Clinical Pearls
- Most common aggressive NHL, but potentially curable with R-CHOP. Goal of therapy is cure. Can arise de novo or from transformation of indolent lymphomas (FL, MZL). 70% present with advanced stage.
- Prognostic tools
- IPI (aggressive NHL): age >60yo, stage III/IV, ECOG ≥2, LDH >UNL, ≥2 extranodal sites. Low (0-1, 5yr OS 91%), low-intermediate (2, 5yr OS 65-81%), high-intermediate (3, 5yr OS 65-81%), high (4-5, 5yr OS 59%).
- Age-adjusted IPI (aggressive NHL, ≤60yo): stage III/IV, ECOG ≥2, LDH >ULN. Low (0), low-intermediate (1), high-intermediate (2), high (3).
- smIPI (localized intermediate/high-grade, stage I-II): age >60yo, stage II/IIE, ECOG ≥2, LDH >ULN. Low (0-1), high (2-4).
- CNS-IPI (need for CNS prophylaxis): age >60yo, stage III-IV, ECOG ≥2, LDH > ULN, ≥2 extranodal site, kidney and adrenal involvement. High risk (4-6, kidney/adrenal involvement) shows 2-year CNS relapse of ~10%. Relapse with CNS occur early (poor prognosis) with median survival of 2-5 months.
- Independent risk factors: Testicular lymphoma, primary cutaneous DLBCL (leg type), breast DLBCL (stage IE), kidney or adrenal gland involvement, uterine (not ovarian), paranasal or parameningeal, orbital, bone-marrow, high-grade lymphoma, HIV-associated lymphoma, ABC cell of origin.
- CNS prophylaxis:
- Leptomeningeal (BL): IT MTX/Cytarabine (4-8 doses). May consider Ommaya reservoir placement, systemic.
- Parenchymal (HGBL, DLBCL): Systemic HD-MTX (3-3.5 g/m2 for 2-4 cycles; D15 of 21-d cycle) + G-CSF.
- Genomics (CD20+, CD45+, CD3-): CD20 is 100% expressed (Rituximab).
- Prognostic subtypes (FISH): Translocation of MYC, BCL2, BCL6. Double-hit HGBL is MYC + BCL2 or BCL6. Triple-hit HGBL is MYC + BCL2 + BCL6. DEL is overexpression (not translocation) of MYC and BCL2.
- Morphological (gene expression profiling): ABC (MYD88, CD79B; worse prognosis), GCB (BCL2, BCL6, EZH2; better).
- Differential diagnosis: LBCL IRF4/MUM1 (peds, Waldeyer’s ring, aggressive),
- First-line: R-CHOP, R-pola-CHP (if IPI≥2), DA-R-EPOCH (DHL or aggressive DEL).
- Localized (stage I-II, nonbulky <7.5cm): R-CHOP x3 cycles; if CR (R-CHOP +1 cycle or ISRT), if PR (R-CHOP +1-3 cycle ±ISRT), if progressive disease (repeat biopsy).
- FLYER (non-inferiority, CHOP x4 cycles + Rituximab x6 cycles vs R-CHOP x6 cycles; no risk age-adjusted IPI, <60 yo) showed non-inferior outcome; similar 3yr PFS, EFS, OS; lower total and non-heme toxicity.
- Advanced (stage I-II, bulky ≥7.5 cm): R-CHOP x6 cycles ± ISRT.
- GELA (R-CHOP vs CHOP) showed higher PFS, CR, OS in elderly (60-80 age); less ttt failure and death; similar ADE.
- Advanced (stage II with extensive mesenteric disease, stage III-IV): R-CHOP x6 cycles, R-pola-CHP x6 cycles, DA-R-EPOCH.
- POLARIX (R-pola-CHP vs R-CHOP; f/b R x2 cycles) showed superior PFS; similar EFS, OS, FN, G3+ infection. Short follow-up, costly. Some prefers in non-GCB tumors.
- CALGB/Alliance 50303 (DA-R-EPOCH vs R-CHOP) showed similar EFS, OS; higher ADE (FN, PN, thrombocytopenia) and longer infusion (96h for etoposide, doxorubicin, vincristine). Etoposide effect is synergistic with CHOP.
- Localized (stage I-II, nonbulky <7.5cm): R-CHOP x3 cycles; if CR (R-CHOP +1 cycle or ISRT), if PR (R-CHOP +1-3 cycle ±ISRT), if progressive disease (repeat biopsy).
- First-line for poor left ventricular function: DA-R-EPOCH, R-CDOP, R-CEOP, R-GCVP.
- Firstline in >80yo with comorbidities: R-CDOP (D: liposomal doxorubicin), R-mini-CHOP, R-GCVP.
- R-mini-CHOP: Ritux 375 mg/m² D1, Cyclophos 400 mg/m² D1, Doxo 25 mg/m² D1, Vincr 1 mg D1, Predni 40 mg/m² D1–5.
- Relapsed/Refractory DLBCL: relapse within 2 years (20-25%), primary refractory with R-CHOP (10-15%). Risk factors for relapse >2yr are age>60, advanced stage, IPI>2. Goal of therapy is cure.
- 2L, relapse <12mo or primary refractory (CAR-T eligible): Yescarta (axi-cel, Category 1), Breyanzi (liso-cel, Category 1)
- Bridging therapy: platinum-based chemo (DHAP±R, GDP±R, ICE±R, GemOx±R), PV±Bendamustine±Rituximab (Bendamustine after leukapheresis), ISRT (monotherapy or sequential).
- ZUMA-7 (conditioning chemo f/b Yescarta vs platinum-regimen f/b high-dose chemo with autoSCT if responsive) showed superior EFS (HR 0.4), higher 4yr OS (HR 0.73), higher ORR (83% vs 50%) and double CR (65% vs 32%); G3+ CRS (6%), neurological events (21%) but no death related to CRS/ICANS.
