NCCN Guidelines Version 1.2026 for CML | Updated: July 16, 2025
For clinical and educational use only. Always verify with current guidelines and institutional protocols.
Epidemiology
- 15% of adult leukemias ~9,560 new cases/yr (2025)
- Median age: 67 years All age groups affected
- Ph+ [t(9;22)] ALL phases BCR::ABL1 driven
- TKI therapy cornerstone treatment-free remission (TFR) goal in select pts
SECTION 1: OVERVIEW, PATHOPHYSIOLOGY & MOLECULAR BIOLOGY
Disease Definition
CML is a myeloproliferative neoplasm (MPN) defined by the presence of the
Philadelphia chromosome (Ph) resulting from a reciprocal translocation t(9;22)(q34;q11)
creating the BCR::ABL1 fusion oncogene.
BCR::ABL1 encodes a constitutively active tyrosine kinase (p210) that drives uncontrolled myeloid proliferation and impairs apoptosis.
BCR::ABL1 Transcript Variants (NCCN v1.2026)
| Transcript | Protein | Frequency | Clinical Notes |
|---|---|---|---|
| e14a2 (b3a2) | p210 | ~62% (most common) | Higher molecular response to imatinib; better DMR rates |
| e13a2 (b2a2) | p210 | ~39% | More frequent in males; may have inferior nilotinib response vs. dasatinib |
| e1a2 | p190 | Uncommon (~1-2%) | Higher progression risk, inferior CyR/MR to TKIs, inferior survival — referral to CML center recommended |
| e19a2 | p230 | Rare (~1%) | Lower CyR/MR to TKIs, inferior survival despite historically indolent course |
| b2(e13)a3, b3(e14)a3 | Atypical | ~1-2% | ASCIMINIB CONTRAINDICATED — lacks ABL1 exon 2, no clinical activity. Also incompatible with standard IS qPCR monitoring. |
PHARMACIST PEARL: BCR::ABL1 Transcript Type Matters at Treatment Selection
– ALWAYS verify transcript type before initiating asciminib—b2(e13)a3 and b3(e14)a3 are absolute contraindications (NCCN v1.2026, footnote g)
– Transcript type is now a required treatment consideration per NCCN v1.2026 (CML-2 new bullet #1)
– Standard IS qPCR assays are calibrated for e13a2 and e14a2 transcripts — atypical transcripts cannot be monitored with standard IS qPCR; use qualitative RT-PCR or nested PCR instead
– Note: e14a2 associated with better molecular response — may influence TFR eligibility discussions
Disease Phases Overview
| Phase | Key Features | Natural History |
|---|---|---|
| Chronic Phase (CP) | WBC elevation, splenomegaly; <15% blasts; minimal symptoms | ~85-90% present here. Most responsive to TKI therapy. Median survival near-normal with optimal TKI response. |
| Accelerated Phase (AP) | Per MDACC criteria: 15-29% PB blasts; blasts+promyelocytes ≥30%; basophils ≥20%; plt <100 x10⁹/L (unrelated to tx); new ACAs in Ph+ cells | Disease progression; worse prognosis than CP. Can occur de novo or progress from CP. TKI therapy followed by evaluation for allogeneic HCT. |
| Blast Phase (BP) | IBMTR: ≥30% myeloblasts in PB/BM or extramedullary disease. Lymphoid BP: ANY increase in lymphoblasts in PB or BM | Transformation to acute leukemia. Myeloid or lymphoid. Allo-HCT goal after achieving remission. CNS prophylaxis for lymphoid BP. |
CRITICAL: IMPORTANT: Diagnostic Criteria Clarification
– NCCN v1.2026 recommends AGAINST using ICC or WHO 2022 criteria for AP/BP-CML diagnosis — use modified MDACC or IBMTR criteria (these are used in TKI clinical trials)
– Lymphoid BP-CML: ANY increase in lymphoblasts in PB or BM qualifies — this was updated in v1.2026 (previously ‘increase concerning for nascent blast phase’)
– AP defined by clonal cytogenetic evolution ALONE on imatinib has better prognosis than AP with additional features
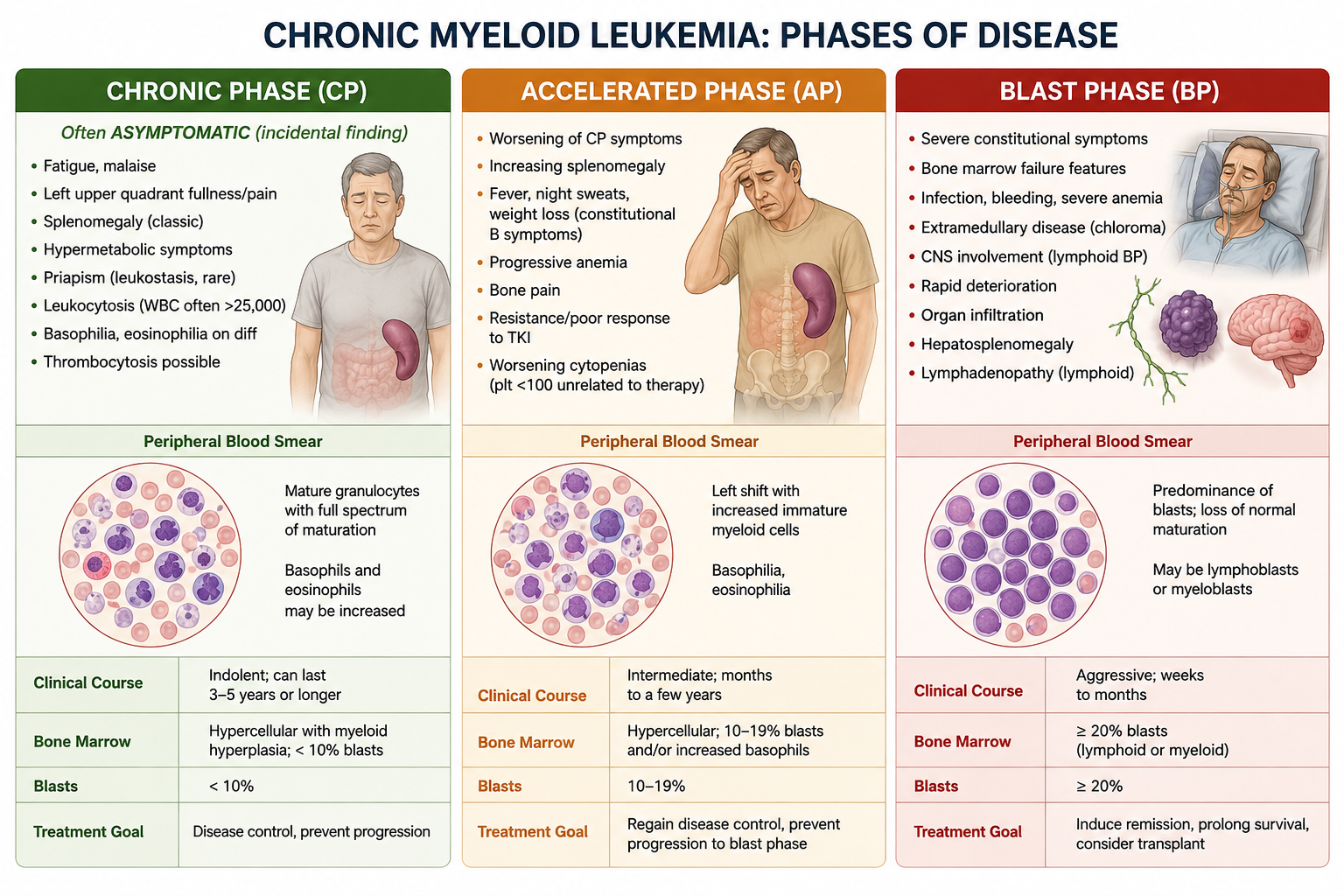
Signs & Symptoms by Phase
| Chronic Phase (CP) | Accelerated Phase (AP) | Blast Phase (BP) |
|---|---|---|
| Often ASYMPTOMATIC (incidental finding) – Fatigue, malaise – Left upper quadrant fullness/pain – Splenomegaly (classic) – Hypermetabolic symptoms – Priapism (leukostasis, rare) – Leukocytosis (WBC often >25,000) – Basophilia, eosinophilia on diff – Thrombocytosis possible | – Worsening of CP symptoms – Increasing splenomegaly – Fever, night sweats, weight loss (constitutional B symptoms) – Progressive anemia – Bone pain – Resistance/poor response to TKI – Worsening cytopenias (plt <100 unrelated to therapy) | – Severe constitutional symptoms – Bone marrow failure features – Infection, bleeding, severe anemia – Extramedullary disease (chloroma) – CNS involvement (lymphoid BP) – Rapid deterioration – Organ infiltration – Hepatosplenomegaly – Lymphadenopathy (lymphoid) |
Differential Diagnosis of CML
- Leukemoid reaction (reactive leukocytosis): BCR::ABL1 negative; usually due to infection/inflammation; LAP score HIGH (vs. low in CML)
- Chronic myelomonocytic leukemia (CMML): BCR::ABL1 negative; monocytosis >1×10⁹/L; mutations in ASXL1, TET2, SRSF2
- Other MPNs (PV, ET, PMF): BCR::ABL1 negative; evaluate per NCCN MPN Guidelines
- Juvenile myelomonocytic leukemia (JMML): Pediatric; BCR::ABL1 negative; RAS pathway mutations
- Ph+ ALL: BCR::ABL1 positive but p190 dominant; ALL immunophenotype on flow; differentiate with interphase FISH on blood granulocytes
