Members of the Class
| Agent | Brand Name(s) | Primary Setting |
|---|---|---|
| Cytarabine (IV/SC/IT) (conventional) | Cytosar-U | AML, ALL, lymphomas |
| Cytarabine liposomal + Daunorubicin liposomal (IV) (combination) | Vyxeos | AML (therapy-related / MRC) |
| Cytarabine liposomal (IT) | DepoCyt | Lymphomatous/leukemic meningitis |
| Gemcitabine (IV) | Gemzar | Solid tumors (pancreatic, NSCLC, bladder, breast, ovarian, lymphoma) |
| Azacitidine (SC/IV) | Vidaza | MDS, AML (low-blast), CMML |
| Azacitidine (oral) | Onureg (CC-486) | AML maintenance post-remission |
| Decitabine (IV) | Dacogen | MDS, AML |
| Decitabine / Cedazuridine (oral) (fixed-dose combination) | Inqovi | MDS, CMML |
Cytidine analogs are a subclass of antimetabolite agents structurally derived from the naturally occurring pyrimidine nucleoside cytidine. Despite sharing a common structural scaffold, clinically relevant cytidine analogs differ substantially in their biochemical mechanisms, cellular targets, indications, and toxicity profiles.
Mechanism of Action (Class-Wide)
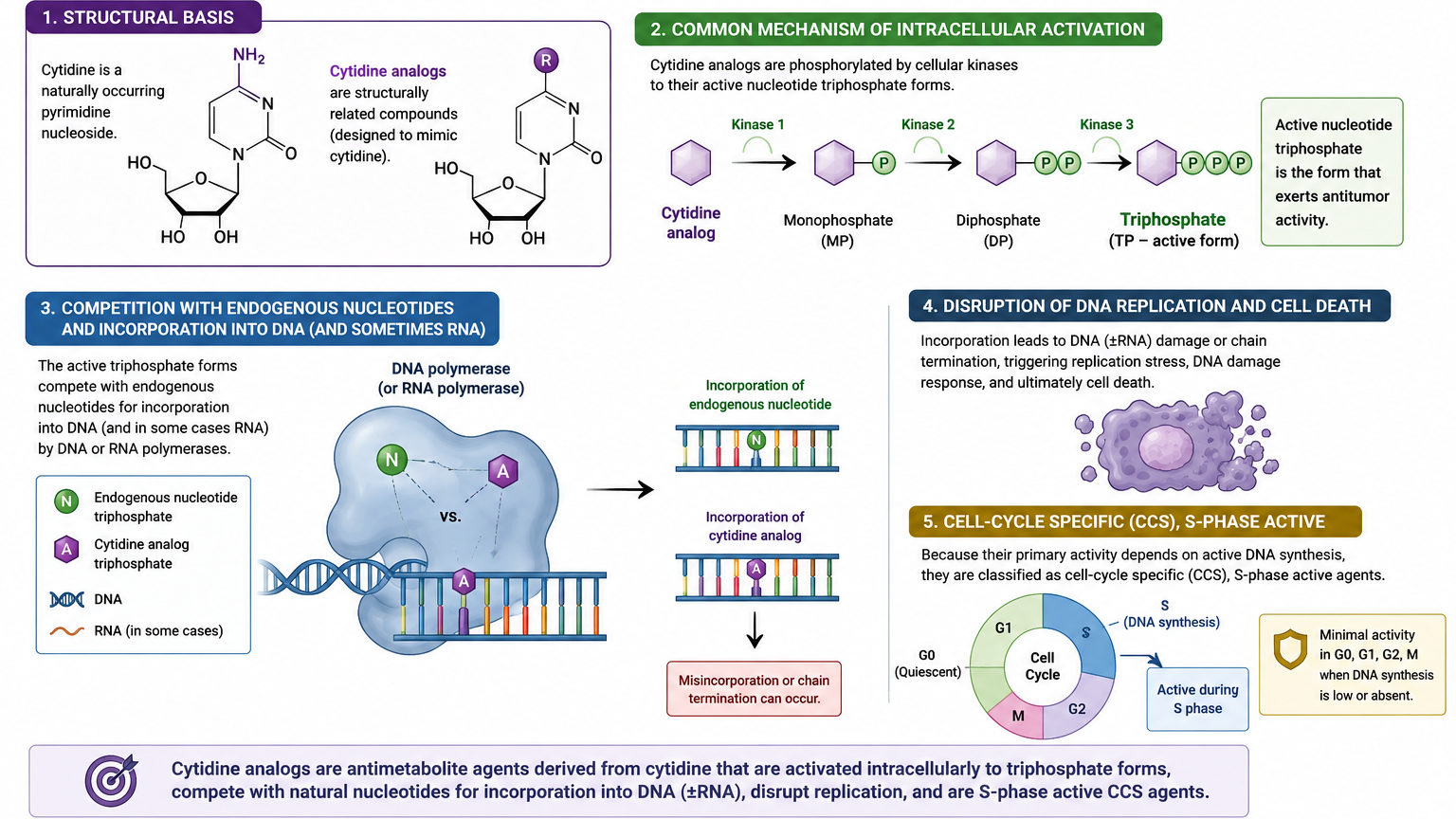
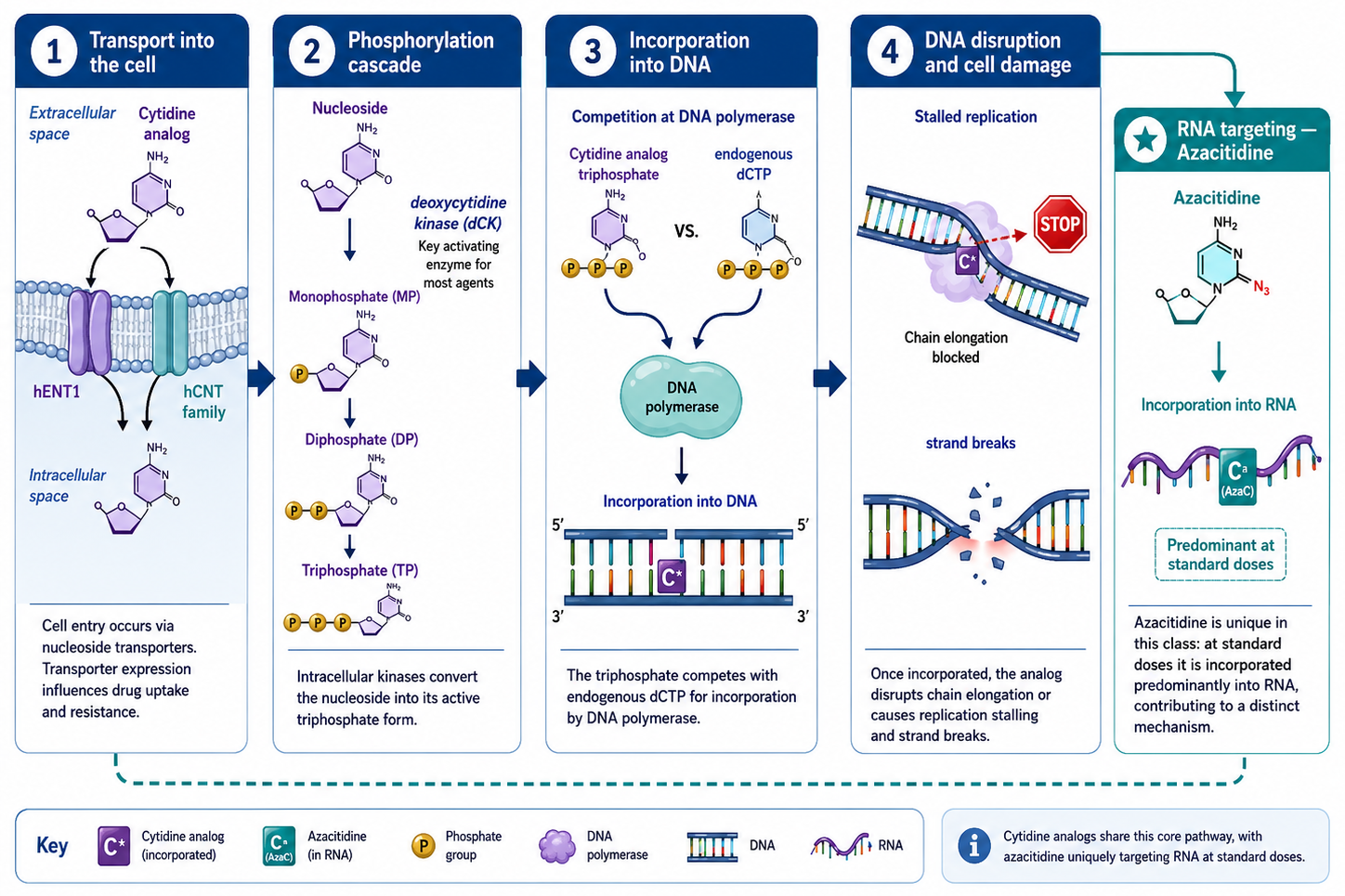
All cytidine analogs undergo a shared pattern of intracellular activation:
- Transport into the cell — via nucleoside transporters (predominantly hENT1 and hCNT family); transporter expression is a determinant of drug uptake and resistance
- Phosphorylation cascade — sequential phosphorylation by intracellular kinases (e.g., deoxycytidine kinase [dCK] for most agents) converts the nucleoside to its monophosphate → diphosphate → triphosphate active form
- Incorporation into DNA — the triphosphate competes with the endogenous dCTP pool for incorporation by DNA polymerase; once incorporated, the analog disrupts chain elongation or triggers stalling and strand breaks
- RNA targeting — azacitidine (uniquely among this class) is predominantly incorporated into RNA rather than DNA at standard doses, contributing to its distinct mechanism
Divergence Within the Class
- Cytarabine (ara-C): After phosphorylation to ara-CTP, it incorporates into DNA, inhibits DNA polymerase-α, and causes chain termination. High intracellular ara-CTP levels relative to competing dCTP determine cytotoxic efficacy — the basis for high-dose cytarabine (HiDAC) strategies.