- TRANSFORM (conditioning chemo FluCy f/b Breyanzi vs 2L x 3C f/b high-dose chemo with autoSCT if CR/PR) showed higher EFS (HR 0.34), higher PFS and CR.
- 2L, relapse <12mo (CAR-T ineligible): BiTE (Epcoritamab + GemOx, Glofitamab + GemOx), PV±Bendamustine±R, PV+Mosunetuzumab, Tafasitamab+Lenalidomide (not in refractory primary, “chemo-free regimen”)
- Other options: platinum-based chemo (DHAP±R, GDP±R, ICE±R, ESHAP±R), GemOx (if BiTE ineligible), CEOP±R, MINE±R, BV (if CD30+), ibrutinib (non-GCB DLBCL), R2 (non-GCB DLBCL)
- 2L, subsequent therapy, relapse >12mo (ASCT eligible): platinum-based (DHAP±R, GDP±R, ICE±R, ESHAP±R, GemOx±R), MINE±R
- If CR: HD chemo f/b autoSCT ± ISRT (Category 1), alloSCT ± ISRT (consider); 75% relapse ~9mo of autoSCT.
- If PR: CAR T (anti-CD19; Yescarta, Breyanzi, Kymriah), HD chemo f/b autoSCT ± ISRT, alloSCT ± ISRT (consider).
- 2L, relapse >12mo (ASCT ineligible): CAR-T (if eligible, Breyanzi), BiTE [Epcoritamab+GemOx, Glofitamab+GemOx (category 1)], PV±Bendamustine±R, PV+Mosunetuzumab, Tafasitamab+Lenalidomide (“chemo-free regimen”)
- 2L, subsequent therapy, relapse >12mo (ASCT eligible): platinum-based (DHAP±R, GDP±R, ICE±R, ESHAP±R, GemOx±R), MINE±R
- Other options: CEOP±R, GDP±R, GemOx (if BiTE ineligible), Rituximab monotherapy, BV (if CD30+), ibrutinib (non-GCB DLBCL), R2 (non-GCB DLBCL)
- Include Rituximab if relapse after remission >6mo. Omit Rituximab if primary refractory.
- L-MIND (Tafasitamab+lenalidomide upto 12cycles f/b Tafasitamab monotherapy) showed ORR (57.5%), CR (41.2%); median DOR was NR, median OS (33.5mo), median PFS (11.6mo).
- 3L, subsequent therapy: CAR-T (Yescarta, Breyanzi, Kymriah; if not previously used), BiTE (Epcoritamab, Glofitamab; after ≥2L, including post-HCT/CAR-T), Loncastuximab tesirine (CD19 ADC), Selinexor (post SCT/CAR-T progression).
- EPCORE NHL-1 (Epcoritamab-bysp) showed ORR 61% (CR 38%), median DOR 15.6mo.
- NP30179 (Glofitamab-gxbm) showed ORR 56% (CR 43%), DOR 18.4 months, median time to response 42 days.
- LOTIS-2 (Loncastuximab tesirine) showed ORR 48.3% (CR 24.1%), median duration of response 10.3 months.
- SADAL (Selinexor): ORR 29% (CR 13%); of 39 patients PR/CR, 38% had response durations ≥ 6 months and 15% had response durations ≥12 months.
- “Rapid” infusion rituximab protocol in FL, DLBCL per MAXIMA trial, RATE trial and NCCN Guideline.
- If no grade ≥3 infusion reaction in Cycle 1, give Cycle 2 over 90 min (20% of dose in first 30 min, 80% over next 60 min) along with glucocorticoid-containing chemo regimen.
- If 90-min infusion is tolerated in Cycle 2, continue same rate for all remaining cycles (C6-8).
- Avoid 90-min infusion if clinically significant CV disease or high lymphocyte count (≥5000 cells/mm3) before C2.
- For mild-moderate reactions, interrupt or slow the infusion; restart at half the previous rate once symptoms improve.
- Rituxan Hycela® SC (+ endoglycosidase hyaluronidase human: enhancing SC permeability, speeding up drug absorption).
- Indication: ONLY if tolerated ≥1 full dose of rituximab IV.
- Premeds: APAP + antihistamine (glucocorticoids may be considered). Monitor for 15 minutes after each dose.
- Dosing (FL, DLBCL): 1,400 mg Rituximab/23,400 units hyaluronidase (11.7 mL of product) SC (abdomen) over ~5 mins, per the recommended schedule. Dosing is different with CLL.
- Rituximab Biosimilar (not interchangeable): -abbs (Truxima®), -pvvr (Ruxience®), -arrx (Riabni®)
- Bone-Health (steroid-containing regimen)
- Highest risk: women with chemo-induced menopause, older adults on chemo.
- Calcium intake from food, and supplements (Institute of Medicine recommendations).
- Evaluation one year after completing therapy: vitamin D 25-OH level, BMD. If deficient, replacement therapy.
- BMD osteopenia (T score -1.1 and -2.4): use FRAX to determine if drug therapy is necessary www.sheffield.ac.uk/FRAX/
- BMD osteoporosis, history of hip/vertebral fractures, asymptomatic vertebral compression deformity: initiate therapy (per National Osteoporosis Foundation guidelines), refer to endocrinologist. Therapy includes hormone replacement therapy, bisphosphonates or denosumab; avoid Teriparatide (CI in XRT).
- Special DLBCL Subtypes & Variants
- DEL (poor prognosis): consider R-EPOCH or R-pola-CHP over R-CHOP.
- DHL/THL: R-CHOP is NOT effective. DA-R-EPOCH, R-hyperCVAD; CNS ppx. High relapse rates; consider CAR-T if relapsed.
- Primary CNS Lymphoma (PCNSL): HD-MTX-based regimens (e.g., MTX + rituximab + temozolomide), not R-CHOP.