SECTION 2: DIAGNOSIS & WORKUP (NCCN CML-1)
Required Initial Workup
| Test | Clinical Notes / Pharmacist Relevance |
|---|---|
| H&P incl. spleen size (cm below costal margin) | Spleen size used in all 3 risk scores (Sokal, Hasford, ELTS) — document accurately |
| CBC with differential | Leukocytosis hallmark; basophilia >20% = AP criteria; thrombocytosis common; anemia in advanced phase. Baseline needed for response monitoring. |
| Chemistry profile (incl. uric acid, LFTs, creatinine) | LFTs at baseline essential — multiple TKIs are hepatotoxic; uric acid for tumor lysis risk assessment; renal function for dose adjustment guidance |
| Bone marrow aspirate + biopsy | Minimum 20 metaphases for cytogenetics. Morphology for blast %. FISH if standard cytogenetics not feasible (minimum 100 interphase nuclei). |
| Bone marrow cytogenetics | Detects Ph chromosome + additional chromosomal abnormalities (ACAs); major route ACAs (trisomy 8, iso17q, 2nd Ph, trisomy 19, chr3 abnl) = negative prognostic impact |
| qPCR (IS) for BCR::ABL1 — peripheral blood | ESSENTIAL BASELINE — establishes quantifiable transcript level for monitoring. Must use International Scale (IS). Detects 1 CML cell per >100,000 normal cells. |
| Hepatitis B panel (HBsAg, anti-HBc, anti-HBs) | HBV reactivation reported with TKI therapy. Screen before initiation. Prophylaxis with entecavir/tenofovir if HBsAg+ or anti-HBc+ (check institutional policy). |
| Assess for distress (NEW v1.2026) | NCCN Distress Thermometer; includes social determinants of health. See NCCN Distress Management Guidelines (DIS-A). |
| ECG / QTc | Not mandated at initial workup but CRITICAL before initiating nilotinib or any QT-prolonging TKI. Must correct K+/Mg2+ before starting therapy. |
Advanced Phase Additional Workup (CML-1, NCCN)
- Flow cytometry to determine cell lineage (myeloid vs. lymphoid BP — critical for treatment selection)
- Consider myeloid mutational analysis (category 2B) — ASXL1, IKZF1, RUNX1, BCOR, TET1/2, IDH1/2, DNMT3A/3B, EZH2
- HLA testing if considering allogeneic HCT
- Lumbar puncture + CNS prophylaxis for LYMPHOID BP-CML (CNS involvement described)
- Interphase FISH on blood granulocytes to differentiate de novo BP-CML vs. de novo Ph+ ALL
PHARMACIST WATCHOUT: Baseline Labs Before TKI Initiation
– QTc: baseline ECG MANDATORY for nilotinib (QTc >480ms = contraindication); document and trend
– Electrolytes: correct K⁺ and Mg²⁺ BEFORE initiating any TKI (low levels increase QT risk)
– LFTs: bosutinib, nilotinib, and ponatinib most hepatotoxic; hold TKI for Grade 3+ LFT elevation
– Lipase/amylase baseline: nilotinib, ponatinib, asciminib cause pancreatitis — document baseline
– Glucose: nilotinib causes hyperglycemia — baseline glucose/HbA1c
– Hepatitis B: do NOT start TKI without HBV screening result — reactivation is a black-box risk
– Phosphate/calcium/vitamin D: check before initiating — correct deficiencies (especially for nilotinib-associated hypophosphatemia)
SECTION 3: RISK STRATIFICATION — PROGNOSTIC SCORES (NCCN CML-A)
Three validated scoring systems are used for CP-CML risk stratification prior to TKI initiation. Online calculators available at: https://www.leukemia-net.org
| Score | Formula Variables | Low Risk | Intermediate | High Risk |
|---|---|---|---|---|
| SOKAL | Age, spleen size (cm below costal margin), platelet count, % blasts in PB | < 0.8 | 0.8 – 1.2 | > 1.2 |
| HASFORD (EURO) | Age, spleen, % blasts, % eosinophils, basophils, platelet count | ≤780 | >780 – ≤1480 | >1480 |
| ELTS | Age, spleen, % PB blasts, platelet count (same as Sokal variables) | ≤1.5680 | >1.5680 – ≤2.2185 | >2.2185 |
Which Score to Use? Clinical Pearl (NCCN)
- ELTS score is preferred as it specifically predicts CML-RELATED death (not competing/non-CML mortality) — most relevant in TKI era where patients die of non-CML causes
- ELTS validated in 1,120 CP-CML patients treated with imatinib across 6 clinical trials
- Sokal/Hasford used in most clinical trials (BFORE, DASISION, ENESTnd, ASC4FIRST) — check which score applies to trial data you are referencing
- All three scores use the same variables (except Hasford adds eosinophils and basophils)
- Risk score impacts FIRST-LINE TKI selection: intermediate/high risk = prefer 2G TKI or asciminib over imatinib
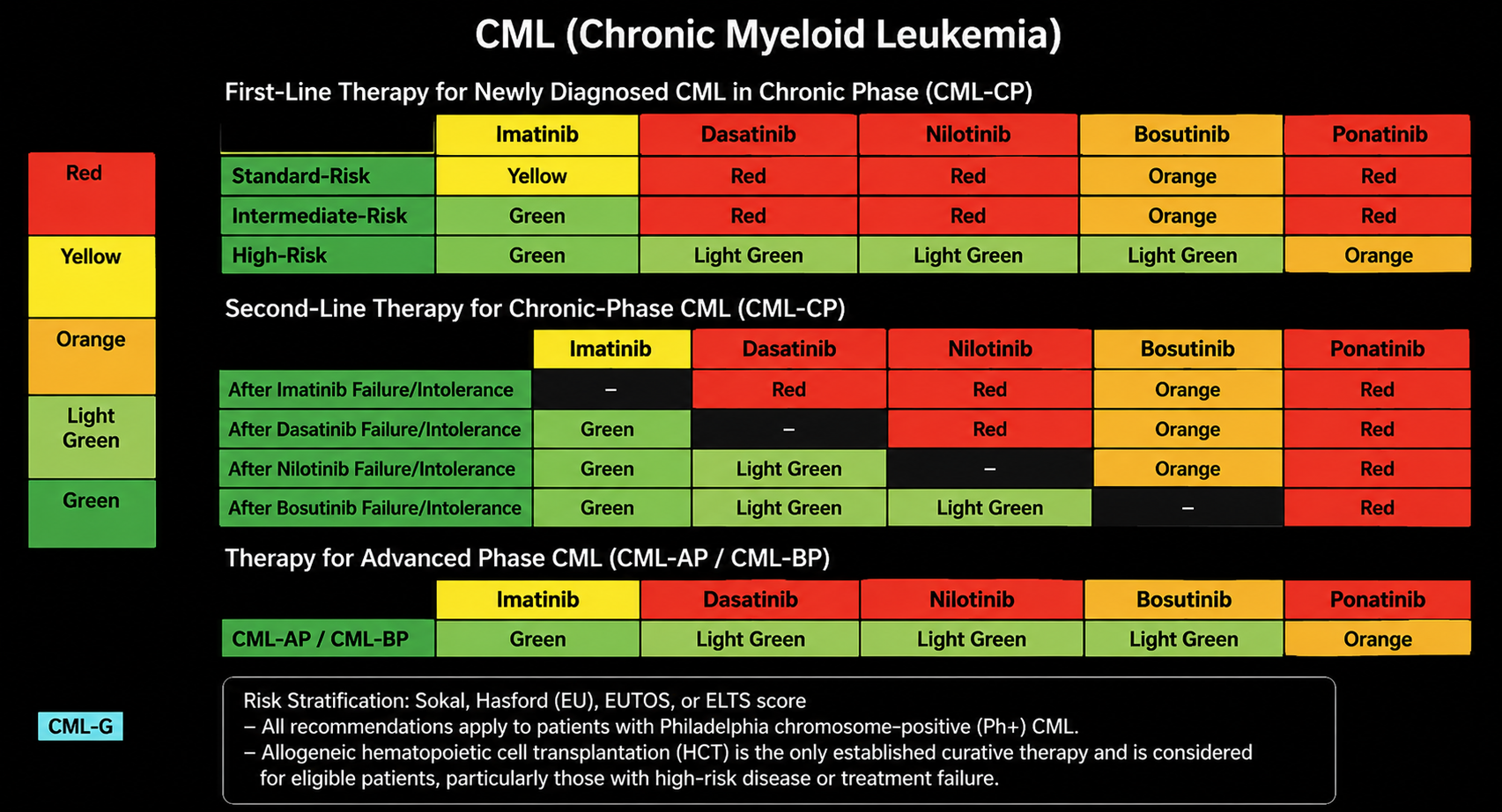
Risk Score and Treatment Selection (NCCN CML-2)
| Risk Category | NCCN Preferred Treatment (1st Line) |
|---|---|
| LOW RISK | Preferred: 1G TKI (Imatinib [Cat 1]) OR 2G TKI (Bosutinib, Dasatinib, or Nilotinib [Cat 1]) OR Allosteric TKI (Asciminib [Cat 1]) | Also: Clinical trial |
| INTERMEDIATE / HIGH RISK | PREFERRED: 2G TKI (Bosutinib, Dasatinib, OR Nilotinib [Cat 1]) OR Allosteric TKI (Asciminib [Cat 1]) | Other recommended: 1G TKI (Imatinib) — use if older age + CV comorbidities | Also: Clinical trial |
Treatment considerations INDEPENDENT of risk score (NCCN CML-2, updated v1.2026):
