Only 20-30% of patients with identified infectious source; ~80% of FN from endogenous flora. Micro-organisms involved are bacteria (GNB 40%, GPC 60%, rarely anaerobes), fungal (rare, common in high risk, candida and aspergillus), viral (community-acquired).
Definitions
- Febrile: Temp ≥38.3 C (101 F) once or ≥38 C (100.4 F) over 1h
- Causes: infection, immune system coming back with more WBC, chemotherapy releasing inflammatory markers (histamine), cancer
- Neutropenia: ANC<500 cells/mm3 or <1000 cells/mm3 and a predicted decline to ≤500 over next 48h.
- Nadir: lowest ANC levels. Usually happens at day 7-14, recovers by day 21
- Profound neutropenia: ANC<100 (or ANC 0). APC can be used in ANC 0 (shows early sign of bone marrow recovery)
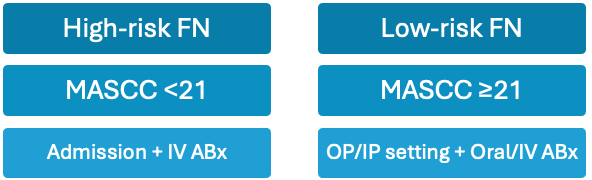
Risk Tools (MASCC Scores)
| Prognostic Factor | Weight |
| Burden of illness No or mild symptoms Moderate symptoms | 5 3 |
| No hypotension (SBP >90 mmHg) | 5 |
| No chronic obstructive pulmonary disease Solid tumor or no previous fungal infection | 4 4 |
| No dehydration requiring parenteral fluids Outpatient status | 3 3 |
| Age <60 years | 2 |
Work-Up
- H&P: comorbidities/meds, time since last chemo, recent ABx, tobacco/alcohol use, infection from household, drug allergy, clinical instability
- Lab (CBC, EMP, LFTs, renal), chest X-ray
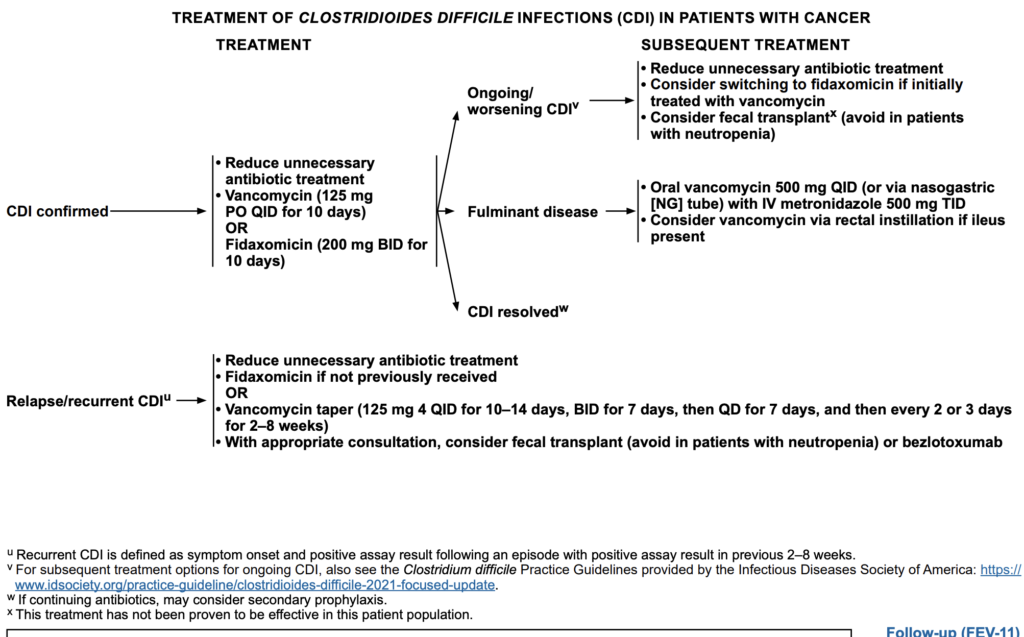
- ID: site of infection, culture (blood x2, urine [if urinary catheter, abnormal UA] stool [diarrhea C.diff/enteric], skin [aspirate/biopsy]), UA, consider fungal/mycobacteria if vascular access, PCR/DFA (viral) – expect ESBL, VRE, MRSA, Pseudomonas
Management
Goal: avoid bloodstream infection, avoid delay/reduction of the dose.
Clinical Pearls
- Choice of ABx depends on high/low risk FN, causative micro-organism, site, source, local antibiogram and organ dysfunction.