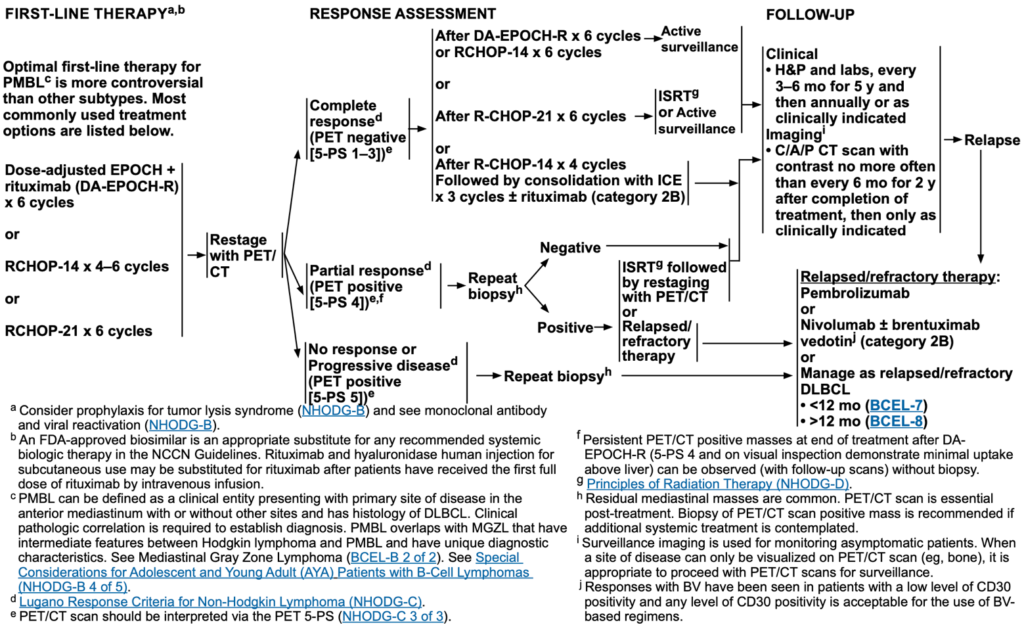
- Primary mediastinal large B cell lymphoma (PMBCL, rare): consider R-CHOP, R-EPOCH; PET-guided approach to XRT.
- HIV-associated DLBCL: Use EPOCH-like regimen + ART (antiretroviral therapy).
- Supportive Care Considerations
- TLS Prophylaxis (for bulky disease, high tumor burden, PV): Allopurinol 100 mg/m2/dose q8h upto 300-800mg/day (intermediate risk) or Rasburicase 0.2mg/kg/day (or flat dose 3-7.5 mg – 6mg) upto 5 days (high risk).
- Febrile Neutropenia ppx (DA-R-EPOCH, age≥65): G-CSF (filgrastim 5mcg/kg SC daily D6+ until ANC >0.5 x109/L of nadir). Use broad-spectrum antibiotics if febrile.
- Cardiotoxicity (Doxorubicin): monitor LVEF by ECHO/MUGA at baseline, then when needed. Use R-CHOP (if mild LVEF >40%), DA-R-EPOCH (if LVEF >35%), R-CDOP (if moderate LVEF), R-CEOP (if anthracycline is contraindicated).
- Neuropathy (Vincristine, Cisplatin): dose reduction/interruption if severe.
- CRS (Epcoritamab, Glofitamab, CAR T): Obinutuzumab 1g IV (7d prior Glofitamab as CRS mitigation); premeds of APAP, diphenhydramine, dexamethasone (Epcoritamab, Glofitamab, CAR T-cell therapy)
- Anticoagulation prophylaxis (Lenalidomide)
- HBV/HCV reactivation (Rituximab): screen at baseline, treat when needed.
- PJP Prophylaxis (Bendamustine, prolonged steroids): TMP-SMX or Dapsone.
- Monitoring & Response Assessment
- Interim PET-CT after cycle 2–4 helps guide therapy adjustments.
- End-of-treatment PET-CT: Use Deauville 5-point scale:
- Deauville 1–3 → Complete response.
- Deauville 4–5 → Consider biopsy or additional therapy.
- Minimal Residual Disease (MRD) testing emerging in DLBCL for better response tracking.
- Obinutuzumab-CHOP (G-CHOP) is not recommended in DLBCL per GOYA trial (G-CHOP vs R-CHOP) which showed similar PFS and higher G3+ adverse events (leading to dose reduction, interruption and treatment discontinuation)
Regimens
| Regimens | Medications |
|---|---|
| R-CHOP | Rituximab, Cyclophosphamide, doxorubicin (Hydroxydaunorubicin), vincristine (Oncovin), Prednisone |
| Pola-R-CHP (if IPI≥2) | Polatuzumab vedotin, Rituximab, Cyclophosphamide, doxorubicin (Hydroxydaunorubicin), Prednisone |
| DA-R-EPOCH [HGBL (DHL/THL), aggressive DEL] | Dose-Adjusted Rituximab, Etoposide, Prednisone, vincristine (Oncovin), Cyclophosphamide, doxorubicin (Hydroxydaunorubicin) |
| R-CDOP | Rituximab, Cyclophosphamide, liposomal Doxorubicin, vincristine (Oncovin), Prednisone |