- BCR::ABL1 transcript type (NEW v1.2026 — check for asciminib contraindication)
- Age and comorbidities
- Toxicity profile of TKI (see CML-C section)
- TKI dosing schedule (NEW v1.2026 — once vs. twice daily; food interaction requirements)
- Possible drug interactions (see Drug Interactions section)
- Treatment goal: long-term survival vs. treatment-free remission (TFR)
- Medication cost (NEW v1.2026 — generics available for imatinib, dasatinib, nilotinib; substantially less costly)
- Patient preference
SECTION 4: TREATMENT — CHRONIC PHASE CML (NCCN CML-2/3)
TKI Dosing Reference Table — CP-CML
| Agent | Standard Dose | Administration | CP-CML Approved Dose | AP/BP-CML Dose | Generation |
|---|---|---|---|---|---|
| Imatinib (Gleevec/generic) | 400 mg PO QD | With food & large glass of water | 400 mg QD (CP) 600 mg QD (suboptimal) | 600 mg QD | 1G TKI |
| Dasatinib (Sprycel/generic) | 100 mg PO QD | With OR without food; NO food restrictions (standard formulation requires acid-independent absorption note) | 100 mg QD (CP) | 140 mg QD | 2G TKI |
| Nilotinib (Tasigna) | 300 mg PO BID | FASTING: 2 hrs BEFORE + 1 hr AFTER dose (NO food). Capsule formulation — no substitution with tablets! | 300 mg BID (CP, newly diag.) 400 mg BID (resistant/intolerant) | 400 mg BID (AP) | 2G TKI |
| Bosutinib (Bosulif) | 400 mg PO QD (1st line) 500 mg QD (2nd+ line) | WITH FOOD (take with food or GI upset significantly worsened) | 400 mg QD (1st line) | 500 mg QD (AP/BP) | 2G TKI |
| Ponatinib (Iclusig) | 45 mg PO QD initially; REDUCE to 15 mg QD if CCyR achieved (CV risk reduction) | With OR without food | 45 mg QD → reduce on response; CP with ≥2 prior TKIs or T315I | 45 mg QD (AP/BP, preferred with T315I) | 3G TKI (CV risk) |
| Asciminib (Scemblix) | 40 mg PO BID (non-T315I) 200 mg PO BID (T315I) | FASTING: take on empty stomach; do NOT eat for at least 2 hrs before and 1 hr after | 40 mg BID (1st line newly diag. — Cat 1; also 2nd+ line) 200 mg BID (T315I) | 40 mg BID (AP); 200 mg BID (T315I AP) | Allosteric TKI (STAMP inhibitor — myristoyl pocket) |
CRITICAL: CRITICAL PHARMACIST WATCHOUTS — TKI Administration & Formulation
– NILOTINIB: MUST be taken on EMPTY STOMACH — food increases absorption unpredictably and can raise drug levels → QT prolongation risk. CRITICAL counseling point.
– ASCIMINIB: MUST be taken on EMPTY STOMACH — food increases exposure. Different dosing for T315I mutation (200 mg BID vs. 40 mg BID standard).
– BOSUTINIB: MUST be taken WITH FOOD — GI tolerability (diarrhea/nausea) significantly worsened when taken fasted
– NILOTINIB formulations are NOT interchangeable: capsule vs. tablet formulations have different administration requirements and bioavailability profiles
– DASATINIB: pH-independent formulation (new FDA-approved option) allows concomitant use with PPIs/H2RAs — confirm which formulation patient has before counseling on acid suppression
– IMATINIB preferred in older patients with cardiovascular comorbidities (nilotinib/ponatinib avoid in CV disease)
– PONATINIB: ALWAYS document indication for use — required for 2+ prior TKI failures OR T315I mutation (NOT a first-line agent); start at 45 mg, reduce to 15 mg once CCyR achieved to minimize CV risk
– GENERICS (imatinib, dasatinib, nilotinib): FDA-approved generics are appropriate substitutes per NCCN v1.2026. Monitor closely during transitions — narrow therapeutic window (esp. nilotinib, bosutinib)
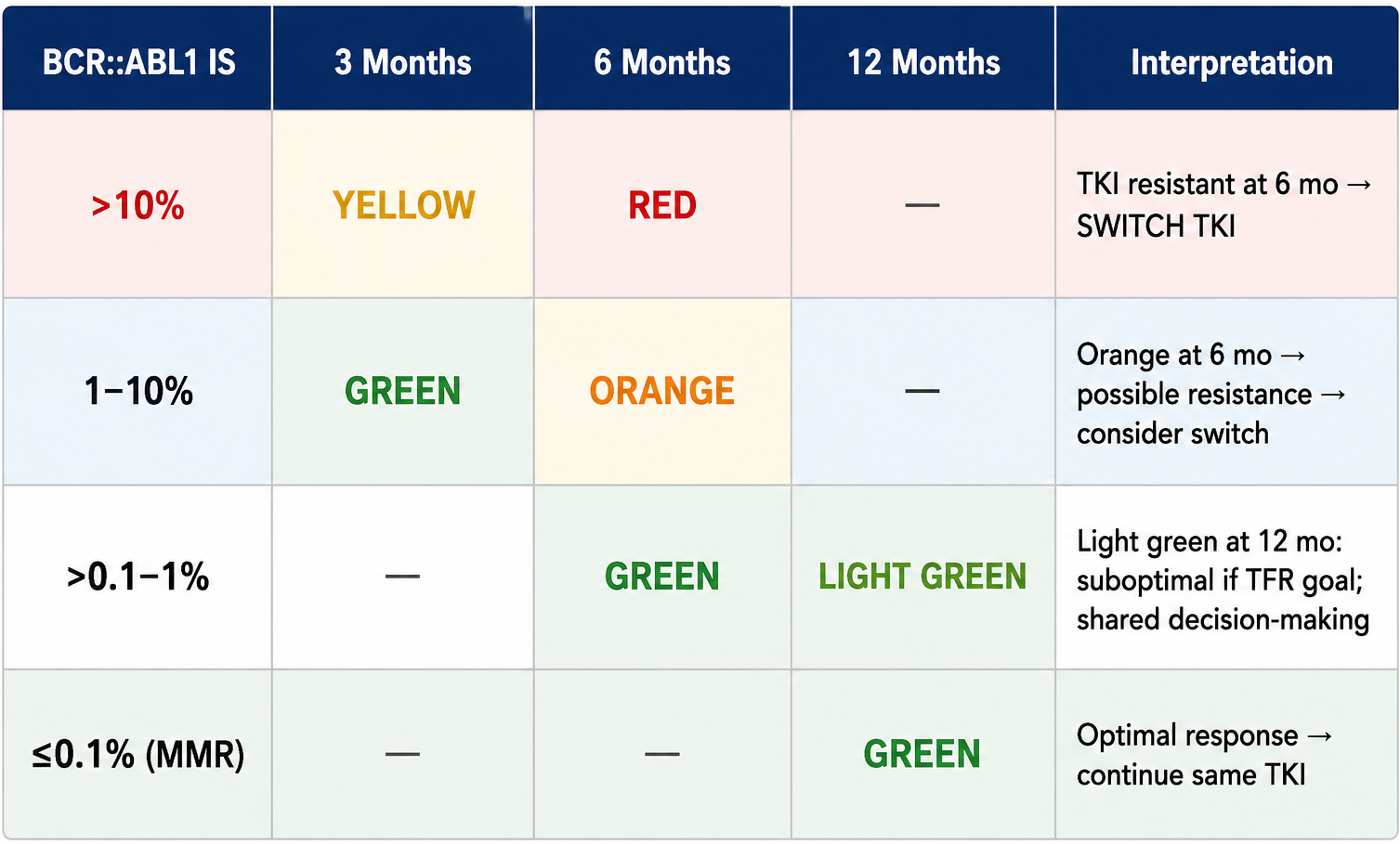
Response Milestones & Color-Coded Decision Tool (NCCN CML-3)
BCR::ABL1 (IS) thresholds at key time points guide treatment decisions:
Context-Sensitive Interpretation of 3-Month BCR::ABL1 Value
- BCR::ABL1 slightly >10% at 3 months: do NOT automatically switch if steep decline from baseline or close to 10% — continue TKI for another 3 months and recheck
- Imatinib is associated with SLOWER molecular responses than 2G TKIs — factor this in before switching from imatinib at 3 months
- A 1-log decrease from baseline is generally reassuring even if still above 10% at 3 months
- Patient adherence and drug interactions MUST be evaluated BEFORE declaring TKI resistance
Response Definitions (NCCN CML-F)
| Response Category | Definition |
|---|---|
| Complete Hematologic Response (CHR) | WBC <10 x10⁹/L; Platelets <450 x10⁹/L; No immature cells (myelocytes, promyelocytes, blasts) in PB; Resolution of splenomegaly |
| Complete Cytogenetic Response (CCyR) | 0% Ph-positive metaphases. Correlates with BCR::ABL1 IS ≤1% (MR2.0) |
| Major Cytogenetic Response (MCyR) | 0–35% Ph+ metaphases |
| Early Molecular Response (EMR) | BCR::ABL1 IS ≤10% at 3 AND 6 months |
| Major Molecular Response (MMR / MR3.0) | BCR::ABL1 IS ≤0.1% OR ≥3-log reduction from standardized baseline (if IS not available) |
| Deep Molecular Response MR4.0 | BCR::ABL1 IS ≤0.01% |
| Deep Molecular Response MR4.5 | BCR::ABL1 IS ≤0.0032% — required for TFR eligibility (more sensitive than MR4.0) |