- ↑ neutropenia = ↑ duration of antibiotic = ↑ fungal infection risk. Can start antibiotic in suspected/expected neutropenia for >7 days.
- Empiric IV broad-spectrum: cefepime, carbapenems, piperacillin-tazobactam. Adjust in 3-5 days based on cultures.
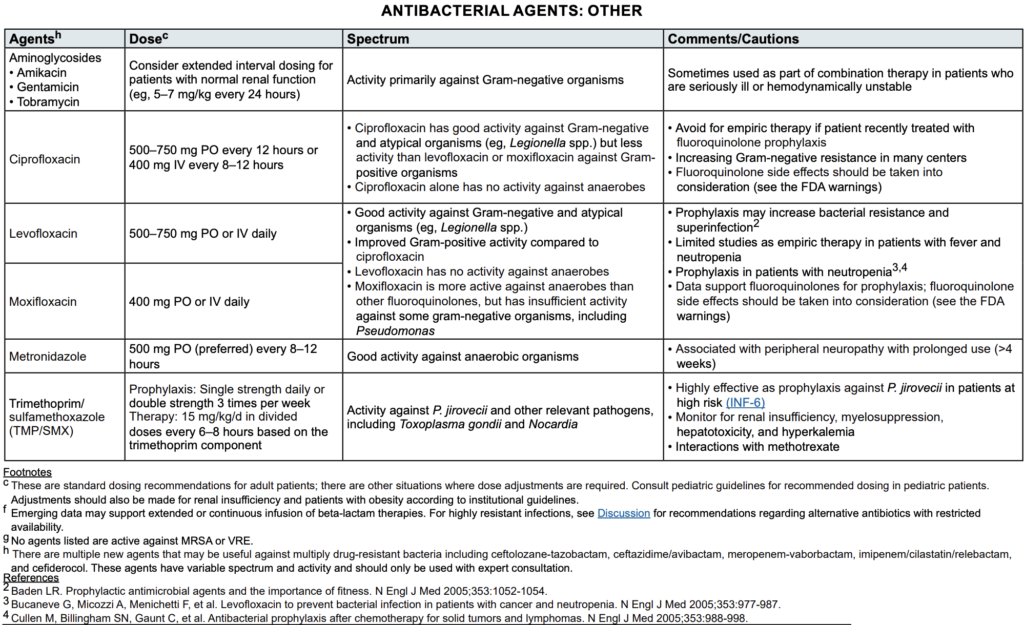
- Oral antibiotics: fluoroquinolones or sulfamethoxazole/trimethoprim
Empiric IV Abx in high risk FN
- High risk definition: acute leukemias (ALL), strong chemo. Most peds are high risk, and mostly are already on Abx compared to adults
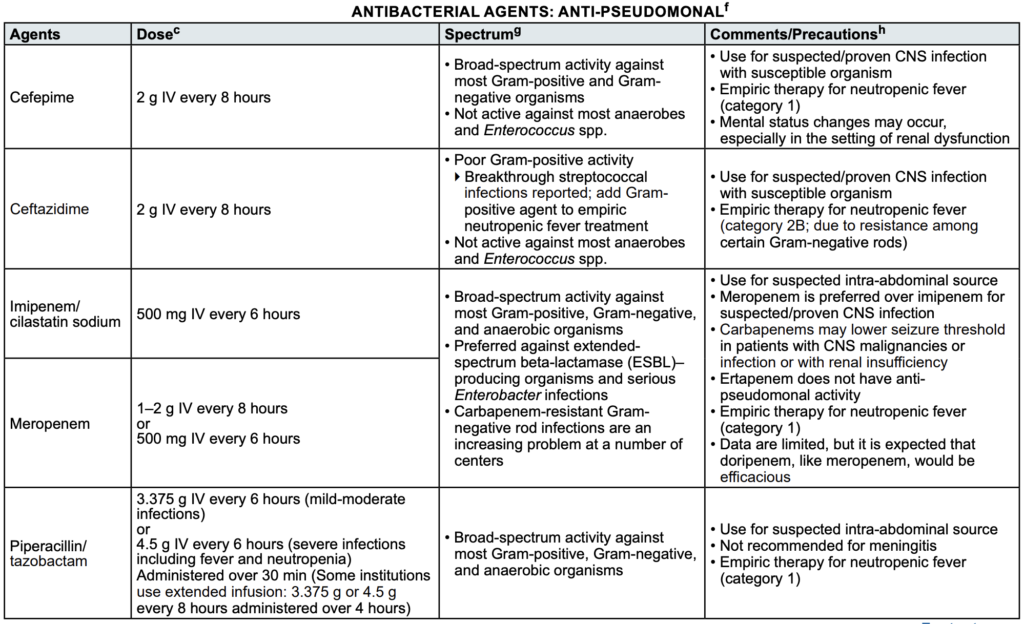
- Anti-pseudomonal: β-lactams (cefepime, pip/tazo), carbapenems (mero, imi/cila), ceftazidime (weak GPC, high breakthrough infection).