| R-CEOP | Rituximab, Cyclophosphamide, Etoposide, vincristine (Oncovin), Prednisone |
| R-GCVP | Rituximab, Gemcitabine, Cyclophosphamide, Vincristine, Prednisone. |
| R-mini-CHOP (elderly and frail) | Rituximab 375 mg/m² D1, Cyclophosphamide 400 mg/m² D1, Doxorubicin 25 mg/m² D1 (Hydroxydaunorubicin), Vincristine 1 mg D1 (Oncovin), Prednisone 40 mg/m² D1–5 |
| DHAP | Dexamethasone, cytarabine (High-dose Ara-C), Platinum (carboplatin, cisplatin, oxaliplatin) |
| GDP | Gemcitabine, Dexamethasone, Platinum (carboplatin, cisplatin) |
| ICE | Ifosfamide, Carboplatin, Etoposide |
| ESHAP | Etoposide, methylprednisolone (Solu-Medrol), cytarabine (High-dose Ara-C), Platinum (cisplatin) |
| GemOx | Gemcitabine, Oxaliplatin |
| MINE | Mesna (uroprotectant, supportive), Ifosfamide, mitoxaNtrone, Etoposide |
Subtypes of DLBCL
Primary Mediastinal Large B-cell Lymphoma [PMBL]
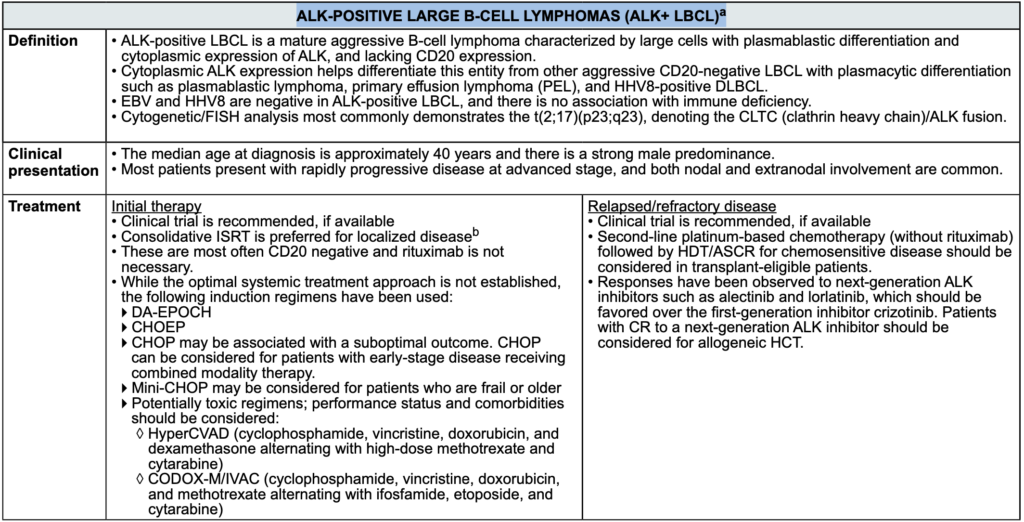
ALK-POSITIVE LARGE B-CELL LYMPHOMAS (ALK+ LBCL)a
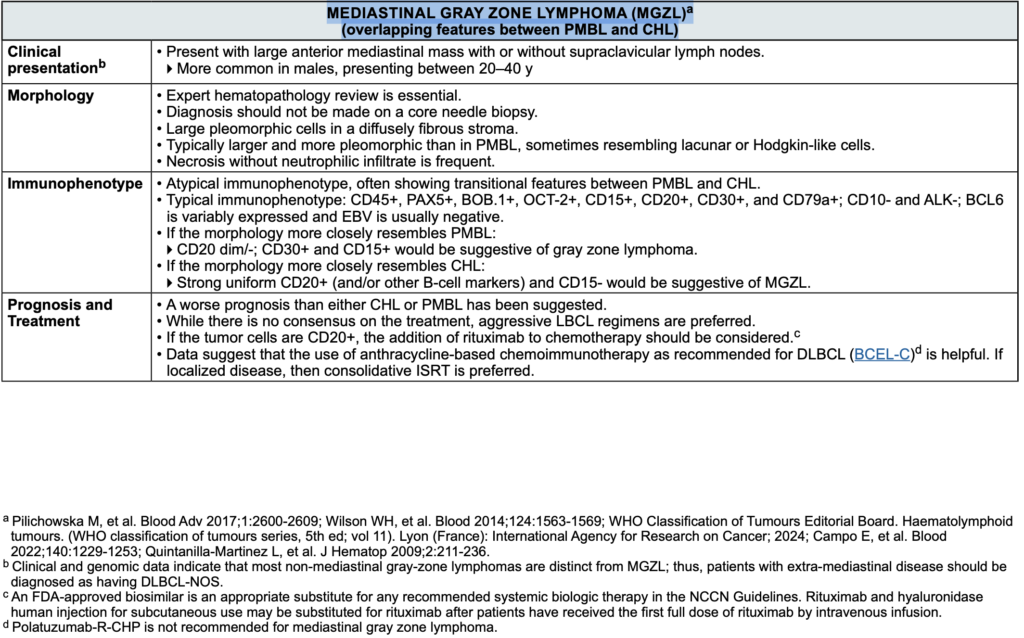
MEDIASTINAL GRAY ZONE LYMPHOMA (MGZL) (overlapping features between primary mediastinal large B-cell Lymphoma [PMBL] and classic Hodgkin lymphoma [CHL])
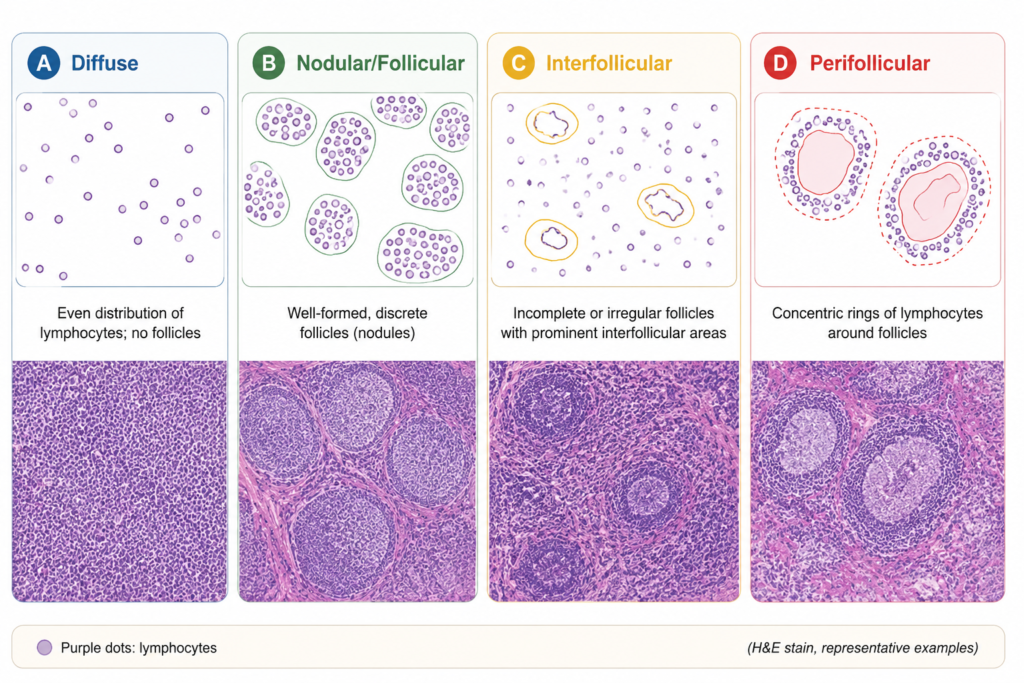
Morphology Pattern
Morphology Cytology: B Cell Lineage Based On Immunophenotype
| Small cells |
| Chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) Mantle cell lymphoma (MCL) Splenic marginal zone lymphoma (SMZL) Hairy cell leukemia (HCL) Lymphoplasmacytic lymphoma (LPL) Extranodal marginal zone lymphoma (EMZL) Nodal marginal zone lymphoma (NMZL) Follicular lymphoma (FL) Pediatric-type follicular lymphoma (PTFL) |
| Medium-sized cells |
| Burkitt lymphoma (BL) MCL, blastoid variant High-grade B-cell lymphoma (HGBL), NOS HGBL with MYC and BCL2 rearrangements (ICC and WHO-5) HGBL with MYC and BCL6 rearrangements (ICC) LBCL with 11q aberration [ICC]; HGBL with 11q aberrations [WHO] |
| Large cells ± anaplastic morphology |
| Diffuse large B-cell lymphoma (DLBCL), NOS GCB subtype Non-GCB subtype T-cell/histiocyte-rich large B-cell lymphoma (THRLBCL) Primary DLBCL of the CNS Primary cutaneous DLBCL, leg type EBV-positive DLBCL (EBV + DLBCL), NOS DLBCL associated with chronic inflammation Lymphomatoid granulomatosis Primary mediastinal large B-cell lymphoma (PMBL) Intravascular LBCL ALK-positive LBCL Plasmablastic lymphoma HHV8+ LBCL, NOS LBCL with IRF4 rearrangement Primary effusion lymphoma (PEL) Mediastinal gray zone lymphoma (MGZL) MCL, pleomorphic variant |
| Cutaneous localization |