| Relapse | Loss of hematologic response; loss of CCyR or MR2.0 (BCR::ABL1 >1%); 1-log increase with loss of MMR |
SECTION 5: MONITORING SCHEDULE (NCCN CML-G)
| Test | Frequency & Trigger |
|---|---|
| CBC with differential | Every 1–2 weeks for first 1–2 months (or until stable blood count normalization), then as indicated based on persistence of cytopenias |
| Bone marrow cytogenetics | At diagnosis; when response milestones not reached; at any sign of loss of hematologic response; loss of CCyR/MR2.0 (BCR::ABL1 >1%) |
| qPCR (IS) — peripheral blood | At diagnosis; EVERY 3 MONTHS after initiating TKI. After BCR::ABL1 IS ≤1% (MR2.0) achieved: every 3 months x 2 years, then every 3–6 months indefinitely. If 1-log increase + MMR: repeat in 1–3 months |
| BCR::ABL1 kinase domain mutation analysis | When response milestones not reached; loss of hematologic response; loss of CCyR or MR2.0 (BCR::ABL1 >1%); 1-log increase + loss of MMR; progression to AP/BP-CML. Consider myeloid mutation panel if NO BCR::ABL1 mutations found (independent resistance mutations) |
| LFTs, chemistries | Per package insert for each TKI; more frequent for hepatotoxic agents (bosutinib, imatinib). Hold for Grade 3+ elevation. |
| Lipase/amylase | Monitor in patients on nilotinib, ponatinib, asciminib — highest pancreatitis risk. Patients should report abdominal pain promptly (NEW monitoring language v1.2026). |
| ECG / QTc | Baseline, 7 days after TKI initiation, and periodically thereafter; after dose modifications. Mandatory for nilotinib — correct electrolytes first. |
| Blood glucose | Before initiating TKI and periodically during treatment — especially nilotinib (hyperglycemia most common with nilotinib). Refer to PCP/endocrinology. |
| Bone mineral density | Baseline; check vitamin D before and periodically. Lifestyle modifications; no specific TKI intervention established. |
| Post-HCT: qPCR q3mo x2y, then q6mo | Post-allogeneic HCT monitoring: every 3 months x 2 years, then every 6 months. Triggers for mutation analysis and DLI consideration. |
MONITORING PEARLS FOR PHARMACIST ROUNDS
– The MOST sensitive qPCR assay must have sensitivity of at least MR4.5 (BCR::ABL1 ≤0.0032% IS) — critical for TFR eligibility assessment
– qPCR results must be on International Scale (IS) — results from different labs are NOT comparable without IS conversion factor
– If MR2.0 not achieved: ALWAYS check adherence and drug interactions BEFORE declaring resistance
– Bone marrow cytogenetics needed at milestone failures (NOT just qPCR) — need to rule out ACAs in Ph+ cells
– Post-HCT patients: if qPCR positive → discuss TKI options, DLI, or clinical trial with transplant team; consider TKI for ≥1 year in prior AP/BP-CML patients regardless of qPCR
SECTION 6: ADVANCED PHASE CML — AP-CML & BP-CML (NCCN CML-4)
AP-CML Treatment
- TKI dose for AP-CML may DIFFER from CP-CML dose (use AP-CML approved dose)
- Preferred: 2G TKI (Bosutinib, Dasatinib, or Nilotinib) OR 3G TKI (Ponatinib)
- Other recommended: Imatinib (ONLY if 2G/3G TKI contraindicated; NOT if progressed on prior TKI)
- Allosteric TKI (Asciminib): useful in certain circumstances for AP-CML with T315I and/or previously treated AP-CML
- ALL patients with AP-CML: evaluate for allogeneic HCT based on response
- De novo AP-CML at presentation: treat with TKI at FDA-approved AP-CML dose, then evaluate for HCT based on response milestones at 3, 6, and 12 months
- Disease progression to AP-CML during TKI therapy: WORSE prognosis than de novo AP-CML
BP-CML Treatment
| BP-CML Type | Treatment (NCCN CML-4) |
|---|---|
| LYMPHOID BP-CML | Preferred: ALL-type induction chemotherapy (per NCCN ALL guidelines) + TKI. Useful in certain circumstances: TKI + steroids (if not candidate for induction chemo). Remission → Allogeneic HCT; or consolidation chemo + TKI maintenance (if not HCT candidate). CNS prophylaxis REQUIRED. |
| MYELOID BP-CML | Preferred: AML-type induction chemotherapy (per NCCN AML guidelines) + TKI. Useful in certain circumstances: TKI alone (if not candidate for induction chemo). Remission → Allogeneic HCT. |
- TKI selection in BP-CML: based on PRIOR therapy and BCR::ABL1 mutation/variant profile
- Preferred TKI in AP/BP: 2G or 3G TKI (imatinib NOT recommended if progressed on prior TKI therapy)
- Ponatinib preferred for T315I in any phase, or any AP/BP when no other TKI indicated
CRITICAL: CNS INVOLVEMENT IN BP-CML — Pharmacist Action Items
– CNS involvement has been described in BP-CML — especially lymphoid BP
– Lumbar puncture + CNS prophylaxis RECOMMENDED for lymphoid BP-CML (NCCN CML-4)
– Dasatinib has the best CNS penetration among approved TKIs — may be preferred in lymphoid BP with CNS disease (not a formal NCCN recommendation but evidence-based clinical practice)
– Intrathecal chemotherapy per ALL guidelines used for CNS prophylaxis/treatment in lymphoid BP
SECTION 7: BCR::ABL1 MUTATION PROFILE & TKI SELECTION (NCCN CML-5)
BCR::ABL1 kinase domain mutation analysis guides TKI selection after resistance or suboptimal response.
