- Anticancer causative agent: Dasatinib, PI3Ki (Alpelisib, Inavolisib, Copanlisib, Duvelisib, Idelalisib, Umbralisib), JAKi (Momelotinib, Ruxolitinib, Fedratinib, Pacritinib), Alemtuzumab
- Antiviral Prophylaxis (proteasome, BTKi): Valacyclovir, foscarnet (if ganciclovir resistant/intolerant)
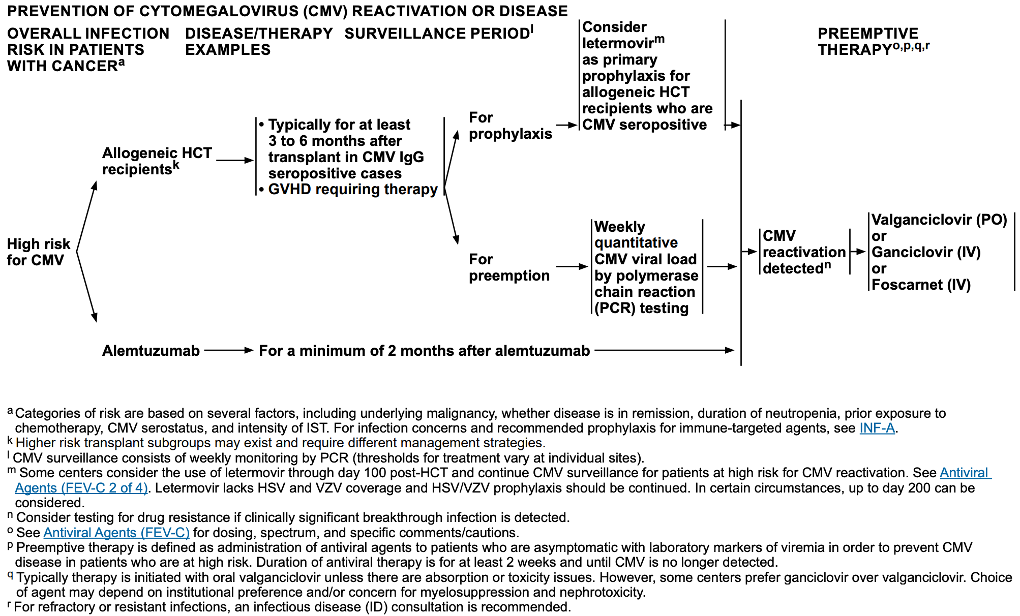
- Surveillance (Alemtuzumab, post alloHCT) : weekly PCR during therapy and ≥2mo after completion of therapy.
Letermovir has no activity against HSV, additional HSV coverage might be warranted (like acyclovir)
| Medication | Spectrum | ADE and Clinical Pearls |
| Ganciclovir IV | CMV HSV/VZV | Preemptive therapy for CMV: 5 mg/kg BID; if CMV remains detectable, further ID evaluation may be requiredTreatment: CMV disease (5 mg/kg BID for induction followed by 5 mg/kg daily for maintenance and resolution of all symptoms)Make cause bone marrow suppressionClinical data unlimited for HHV-6 and HHV-8 |
| Valganciclovir PO | CMV HSV/VZV | Preemptive therapy and treatment for CMV: Induction with 900 PO BID for induction and until negative test; consider additional 900 mg PO daily for maintenance after negative testMake cause bone marrow suppressionClinical data unlimited for HHV-6 and HHV-8 |
| Cidofovir IV | CMV HSV/VZV Adenovirus | Treatment: 5 mg/kg IV weekly x2wks, followed by 5 mg/kg IV q2wk with probenecid 2g PO 3h before the dose, followed by 11g PO 2h after the dose and 1g PO 8h after the doseHydration and probenecid are required to reduce nephrotoxicityOcular toxicity, bone marrow toxicityEvidence is limited for treatment of adenovirus; when used, ID consult is strongly recommended |
| Foscarnet IV | HSV/VZV CMV HHV-6 | Prophylaxis for CMV: 60 mg/kg IV q8-12h for induction, followed by 90-120 mg/kg IV daily for maintenance after HCTPre-emptive therapy for CMV: induction; either 60 mg/kg IV q8h or 90 mg/kg IV q12hTreatment IV (ganciclovir-resistant CMV drug of choice): 90 mg/kg q12h for induction followed by 90-120 mg/kg daily for maintenance and resolution of all symptoms ADE: nephrotoxic; monitor electrolytesLimited clinical data for HHV-6/HHV-8. Treatment should be reserved for clinically documented disease; ID consult is highly recommended. |
| Letemovir PO/IV | CMV | Primary prophylaxis for alloHCT recipients who are CMV seropositive: 480 mg PO daily or daily IV infusion over 1h post-txp. Reduce dose to 240 mg PO/IV daily if co-administered with cyclosporineHas not been studied as an angent for treatmentHas multiple drug interactions, including azoles, cyclosporine, and tacrolimus; see package insert TDM is importantNot active against other herpes group viruses. Acyclovir is also needed for HSV/VZV. |
| Mirabavir PO | CMV | Treatment 400 mg PO BIDIndicated for post-transplant CMV infection refractory to ganciclovir/valganciclovir, foscarnet, and cidofovir. ID consult is highly recommendedNo activities against HSV/VZV, HHV-6Inhibitor of HCMV-encoded kinase UL97Virologic failure due to resistance can occur and cross-resistance between maribavir and ganciclovir/valganciclovir has been observed Not recommended to be co-administered with ganciclovir/valganciclovir has been observedMonitor for drug interactions (may increase level of immunosuppressants such as cyclosporine, tacrolimus, sirolimus, etc.)May cause dysgeusia |