| Primary cutaneous marginal zone lymphoma (PCMZL) Primary cutaneous follicle center lymphoma (PCFCL) Primary cutaneous DLBCL, leg type (PC-DLBCL, leg type) |
Lymphoid Cells
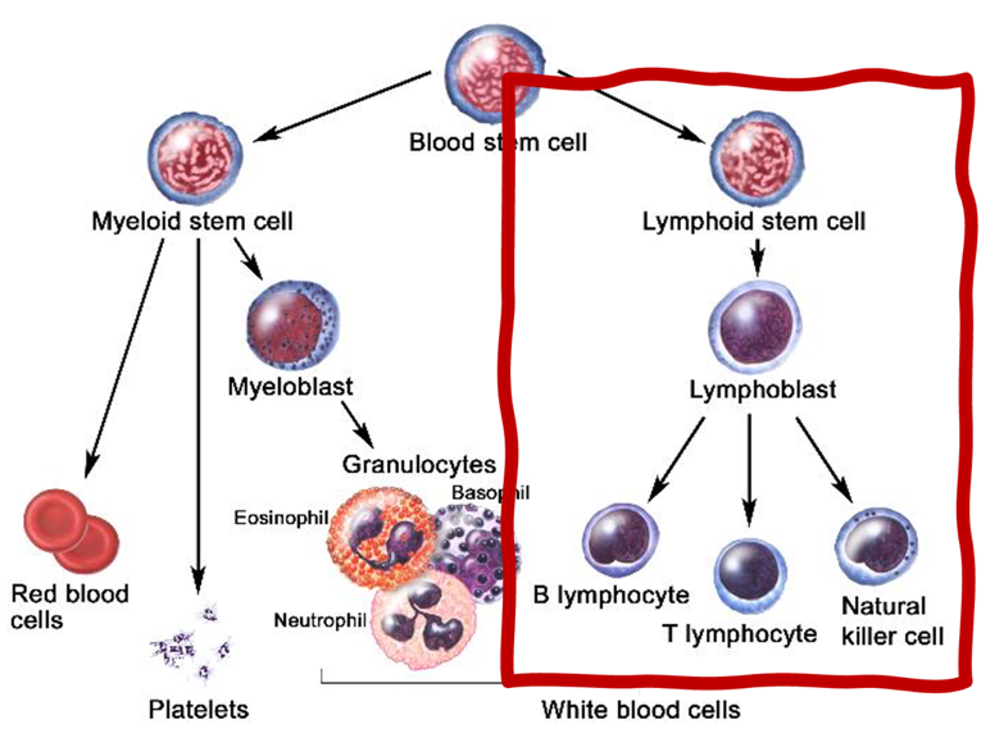
| B cells | Humoral immunity. Originates from stem cells in bone marrow and matures in the Bone marrow. Migrate to peripheral lymphoid tissue (follicles of lymph nodes, white pulp of spleen, unencapsulated lymphoid tissue). Recognize and present antigen. B cells differentiate into plasma cells (which produce antibodies and secrete specific immunoglobulins) and memory B cells (persist and accelerate future response to antigen). Can function as an APC. |
| T cells | Cell-mediated immunity. Originates from stem cells in bone marrow but matures in Thymus. Helper T-cells (Tc): CD4+ T cells help B cells make antibodies and produce cytokines to recruit phagocytes and activate other leukocytes. Cytotoxic T cells (Th): CD8+ T cells directly kill virus-infected and tumor cells via perforin and granzymes (similar to NK cells). Rule of 8: MHC II × CD4 = 8; MHC I × CD8 = 8. Delayed cell-mediated hypersensitivity (type IV). Acute and chronic cellular organ rejection. CD28 (costimulatory signal) necessary for T-cell activation. Most circulating lymphocytes are T cells (80%). |
| Natural killer (NK) cells | Lymphocyte member of innate immune system. Use perforin and granzymes to induce apoptosis of virally infected cells and tumor cells. Activity enhanced by IL-2, IL-12, IFN-α, and IFN-β. Induced to kill when exposed to a nonspecific activation signal on target cell and/or to an absence of MHC I on target cell surface. Also kills via antibody-dependent cell-mediated cytotoxicity (CD16 binds Fc region of bound IgG, activating the NK cell). |
B-cell Maturation
B-cell development stages:
- Pro-B cell (TdT, CD34, CD19, CD10, CD38): earliest stage in bone marrow (no surface Ig yet)
- Pre-B cell (TdT, CD19, CD10, ↓CD20, CD38, ↓CD138): rearranged heavy chain in the cytoplasm (Cμ; no surface light chain yet)
- Immature B cell (CD19, ↓CD10, CD20, ↓CD22, CD38, IgM): surface IgM with either κ or λ light chain
- Mature naïve B cell (CD19, CD20, CD22, IgM/IgD): expresses surface IgM and IgD, can circulate and enter lymphoid tissues
- Activated B cell (CD19, CD10, CD20, CD22, ↓CD27, CD38, ↓CD138): produce different Ig types (IgG, IgA…) per antigen expressed
- Memory B cell (CD19, CD20, ↓CD22, CD27): long-lived; rapidly reactivates upon re-exposure to the same antigen.