| TKI | Contraindicated Mutations/Variants (NCCN CML-5 v1.2026) |
|---|---|
| Asciminib | A337T, P465S, M244V, F359V/I/C; also b2(e13)a3, b3(e14)a3 transcript variants (NEW v1.2026) |
| Bosutinib | T315I, V299L, G250E, F317L (minimal activity vs. F317L — nilotinib preferred over bosutinib for F317L) |
| Dasatinib | T315I/A, F317L/V/I/C, V299L |
| Nilotinib | T315I, Y253H, E255K/V, F359V/C/I |
| Ponatinib | NONE (no contraindicated mutations) — only TKI active against T315I; compound mutations that can cause ponatinib resistance are UNCOMMON after bosutinib/dasatinib/nilotinib |
| Imatinib | Multiple mutations (too numerous to list); BCR::ABL35INS reported — limited data for 2G TKIs to overcome this resistance |
Sequencing & Decision Logic for Resistant/Intolerant CML
- After imatinib resistance: switch to alternate TKI (check mutation profile) — any 2G TKI, allosteric TKI, or 3G TKI based on mutation
- After asciminib/bosutinib/dasatinib/nilotinib resistance: switch to alternate (NOT imatinib); ponatinib PREFERRED if no identifiable BCR::ABL1 mutation
- T315I mutation (the ‘gatekeeper’ mutation): ONLY ponatinib (any phase — preferred for AP/BP) or asciminib 200 mg BID are active
- Compound mutations (≥2 mutations on same BCR::ABL1 allele): can cause ponatinib resistance — uncommon after 2G TKIs
- No BCR::ABL1 mutation found + resistance: consider myeloid mutation panel (ASXL1, RUNX1, IKZF1, etc.) for independent resistance mechanisms
KEY CLINICAL PEARL
– The T315I Mutation T315I = ‘gatekeeper mutation’ = MOST CLINICALLY IMPORTANT mutation in CML practice
– Confers resistance to ALL 1G and 2G TKIs (imatinib, dasatinib, nilotinib, bosutinib)
– Active agents: Ponatinib (3G) OR Asciminib 200 mg BID (allosteric, myristoyl pocket binding — different mechanism than ABL1 kinase domain inhibitors)
– Asciminib 200 mg BID (double the standard dose) is used specifically for T315I — verify dose on ANY asciminib order
– Ponatinib dose-reduction strategy: reduce to 15 mg QD once CCyR achieved to minimize arterial/CV events
– Select mutations may be MORE sensitive to certain TKIs based on IC50 values — consult mutation-specific TKI sensitivity tables for precision selection
SECTION 8: ALLOGENEIC HCT — INDICATIONS & POST-HCT MANAGEMENT (NCCN CML-6)
Indications for Allogeneic HCT (NCCN CML-6 v1.2026)
- CP-CML with resistance AND/OR intolerance to ALL available TKIs
- Advanced phase CML at presentation OR disease progression to BP-CML
- Disease progression to AP-CML DURING TKI therapy
- BP-CML in patients who achieve morphologic remission
Outcomes of allogeneic HCT are dependent on: age, comorbidities, donor type, pretransplant disease status, and transplant center.
Post-HCT Management
- Monitor qPCR (peripheral blood) every 3 months x 2 years, then every 6 months thereafter
- If qPCR NEGATIVE: continue monitoring as above
- If qPCR POSITIVE: discuss options with transplant team: TKI therapy, donor lymphocyte infusion (DLI), or clinical trial
- Consider TKI therapy for at least 1 YEAR in patients with PRIOR AP-CML or BP-CML
- TKI selection post-HCT: based on prior therapy, BCR::ABL1 mutation/variant profile, AND post-HCT morbidities
SECTION 9: TKI DISCONTINUATION — TREATMENT-FREE REMISSION (NCCN CML-H)
Criteria for TKI Discontinuation (ALL criteria must be met)
- CP-CML only — NO prior history of AP-CML or BP-CML
- On approved TKI therapy for at least 3 YEARS (age ≥18 years requirement was REMOVED in v1.2026)
- Prior evidence of quantifiable BCR::ABL1 transcript at baseline
- Stable molecular response MR4.0 (BCR::ABL1 ≤0.01% IS) for ≥2 years — documented on at LEAST 4 tests at least 3 months apart
- Access to reliable qPCR with sensitivity of at LEAST MR4.5 (BCR::ABL1 ≤0.0032% IS); results within 2 weeks
Post-Discontinuation Monitoring
- Every 1–2 months for first 6 months post-discontinuation
- Bimonthly (every 2 months) during months 7–12
- Quarterly INDEFINITELY thereafter for patients who remain in MMR
- If loss of MMR: RESTART TKI within 4 weeks; monthly monitoring until MMR re-established, then every 3 months indefinitely
- If MMR not regained after 3 months of TKI resumption: BCR::ABL1 kinase domain mutation testing; continue monthly monitoring for another 6 months
TFR Clinical Pearls for Pharmacist Counseling TKI WITHDRAWAL SYNDROME: musculoskeletal pain, arthralgias, myalgias in ~20-30% of patients — onset weeks to months post-discontinuation. Counsel all patients BEFORE discontinuation.TFR feasibility after TKIs OTHER than dasatinib/imatinib/nilotinib not evaluated in formal clinical studies — extrapolation assumed; consult CML specialistEURO-SKI study: MR4.0 for ≥3 years was most significant predictor of successful discontinuation from imatinib; total imatinib duration ≥6 years also predictiveFactors AGAINST successful TFR: high Sokal risk score, female gender, lower NK cell counts, prior suboptimal response or resistance to imatinib, shorter TKI durationPatient MUST consent after thorough discussion of risks/benefits of TFR attemptConsult NCCN Panel member or CML center of expertise for: significant adverse events related to discontinuation, progression to AP/BP at any time, failure to regain MMR after 3 months
SECTION 10: ADVERSE EVENT MANAGEMENT & SUPPORTIVE CARE (NCCN CML-C)
Switch TKI — Trigger Events (NCCN CML-C)
Consider switching to alternate TKI for the following non-hematologic adverse events:
- Arterial and vascular adverse events — more common with nilotinib and ponatinib
- Severe hypertension NOT responsive to antihypertensives — ponatinib and asciminib
- Pulmonary hypertension — dasatinib
- Recurrent pleural or pericardial effusions despite dose reduction — dasatinib (less common with bosutinib)
- Recurrent pancreatitis despite dose reduction — most common with nilotinib, ponatinib, asciminib
- Hyperglycemia — most common with nilotinib
- Persistent moderate to severe nephrotoxicity — all TKIs
- LFT abnormalities — more common with bosutinib and imatinib
- GI bleeding — dasatinib
- Immune-mediated adverse events (colitis, pneumonitis, hepatitis, myocarditis, pericarditis, nephritis) — all TKIs
- Neurotoxicity — rarely imatinib and dasatinib; dementia-like, parkinsonism, intracranial hypertension
Adverse Event Management Table (NCCN CML-C Table 1)
| Adverse Events | Most Common TKI(s) | Supportive Care | TKI Action |
|---|---|---|---|
| Cardiovascular / Vascular | Nilotinib, Ponatinib | Risk factor control (DM, HTN, HLD, smoking, estrogen); identify drug interactions with CV meds; cardiology referral for CV risk factors | HOLD TKI; SWITCH for new arterial/vascular events when possible |
| QT Prolongation | Nilotinib (most common) | Monitor K+/Mg2+; correct deficiencies BEFORE and DURING TKI; AVOID concomitant QT-prolonging drugs; ECG at baseline, 7 days, and after dose changes | SWITCH if persistent symptoms despite adequate supportive care |
