraterone • Acalabrutinib • Afatinib • Alectinib • Alpelisib • Anastrozole • Apalutamide • Asciminib • Axitinib • Belzutifan • Bexarotene • Bicalutamide • Bosutinib ≤400 mg/day • Brigatinib • Busulfan <4 mg/day • Capecitabine • Capivasertib • Capmatinib • Chlorambucil • Cobimetinib • Cyclophosphamide <100 mg/m2/day • Dacomitinib • Darolutamide • Dasatinib • Decitabine and Cedazuridine • Duvelisib • Eflornithine • Entrectinib • Enzalutamide • Erdafitinib • Erlotinib • Everolimus • Exemestane • Fludarabine | • Flutamide • Fruquintinib • Futibatinib • Gefitinib • Gilteritinib • Glasdegib • Hydroxyurea • Ibrutinib • Idelalisib • Imatinib ≤400 mg/day • Ivosidenib • Ixazomib • Lapatinib • Larotrectinib • Lenalidomide • Lenvatinib ≤12 mg/day • Letrozole • Lorlatinib • Megestrol • Melphalan • Mercaptopurine • Methotrexate • Momelotinib • Neratinib • Nilotinib • Nilutamide • Nirogacestat • Olutasidenib • Osimertinib • Pacritinib • Palbociclib • Pazopanib • Pemigatinib • Pexidartinib • Pirtobrutinib | • Pomalidomide • Ponatinib • Pralsetinib • Quizartinib • Regorafenib • Relugolix • Repotrectinib • Ribociclib • Ripretinib • Ruxolitinib • Selpercatinib • Sonidegib • Sorafenib • Sotorasib • Sunitinib • Talazoparib tosylate • Tamoxifen • Tazemetostat • Temozolomide ≤75 mg/m2/day • Tepotinib • Thalidomide • Thioguanine • Tivozanib • Topotecan • Toremifene • Trametinib • Tretinoin • Tucatinib • Vandetanib • Vemurafenib • Venetoclax • Vismodegib • Vorinostat • Zanubrutinib |
Moderate-High Emetic Risk (prophylaxis required): 5-HT3 RA or Olanzapine
Minimal-low Emetic Risk (PRN recommended): Metoclopramide, Prochlorperazine, or 5-HT3 RA
Dosing:
- Olanzapine 2.5-10mg/day PO
- NK1 RA
- Aprepitant 125 mg PO, Aprepitant 130 mg IV
- Fosaprepitant 150 mg IV
- Netupitant/palonosetron 300mg/0.5mg PO
- Fosnetupitant/palonosetron 235mg/0.25mg IV
- Rolapitant 180 mg PO
- 5-HT3 RA
- Dolasetron 100 mg PO
- Granisetron 10 mg SC or 2 mg PO or 0.01 mg/kg (max 1 mg) IV or 3.1 mg transdermal patch applied 24–48 h prior to first dose of anticancer therapy
- Ondansetron 16–24 mg PO or 8–16 mg IV once
- Palonosetron 0.25 mg IV
- Dexamethasone 12mg PO/IV (on D2-4: 8mg/day PO/IV)