- Plasma cell (CD19 (if long-lived), CD38, CD138, CD27): Ab-secreting, short-lived in circulation, long-lived in bone marrow niches.
Mature B-cell lymphomas (BL, DLBCL, FL, MCL) originate after the immature B-cell stage; they already have a surface BCR (with κ/λ). Immature B-cell malignancies (B-lymphoblastic lymphoma/leukemia) usually lack surface light chains; they have cytoplasmic μ instead. If all the B cells in a sample have only κ or only λ light chains on their surface (instead of a normal κ:λ mix of ~2:1), that strongly suggests they’re all copies of one original malignant B cell (clonal lymphoma) and is not a reactive inflammation (polyclonal κ:λ ~2:1).
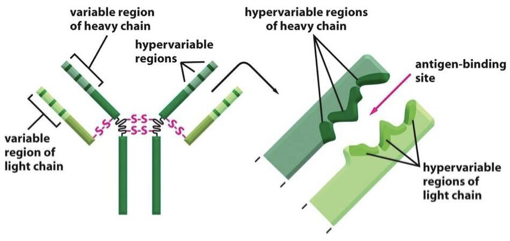
Sequence of gene rearrangements for BCR (heavy chain first [μ, δ, γ, α, ε] → light chain next [κ, λ] → class switching later [Ig]).
B-cell activation and class switching
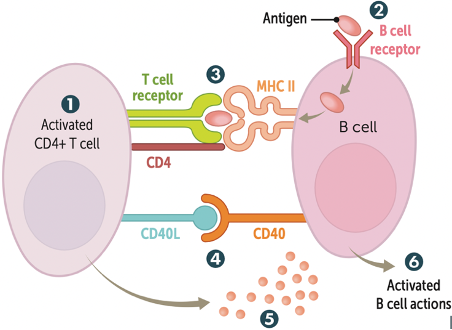
- Th-cell activation as on the left.
- B-cell receptor–mediated endocytosis.
- Exogenous antigen is presented on MHC II and recognized by TCR on Th cell.
- CD40 receptor (B cell) binds CD40 ligand (CD40L) on Th cell.
- Th cells secrete cytokines to determine Ig class switching of B cells.
- B cells are activated, undergo class switching and affinity maturation, and begin producing antibodies.
LYMPH NODE ANATOMY AND LYMPHOMA
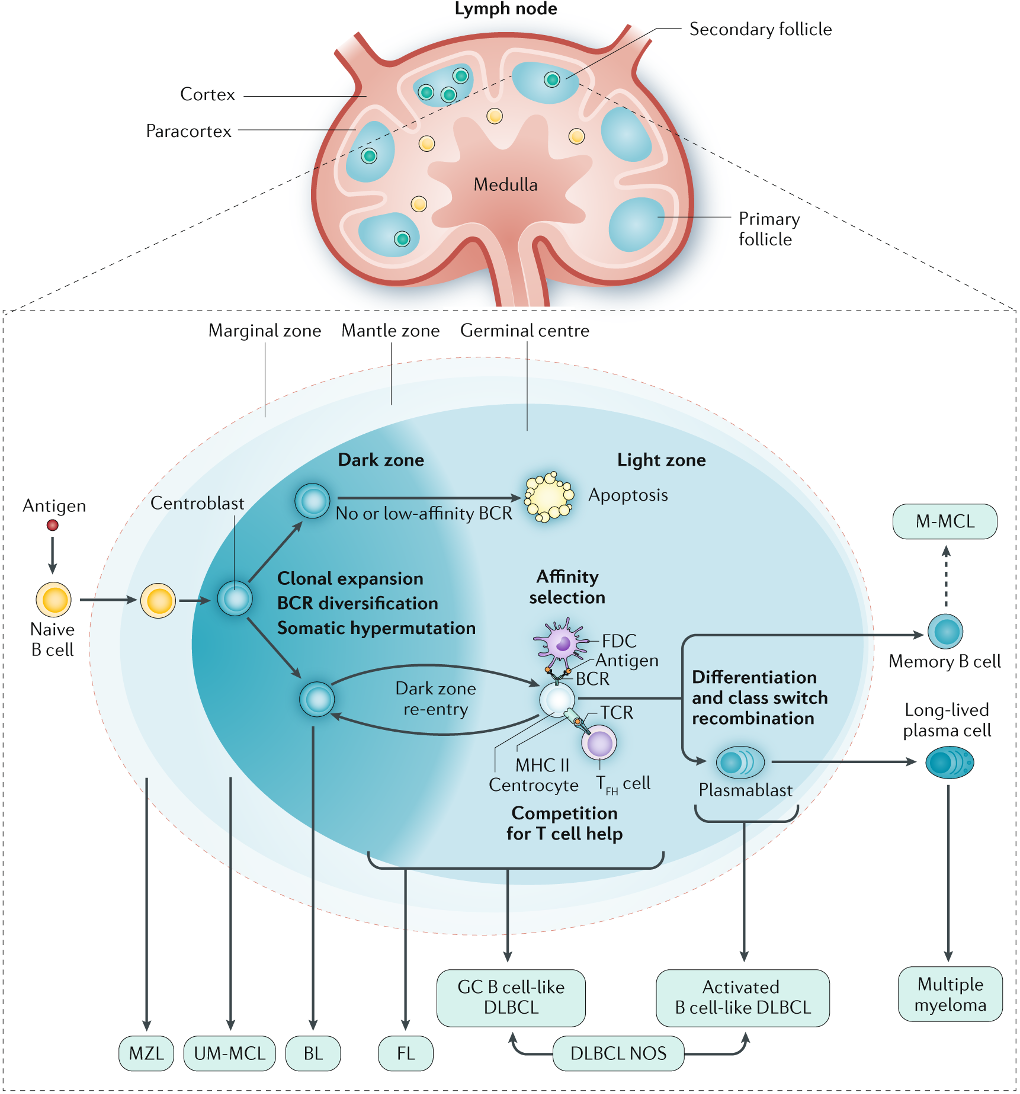
| Zone | Normal Function | Common Lymphoma | Immunophenotype/ Genetics | Treatment & Prognostic Relevance |
|---|---|---|---|---|