| Hypertension | Ponatinib, Asciminib | Antihypertensives; cardiology referral; BP monitoring | SWITCH if severe HTN not responsive to antihypertensives (ponatinib/asciminib) |
| Pulm. Arterial HTN (PAH) | Dasatinib | HOLD TKI; consider oral corticosteroids and/or sildenafil; cardiology/pulmonary vascular specialist referral | SWITCH (dasatinib-specific; irreversible PAH possible with prolonged exposure) |
| Pleural/Pericardial Effusion | Dasatinib (most common) | HOLD TKI; diuretics and/or oral corticosteroids; echocardiogram for LVEF assessment; dose reduction with close monitoring if not controlled | SWITCH if persistent despite dose reduction; bosutinib less common |
| Pancreatitis | Nilotinib, Ponatinib, Asciminib | HOLD TKI; check amylase/lipase; CT/MRI if indicated; patients must report abdominal pain | SWITCH if recurrent pancreatitis despite dose reduction |
| Hyperglycemia | Nilotinib (most common) | Monitor glucose before initiating and periodically; PCP/endocrinology referral | Monitor; consider switch if severe/uncontrolled |
| GI: Diarrhea / N&V | Bosutinib, Imatinib | Take with food (except nilotinib capsules and asciminib); anti-diarrheals; NCCN antiemesis guidelines; hydration | Dose reduction if not controlled; switch if persistent |
| Hepatotoxicity / LFTs | Bosutinib, Imatinib | Limit alcohol; monitor LFTs; identify drug interactions; HOLD TKI for Grade 3 LFTs; monitor and resume when returns to ≤Grade 1 | Resume at same or reduced dose; switch if recurrent Grade 3+ |
| Dermatologic: Rash | All TKIs (imatinib common) | Moisturizers, antihistamines, topical steroids; dermatology referral for severe rash; avoid tight clothing/hot baths | Dose reduction; switch if rash recurs after restarting |
| Fluid Retention / Edema | Imatinib (most common) | Compression stockings for LE edema; diuretics if needed; monitor weight | Usually manageable without switching; dose reduction if severe |
| Muscle Cramps / Spasms | Imatinib | Check K+/Ca2+/phosphate; correct electrolytes; tonic water (quinine); hydration, stretching; check CK levels | Usually manageable; rarely need to switch |
| Cytopenias (ANC/plt/Hgb) | All TKIs | G-CSF for persistent neutropenia; transfusions per protocol; consider BM evaluation to rule out progression to AP/BP or other myeloid neoplasm | Growth factor support for persistent cytopenias; dose reduction per PI; cytopenias may persist after switching |
Cardiovascular Risk Monitoring (NCCN CML-C)
- Counsel ALL patients on CVD risk factors: diabetes, hypertension, hyperlipidemia, smoking, estrogen use — ABCDE prevention framework
- Cardiology referral RECOMMENDED for patients with CV risk factors for additional monitoring/assessment
- Identify drug interactions of TKIs with cardiovascular medications BEFORE prescribing (see Drug Interactions section)
- ABCDEs of CVD Prevention: A-Antiplatelet/Aspirin, B-Blood pressure, C-Cholesterol/Cigarettes, D-Diet/Diabetes, E-Exercise/Estrogen avoidance
SECTION 11: TKI DRUG INTERACTIONS (NCCN CML-D)
Always obtain a COMPLETE medication history including herbal supplements at EVERY visit. CYP3A4 interactions are the most clinically significant.
| Drug/Food | Asciminib | Bosutinib | Dasatinib | Imatinib | Nilotinib | Ponatinib |
|---|---|---|---|---|---|---|
| PPIs (omeprazole, pantoprazole, lansoprazole, etc.) | No major interaction | Decrease exp. AVOID* | Decrease exp. AVOID** (std formulation) | No major interaction | Decrease exp. AVOID* | Minor decrease |
| H2RAs (famotidine, ranitidine) | No major interaction | Decrease exp. AVOID* (if nec.: H2RA 2h AFTER bosutinib) | Decrease exp. AVOID** (if nec.: H2RA 2h AFTER dasatinib) | No major interaction | Decrease exp. AVOID* (if nec.: H2RA 2h AFTER or 10h BEFORE nilotinib) | No major interaction |
| Antacids | No major interaction | Decrease if concomitant. Use ≥2h before OR ≥2h after bosutinib | Decrease if concomitant. Use ≥2h before OR ≥2h after dasatinib | No major interaction | Decrease if concomitant. Use ≥2h before OR ≥2h after nilotinib | No major interaction |
| Antidepressants (fluoxetine, bupropion, citalopram) | No major interaction | Minor ↑ exp. QTc monitoring | Minor ↑ exp. QTc monitoring | Minor ↑ exp. QTc monitoring | AVOID if possible (cumulative QTc risk) | Minor ↑ exp. QTc monitoring |
| CV Meds (amiodarone, diltiazem, verapamil, simvastatin, atorvastatin) | No major interaction | ↑ exp. + arrhythmia risk. Strongly consider alt. cardiac med or TKI dose adj. | ↑ exp. + arrhythmia risk. Strongly consider alt. cardiac med or TKI dose adj. | ↑ exp. Strongly consider alt. or TKI dose adj. | ↑ exp. + arrhythmia risk. AVOID | ↑ exp. Strongly consider alt. or TKI dose adj. |
| Azole Antifungals (voriconazole, itraconazole, posaconazole, fluconazole ≥200mg) | ↑ exp. Strongly consider alt. antifungal or TKI dose adj. | ↑ exp. Strongly consider alt. antifungal or TKI dose adj. | ↑ exp. Strongly consider alt. antifungal or TKI dose adj. | ↑ exp. Strongly consider alt. antifungal or TKI dose adj. | ↑ exp. Strongly consider alt. antifungal or TKI dose adj. | ↑ exp. Strongly consider alt. antifungal or TKI dose adj. |
| Fluoroquinolones (levofloxacin, moxifloxacin, ciprofloxacin) | No major interaction | QTc monitoring | QTc monitoring | No major interaction | Use with caution | No major interaction |
| Herbal: St. John’s Wort | AVOID (CYP3A4 inducer ↓ exp.) | AVOID (↓ exp.) | AVOID (↓ exp.) | AVOID (↓ exp.) | AVOID (↓ exp.) | AVOID (↓ exp.) |
| Herbal: Turmeric, Ginkgo, Green Tea Extract | ↑ exp. Consider discontinuing supplement | ↑ exp. Consider discontinuing supplement | ↑ exp. Consider discontinuing supplement | ↑ exp. Consider discontinuing supplement | ↑ exp. Consider discontinuing supplement | ↑ exp. Consider discontinuing supplement |
| Fruits/Juices: Grapefruit, Star fruit, Black mulberry, Wild grape, Pomegranate | AVOID (CYP3A4 inhibitors) | AVOID | AVOID | AVOID | AVOID | AVOID |
CRITICAL: PHARMACIST WATCHOUT: Acid Suppression & TKIs — HIGH FREQUENCY INTERACTION
– PPI use is EXTREMELY COMMON in oncology patients — ALWAYS screen
– Bosutinib + nilotinib: PPIs ABSOLUTELY CONTRAINDICATED/AVOID — decreased TKI absorption due to pH-dependent solubility
– Dasatinib standard formulation: also avoid PPIs/H2RAs. NEW: pH-independent dasatinib formulation allows concurrent acid suppression — verify which formulation patient has
– If PPI absolutely required with bosutinib: NO viable safe alternative listed — consider TKI switch
– Antacids (Tums, Maalox): space at least 2 hours before OR 2 hours after for bosutinib/dasatinib/nilotinib
– Azole antifungals (voriconazole, posaconazole common in oncology): INCREASE ALL TKI levels — strong CYP3A4 inhibitors; consider TKI dose reduction or antifungal switch to fluconazole if possible
– St. John’s Wort: ABSOLUTE AVOID with ALL TKIs — CYP3A4 inducer causes sub-therapeutic TKI levels
– Grapefruit/exotic fruit juices: AVOID with ALL TKIs — list updated in v1.2026 to include star fruit, black mulberry, wild grape, pomegranate (in order of CYP3A4 inhibition potency)