- Gemcitabine (dFdC): A difluorinated analog. Its diphosphate form inhibits ribonucleotide reductase (RNR), depleting the dCTP pool and secondarily enhancing gemcitabine triphosphate incorporation (self-potentiation). Its masked chain termination (incorporation of one additional nucleotide after gemcitabine triphosphate before arrest — “masked chain termination”) makes it resistant to exonuclear proofreading, contributing to its potency.
- Azacitidine: Primarily incorporated into RNA at standard doses, inhibiting ribosomal RNA processing and protein synthesis; at lower levels, its deoxy-metabolite (5-aza-dCTP) incorporates into DNA and covalently traps and depletes DNMT1/3, reversing hypermethylation of tumor suppressor gene promoters.
- Decitabine (5-aza-dC): A deoxyribose analog that bypasses the RNA incorporation step entirely; fully directed toward DNA, where it acts as a DNMT inhibitor at low concentrations and a DNA chain terminator at higher concentrations. Clinical HMA dosing intentionally stays in the low-dose range to maximize epigenetic activity over cytotoxicity.
Unique azacitidine and decitabine mechanism of action
- Azacitidine and decitabine are frequently grouped separately as hypomethylating agents (HMAs). While technically members of the cytidine analog family, their dominant pharmacologic mechanism — inhibition of DNA methyltransferases (DNMTs) at low doses — distinguishes them functionally from cytarabine and gemcitabine, which act primarily as chain terminators.
- At high (cytotoxic) doses → cytotoxic (chain termination)
- At low (epigenetic) doses → epigenetic reprogramming (DNMT inhibition) leading to the removal of methyl groups (hypomethylation) from the DNA, which “switches on” epigenetically silenced genes (such as tumor suppressors) and helps reprogram the cancer cells. Adding a methyl group is a gene-silencing mechanism.
- Unlike high-dose, traditional chemotherapy, which violently attacks and kills rapidly dividing cells, lower doses of azacitidine allow abnormal cells to live but force them to mature → normal myeloid maturation. That is why it takes time for a response, because it unsilences genes instead of directly damaging the DNA.
- Azacitidine is a ribonucleoside — it incorporates predominantly into RNA, not DNA, at standard doses. This inhibits rRNA processing, tRNA function, and protein synthesis
- Decitabine is a deoxyribonucleoside — it goes directly and exclusively into DNA, making it a purer DNMT inhibitor with no RNA component.
Resistance Mechanisms (Class-Wide)
Understanding resistance is clinically relevant both for anticipating treatment failure and for the rationale behind combination strategies:
- Reduced nucleoside transporter expression (↓ hENT1) — decreased cellular uptake; relevant for cytarabine and gemcitabine
- Downregulation or loss of activating kinases — particularly dCK; reduces phosphorylation to active triphosphate
- Upregulation of catabolic enzymes — cytidine deaminase (CDA) degrades cytidine analogs back to inactive uracil forms; the rationale for combining decitabine with cedazuridine (a CDA inhibitor) in Inqovi to enable oral bioavailability
- Expansion of competing dCTP pool — upregulation of RNR increases endogenous dCTP, diluting analog incorporation; gemcitabine’s RNR inhibition partially counteracts this
- Enhanced DNA repair — increased base excision or nucleotide excision repair removes incorporated analogs before lethal damage occurs
Toxicity Profile (Class Theme)
While individual toxicity profiles are addressed under each agent, cytidine analogs share several class-wide themes:
- Myelosuppression — universal, dose-dependent; expected and monitored closely in hematologic malignancies where marrow compromise is often already present
- Mucositis / GI toxicity — related to the high proliferative rate of GI epithelium; more pronounced with cytarabine and gemcitabine than HMAs
- Hepatotoxicity — transaminase elevations seen across the class; dose modification thresholds vary by agent
- Neurotoxicity — predominantly cerebellar toxicity with high-dose cytarabine (a critical monitoring requirement); less prominent with gemcitabine or HMAs
- Pulmonary toxicity — gemcitabine-associated pneumonitis and capillary leak are the most clinically significant within the class
- Injection site reactions — especially azacitidine SC (erythema, induration at injection sites)
- Teratogenicity / embryo-fetal toxicity — class-wide; all agents require effective contraception and are contraindicated in pregnancy
Formulations
Several agents in this class exist in multiple formulations with meaningfully different clinical roles — they are not interchangeable:
- Cytarabine conventional IV/SC vs. Vyxeos (liposomal cytarabine:daunorubicin 5:1 molar ratio) vs. DepoCyt (liposomal intrathecal) — three distinct products, distinct indications, non-substitutable
- Azacitidine IV/SC (Vidaza) vs. oral azacitidine (Onureg) — same molecule, but oral formulation achieves prolonged low-level exposure by design, optimized for AML maintenance rather than induction-level HMA activity
- Decitabine IV (Dacogen) vs. decitabine/cedazuridine oral (Inqovi) — Inqovi leverages CDA inhibition to replicate IV decitabine PK orally; it is not simply an oral version of Dacogen but a co-formulated product requiring its own prescribing logic