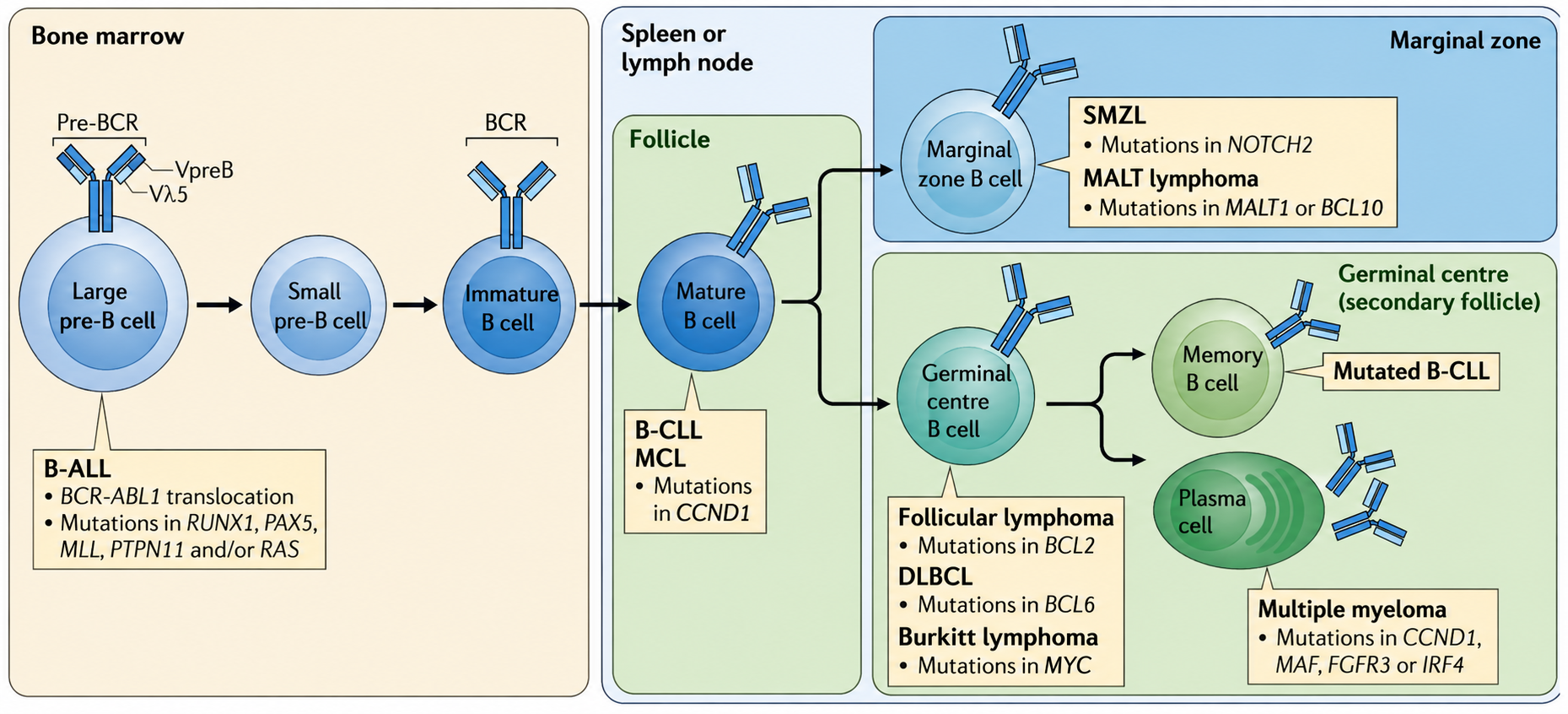
| Marginal Zone | First antigen-sampling area; contains memory B cells and antigen-presenting macrophages/dendritic cells. | MZL: extranodal (MALT), nodal, splenic types. | CD20+, CD79a+, CD5–, CD10–; t(11;18) in gastric MALT; chronic antigen stimulation link (H. pylori). | Eradication of H. pylori in gastric MALT may induce remission; rituximab-based regimens for systemic disease. Usually indolent but can transform. |
| Mantle Zone | Ring of resting naïve B cells; “reserve pool” for activation. | MCL (aggressive) | Cyclin D1 overexpression from t(11;14); CD5+, CD20+, SOX11+. | Not curable with R-CHOP alone; BTKi (ibrutinib, acalabrutinib) used in R/R disease. |
| Germinal Center (Dark Zone) | Rapid B-cell proliferation (centroblasts), somatic hypermutation. | BL, FL, GCB-DLBCL | CD10+, BCL6+; BL = MYC translocation; FL = BCL2 rearrangement (t(14;18)). | Germinal center–derived DLBCL has better prognosis with R-CHOP vs ABC subtype; certain translocations (high-grade lymphoma category). |
| Germinal Center (Light Zone) | Selection of B cells (centrocytes) for high-affinity antigen receptors; interaction with FDC and Tfh cells. | BL, FL, GCB-DLBCL; germinal center lymphomas; centrocyte predominance in low-grade FL. | FL grading per number of centroblasts/HPF. | Low-grade FL often “watch and wait” unless symptomatic; high-grade treated more aggressively. |
Marginal Zone (outermost layer of the follicle)
- Cell type: Mainly memory B cells, antigen-presenting macrophages and dendritic cells.