SECTION 12: SPECIAL POPULATIONS
CML During Pregnancy (NCCN CML-E)
Male Patients
- TKI therapy does NOT need to be discontinued if pregnancy planned by female partner
- No elevated miscarriage or fetal abnormality rate in female partners of male patients on TKI
Female Patients — Pre-Conception
- TKI during pregnancy: HIGHER rate of miscarriage AND fetal abnormalities — strongly discourage conception on active TKI
- Discuss: prolonged washout period, holding TKI if pregnancy occurs, close monitoring
- Prior to attempting pregnancy: counsel on risks/benefits of TKI discontinuation, possible TKI resumption, treatment options during pregnancy
- Fertility preservation: discuss with ALL patients of childbearing age BEFORE TKI initiation; referral to IVF center; TKI stop before oocyte retrieval (≥1 month recommended)
- No published guidelines on minimum DMR depth for ‘safe’ pregnancy attempt; literature limited to case reports
Treatment DURING Pregnancy
- Preferred treatment during pregnancy: INTERFERON — peginterferon alfa-2a (preferred; may preserve molecular remission) or ropeginterferon alfa-2b (available but limited CML-specific data)
- TKI therapy during FIRST TRIMESTER: AVOID (teratogenic risk)
- Hydroxyurea: AVOID during pregnancy (especially first trimester)
- Leukapheresis: option for rising WBC/platelet count (no specific threshold defined)
- Low-dose aspirin or LMWH: consider for thrombocytosis
- Monthly CBC with differential + qPCR every 1–3 months during pregnancy
Breastfeeding
- TKIs pass into breast milk — ADVISE AGAINST breastfeeding while on TKI
- May be acceptable to delay TKI for first 2–5 days post-delivery to allow colostrum
- Breastfeeding without TKI may be considered in patients with DURABLE DMR — monthly molecular monitoring required
- Loss of MMR confirmed during breastfeeding → STOP breastfeeding and RESTART TKI
Pediatric CML
- Imatinib first-line for pediatric CP-CML (adult dosing guidelines not directly applicable)
- Dasatinib has pediatric approval for CP-CML
- Allogeneic HCT earlier consideration in pediatric patients
- Growth retardation, bone development effects: relevant long-term toxicity concern in children on TKIs
Elderly Patients
- Imatinib may be preferred for patients who are older with comorbidities such as cardiovascular disease (NCCN CML-2 footnote n)
- Nilotinib: USE CAUTION in elderly with diabetes, PAD, or prior MI — arterial/vascular events more common
- Ponatinib: high cardiovascular risk — particularly cautious in elderly with any CV risk factors
- Dose reductions may be needed more frequently; closer monitoring of renal/hepatic function
SECTION 13: KEY CLINICAL TRIALS (BRIEF SUMMARIES)
| Trial Name | Population | Intervention | Comparator | Key Outcomes |
|---|---|---|---|---|
| IRIS | Newly diagnosed CP-CML | Imatinib 400 mg QD | IFN-alpha + Ara-C | Superior CCyR (76% vs 14%); 10-yr OS 83.3%; established imatinib as standard of care; landmark trial |
| ENESTnd | Newly diagnosed CP-CML | Nilotinib 300 mg BID or 400 mg BID | Imatinib 400 mg QD | Higher MMR and MR4.5 at 12 mo; superior MCyR at 12 mo; fewer progressions to AP/BP; more CV events with nilotinib long-term |
| DASISION | Newly diagnosed CP-CML | Dasatinib 100 mg QD | Imatinib 400 mg QD | Faster and deeper molecular responses vs. imatinib; higher MMR at 12 mo; more pleural effusions with dasatinib; similar 5-yr OS |
| BFORE | Newly diagnosed CP-CML | Bosutinib 400 mg QD | Imatinib 400 mg QD | Higher MMR at 12 mo (47.2% vs 36.9%, p=0.02); superior CCyR at 12 mo; more GI and LFT AEs with bosutinib vs. imatinib |
| ASC4FIRST | Newly diagnosed CP-CML | Asciminib 40 mg BID | Investigator-selected imatinib or 2G TKI (dasatinib/nilotinib/bosutinib) | Superior MMR at 48 weeks vs. all comparators; better tolerability profile vs. 2G TKIs; established 1st-line Cat 1 indication for asciminib |
| ASCEMBL | CP-CML resistant/ intolerant to ≥2 TKIs, no T315I | Asciminib 40 mg BID | Bosutinib 500 mg QD | Superior MMR at 24 weeks (25.5% vs 13.2%); better tolerability; led to asciminib approval for 3rd-line+ CP-CML |
| PACE | CP/AP/BP-CML resistant/ intolerant to ≥2 TKIs or T315I | Ponatinib 45 mg QD | Single-arm | MCyR in 54% CP-CML; high activity in T315I; CV events in 9% at 5 yrs; led to ponatinib approval for T315I and ≥3rd-line CML |
| EURO-SKI | CP-CML in MR4.0 on imatinib | Imatinib discontinuation (TFR attempt) | Single-arm | MR4.0 ≥3 years = strongest predictor for successful TFR; TKI duration ≥6 yrs also predictive; NK cell count predictive of outcome |
SECTION 14: TKI AGENT PROFILES — PHARMACIST REFERENCE
| Agent (Brand) | Class/Mechanism | Key Adverse Effects | Clinical Pearls / Pharmacist Counseling |
|---|---|---|---|
| Imatinib (Gleevec; generics available) | 1G TKI; competitive BCR::ABL1 kinase inhibitor (ATP-binding site); also inhibits c-KIT and PDGFR | Edema/periorbital edema, nausea, muscle cramps, rash, diarrhea, myelosuppression, hepatotoxicity, fluid retention. Less CV toxicity than 2G TKIs. | Take WITH food to reduce GI upset. Generics are bioequivalent and interchangeable per FDA. Preferred in elderly with CV disease. Monitor LFTs. Muscle cramps: check Ca/K/Mg, tonic water. |
| Dasatinib (Sprycel; generic available) | 2G TKI; inhibits BCR::ABL1 + SRC kinases; active against most imatinib-resistant mutations except T315I; pH-independent formulation (NEW) | Pleural effusion (most distinctive AE), myelosuppression, PAH (rare but serious), GI bleeding, edema, diarrhea, rash, QT prolongation (less than nilotinib) | PLEURAL EFFUSION: monitor symptoms (SOB, chest pain, cough); diuretics + corticosteroids + dose reduction. Best CNS penetration — preferred in CNS-involved CML. Check formulation for acid suppression compatibility. No food restrictions. |
| Nilotinib (Tasigna; generic available) | 2G TKI; more potent/selective BCR::ABL1 inhibitor than imatinib; active against most imatinib-resistant mutations except T315I, Y253H, E255K/V, F359V/C/I | QT prolongation (most significant), hyperglycemia, CV/arterial events (PAOD, MI, stroke — BLACK BOX), pancreatitis, rash, hyperbilirubinemia, headache | FASTING REQUIRED — capsule formulation. Correct K+/Mg2+ BEFORE starting. ECG at baseline, 7 days, and after dose changes. Avoid PPIs/H2RAs/antacids. AVOID in diabetes/PAD/prior CV events. Different formulations/strengths NOT interchangeable. |
| Bosutinib (Bosulif) | 2G TKI; inhibits BCR::ABL1 + SRC kinases (similar to dasatinib); minimal c-KIT/PDGFR activity (less edema/effusion than imatinib/dasatinib); active against most imatinib-resistant mutations except T315I, V299L, G250E, F317L | DIARRHEA (most common — early onset, usually resolves), nausea/vomiting, hepatotoxicity (LFT elevations most common with 2G TKIs), rash, thrombocytopenia | Take WITH FOOD — essential for GI tolerability. Avoid PPIs/H2RAs (pH-dependent absorption). Prophylactic loperamide may be considered at treatment initiation. Monitor LFTs frequently first 6 months. 400 mg QD (1st line), 500 mg QD (2nd+ line). |