- Function: First area for antigens arriving in the lymph node. Antigen sampling from subcapsular sinus macrophages.
- Pathology: MZL originate here (extranodal, nodal, splenic); associated with chronic antigen stimulation (infection, autoimmune).
Mantle Zone (between marginal zone and germinal center)
- Cell type: Resting naïve B cells (small, mature).
- Function: Reservoir of non-activated B cells. These B cells can be recruited into the germinal center upon antigen stimulation.
- Pathology: MCL originates here (aggressive). Overexpression of cyclin D1 due to t(11;14).
Germinal Center (center of the follicle)
- Forms only in secondary follicles. Its function is antigen-driven B-cell maturation. FL, BL, and GCB-DLBCL originates here.
- Dark Zone: centroblasts proliferate (make huge army of B cells with same antibody), somatic hypermutation (introduces random point mutations in the variable (V) region of the Ig heavy/light chain genes via Activation-Induced cytidine Deaminase (AID), which affects the antibodies affinity to the FDC antigens and its selection in light zone)
- Light Zone: centrocytes undergo selection for high-affinity receptors).
Primary Follicle And Secondary Follicle
| Feature | Primary Follicle | Secondary Follicle |
| State | Resting/naïve B-cell cluster | Activated B-cell response |
| Cell type | Naïve small B lymphocytes | Proliferating & maturing B cells (centroblasts/centrocytes) |
| Function | Antigen surveillance | B-cell proliferation, selection, differentiation |
| Germinal center | Absent (+Marginal and Mantle zones) | Present (+Marginal and Mantle zones) |
Primary to secondary follicle
- Primary follicle: Cluster of naïve B cells in the outer cortex.
- When an antigen is presented to B cells (usually via follicular dendritic cells (FDCs) or subcapsular sinus macrophages), helper T cells (Tfh) enter the follicle through the T–B border.
- Tfh provide co-stimulation (e.g., CD40–CD40L, cytokines like IL-4, IL-21), activating the B cells.
- Activated B cells proliferate → follicle transforms into a secondary follicle with a germinal center.
- One germinal center ≈ one antigen-specific B-cell army.
Secondary follicle is temporary. Once the immune response ends:
- Germinal center shrinks.
- B cells either differentiate into plasma cells or memory B cells and leave, or undergo apoptosis if they fail selection.
- The follicle reverts to a primary follicle (or disappears entirely until reactivated).
- Why reversion happens: Antigen is cleared → no ongoing B-cell stimulation → germinal center collapses.
Germinal center (Dark zone vs. light zone)
Dark Zone
- Cells: Mainly centroblasts (large, activated, rapidly dividing B cells).
- Function: Intense proliferation. Somatic hypermutation of immunoglobulin genes (to tweak antibody affinity).
- “Dark” appearance: Packed, large nuclei and dense chromatin (stains darker histologically).
- Proliferation rate (highest in dark zone): This is the B-cell “breeding ground”.
Light Zone
- Cells: Mostly centrocytes (smaller, non-dividing B cells derived from centroblasts), plus FDCs and Tfh.
- Function:
- Selection: Centrocytes test their mutated B-cell receptors against antigen displayed on FDCs.
- Help from Tfh: Those with high-affinity receptors receive survival signals; low-affinity or autoreactive cells undergo apoptosis.
- “Light” appearance: Looser cell packing, more cytoplasm, and presence of FDC processes → stains lighter.
| Feature | Centroblast (Dark Zone) | Centrocyte (Light Zone) |
| Size | Large | Smaller |
| Proliferation | High | Low |
| Function | Centroblast proliferation, somatic hypermutation, clonal expansion | Antigen testing, selection |
| Surface Ig | Low/absent (internal rearrangement ongoing) | Present (mutated Ig for antigen testing) |
Germinal Center–Derived vs. Post–Germinal Center B-cell Lymphomas
When a B cell becomes malignant, the stage of its development in the normal immune response can be traced from its immunophenotype and gene expression profile.
Germinal center–derived = the cancer cell looks genetically and phenotypically like a normal B cell in the germinal center (secondary follicle stage).
GCB subtype (germinal center B-cell–like)
- Derived from B cells in the germinal center.
- Better prognosis with standard R-CHOP therapy.
- Often has genetic features like BCL6 expression, t(14;18) BCL2 rearrangement.
Post–germinal center (also called activated B-cell–like): the cancer cell has already passed through the germinal center stage and has begun differentiating into plasma cells or memory B cells.
ABC subtype (activated B-cell–like, post–germinal center)
- Derived from B cells that have exited the germinal center.
- Worse prognosis with R-CHOP.
- Often has NF-κB pathway activation (e.g., MYD88 mutations).
- May respond better to targeted agents (e.g., ibrutinib in trials).