| Ponatinib (Iclusig) | 3G TKI; pan-BCR::ABL1 inhibitor; ONLY agent active against T315I mutation; also inhibits VEGFR, FGFR, PDGFR, c-KIT, SRC. Multi-kinase inhibitor. | ARTERIAL/VASCULAR EVENTS — MI, stroke, PAD (BLACK BOX — can occur in absence of traditional CV risk factors); hypertension; pancreatitis; hepatotoxicity; myelosuppression; skin rash; DRY SKIN | Strict indication verification required. Start at 45 mg; REDUCE to 15 mg QD once CCyR achieved (NCCN v1.2026). Monitor BP closely — switch for severe uncontrolled HTN. Document CV risk assessment. Lower starting dose appropriate risk-reduction strategy per NCCN. No food restriction. |
| Asciminib (Scemblix) | Allosteric TKI; STAMP inhibitor (Specifically Targeting the ABL1 Myristoyl Pocket) — completely different mechanism from 1G/2G/3G TKIs; can be combined with ATP-competitive TKIs in some cases; no cross-resistance except ASXL1 pocket mutations | Hypertension, pancreatitis, myelosuppression, fatigue, musculoskeletal pain, rash, hypersensitivity reactions; QTc prolongation at T315I dose (200 mg BID) | FASTING required (like nilotinib). VERIFY DOSE: 40 mg BID (standard) vs. 200 mg BID (T315I ONLY) — different dose for same drug. CONTRAINDICATED in e13a3/e14a3 transcripts. 1st-line Cat 1 approval (ASC4FIRST). Completely different MOA from other TKIs. Monitor BP. |
SECTION 15: CLINICAL PEARLS & PHARMACIST WATCHOUT SUMMARY
Top Clinical Pearls for Hem/Onc Pharmacist Rounds
PEARL 1: Transcript Type = Treatment Selection (NCCN v1.2026 Update)
– ALWAYS check BCR::ABL1 transcript type before prescribing asciminib
– b2(e13)a3 and b3(e14)a3: asciminib has NO clinical activity and is CONTRAINDICATED
– e1a2 (p190) and e19a2 (p230): worse prognosis; consider referral to CML specialty center
– Standard IS qPCR monitoring NOT valid for atypical transcripts (e13a3, e14a3) — need qualitative RT-PCR
PEARL 2: Food Interactions — The Most Counseling-Critical TKI Difference
– NILOTINIB: EMPTY STOMACH (fasting) — capsule formulation; 2 hrs before/1 hr after — counseling priority #1
– ASCIMINIB: EMPTY STOMACH — same fasting requirement (do not eat 2 hrs before, 1 hr after)
– BOSUTINIB: WITH FOOD — opposite of nilotinib/asciminib; GI tolerability depends on taking with food
– IMATINIB: WITH food to reduce GI upset — no strict fasting required
– DASATINIB: no food restriction (standard formulation); pH-independent formulation expands acid suppression flexibility
PEARL 3: T315I = Gatekeeper Mutation — Know Your Options
– T315I: resistant to ALL 1G and 2G TKIs (imatinib, dasatinib, nilotinib, bosutinib)
– Active agents: PONATINIB (preferred for AP/BP-CML or any T315I) or ASCIMINIB 200 mg BID
– Asciminib dosing doubles for T315I: 200 mg BID vs. standard 40 mg BID — verify on every order
– Ponatinib dose reduction strategy: 45 mg → 15 mg QD once CCyR achieved (reduces CV events)
PEARL 4: Treatment Response Milestones — Know the Color Code
– 3 months: BCR::ABL1 >10% = YELLOW (possible resistance, consider switch or continue and recheck at 6 months)
– 6 months: BCR::ABL1 >10% = RED (TKI-resistant; SWITCH TKI); 1-10% = ORANGE (possible resistance; consider switch)
– 12 months: BCR::ABL1 0.1-1% = LIGHT GREEN (evaluate treatment goal — TFR goal or survival only); ≤0.1% = GREEN
– ALWAYS check adherence and drug interactions BEFORE declaring resistance
– BCR::ABL1 must be on International Scale (IS) for valid interpretation
PEARL 5: TFR — The Ultimate Goal in Eligible Patients
– Criteria: CP-CML, ≥3 years TKI, MR4.0 (≤0.01% IS) ≥2 years documented on ≥4 tests ≥3 months apart
– qPCR sensitivity must be at least MR4.5 for monitoring post-discontinuation
– TKI WITHDRAWAL SYNDROME: musculoskeletal/joint pain in ~20-30% — counsel patients proactively
– Age ≥18 years requirement REMOVED in NCCN v1.2026
– Restart TKI within 4 WEEKS of confirmed loss of MMR — don’t wait
CRITICAL: PHARMACIST WATCHOUT SUMMARY — HIGH-PRIORITY SAFETY ISSUES
#1 ACID SUPPRESSION: PPIs CONTRAINDICATED with bosutinib and nilotinib (pH-dependent absorption). SCREEN EVERY PATIENT.
#2 QTc: Nilotinib — mandatory baseline ECG, Day 7 ECG, correct K+/Mg2+ before start; antidepressants + fluoroquinolones + nilotinib = triple QT risk
#3 GRAPEFRUIT/FRUIT JUICES: ALL TKIs — avoid grapefruit, star fruit, black mulberry, wild grape, pomegranate (all CYP3A4 inhibitors, updated v1.2026)
#4 AZOLE ANTIFUNGALS: increase ALL TKI levels significantly — common combination in immunocompromised patients; always flag and recommend dose adjustment or antifungal switch
#5 PONATINIB CV RISK: Document indication (T315I or ≥2 prior TKIs) before approval. Black box for arterial events. Reduce dose to 15 mg after CCyR.
#6 NILOTINIB FORMULATION: Different formulations/strengths NOT interchangeable. Capsule = fasting required. Refer to package insert.
#7 ASCIMINIB DOSE VERIFICATION: 40 mg BID (standard) vs. 200 mg BID (T315I ONLY) — same drug, very different doses; always verify mutation status.
#8 HEPATITIS B REACTIVATION: Screen (HBsAg, anti-HBc, anti-HBs) before ALL TKIs. Prophylaxis if positive markers.
#9 PREGNANCY: TKIs are teratogenic — verify pregnancy status in all reproductive-age patients; counsel on contraception; peginterferon preferred if treatment needed during pregnancy.
#10 GENERICS: Monitor closely when transitioning from brand to generic nilotinib or bosutinib — narrow therapeutic window; pharmacokinetic variability possible.
#11 HYDROXYUREA: Use as BRIDGE ONLY (to lower WBC until TKI starts) — NOT a long-term CML treatment; AVOID in pregnancy.
#12 MYELOID MUTATIONAL ANALYSIS: If no BCR::ABL1 kinase domain mutation found on resistance workup, consider broader myeloid mutation panel (ASXL1, etc.) — independent resistance mechanisms exist.
Quick Reference — TKI Toxicity by Drug
| Toxicity | Imatinib | Dasatinib | Nilotinib | Bosutinib | Ponatinib | Asciminib |
|---|---|---|---|---|---|---|
| QT Prolongation | + | + | +++ | + | + | + (especially 200 mg BID dose) |
| Pleural Effusion | – | +++ | – | + | + | – |
| CV/Arterial Events | – | – | ++ | – | +++ | + (HTN primarily) |
| Pancreatitis | – | – | ++ | – | ++ | ++ (asciminib notable for pancreatitis) |
| Hyperglycemia | – | – | +++ | – | – | – |
| GI (Diarrhea/Nausea) | ++ | + | + | +++ | + | + (less than bosutinib) |
| Hepatotoxicity | ++ | + | + | +++ | + | -/+ |
| Edema/Fluid Retention | +++ | + | – | – | – | – |
| Muscle Cramps | +++ | + | – | – | – | -/+ |
SOKAL/HASFORD/ELTS Risk Score Reminders
– Use calculator: leukemia-net.org Inputs needed: Age, Spleen (cm below CM), Platelet count, % blasts in PB, % eosinophils (Hasford), % basophils (Hasford)
– Intermediate/High risk → prefer 2G TKI or asciminib over imatinib (NCCN Cat 1)
When to Check BCR::ABL1 Kinase Domain Mutations
– Response milestones NOT reached
– Loss of hematologic response
– Loss of CCyR/MR2.0 (BCR::ABL1 >1%)
– 1-log increase in BCR::ABL1 + loss of MMR
– Progression to AP/BP-CML