- Clindamycin (pen/ceph allergy, cheaper, more GPC coverage, mutliple capsules per day and PO suspension tastes bad)
- Aztreonam (pen/ceph allergic/anaphylaxis, $$$)
- Reserve second GN ABx or vanco (MRSA history, SSTI, catheter) for hemodynamically unstable, high resistance suspicion/antibiogram.
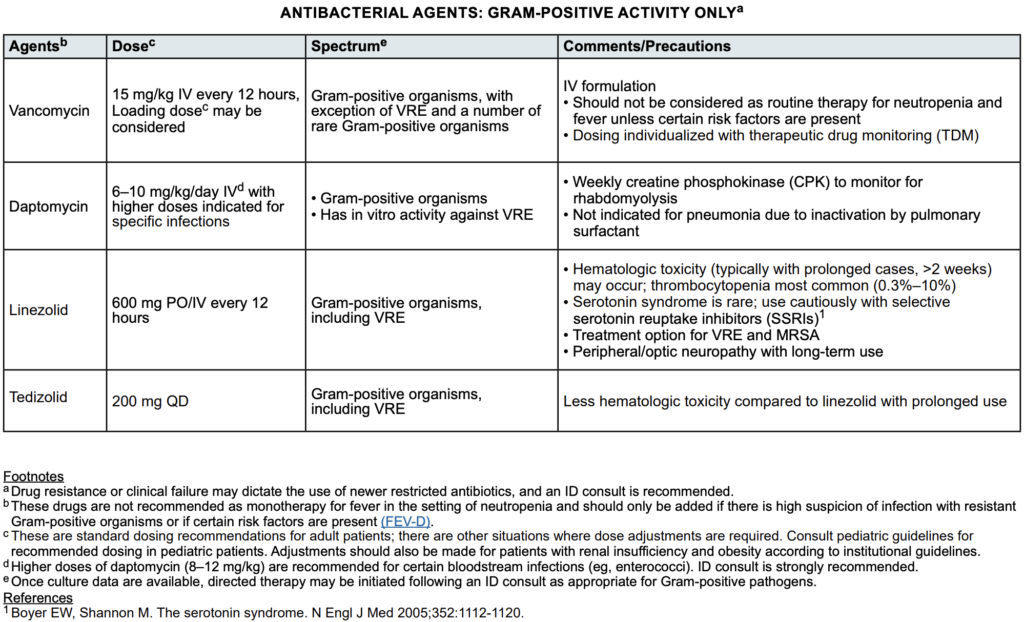
- GPC (MRSA): vancomycin, daptomycin (not pneumonia, deactivated by lung surfactant), linezolid, ceftaroline (pneumonia)
- Re-assess in 2-3 days and consider D/C
Outpatient PO Abx in low risk FN
- Low-risk definition: palliative treatment, non-traditional chemo; can be seen in adults. Rarely seen in peds.
- Consider palatability, cooperation (in peds), drug availability (as PO liquid for peds), mucositis, able to swallow, no N/V, not on FQ ppx
- Meds: Ciprofloxacin + amoxicillin/clavulanic acid, Levofloxacin, or Moxifloxacin (no pseudomonal coverage)
- Return to clinic if any positive culture, new signs and symptoms, persistent/recurrent 3-5 days, oral intolerance, IV infusion antibiotic
Monitoring Daily
Clinically stable or improving; fever decreasing or persistent; otherwise clinically stable:
- No change in empiric regimen. Fever could be from bone marrow recovery (increasing WBC), cancer, chemo (histamine).
- Continue at least until ANC ≥500 cells/mcL and increasing
- Modify regimen based on new clinical or microbiologic data
Not responding/clinically worsening; persistently febrile; persistently bacteremic:
- ID consult; broaden coverage based on clinical and microbiologic data to include other organisms not covered by empiric regimen
- Consider imaging studies and further microbiological testing
- Consider adding G-CSF
Fever ≥4 days: add mold active anti-fungal
Discontinuation
- D/C if all applies: afebrile ≥24h , negative blood cx >48h, bone marrow recovery (ANC >100 or trending up). Continue antibiotic; no matter the duration; until ANC>100
- Low risk (not in peds): D/C at 72h if afebrile ≥24h and negative blood culture
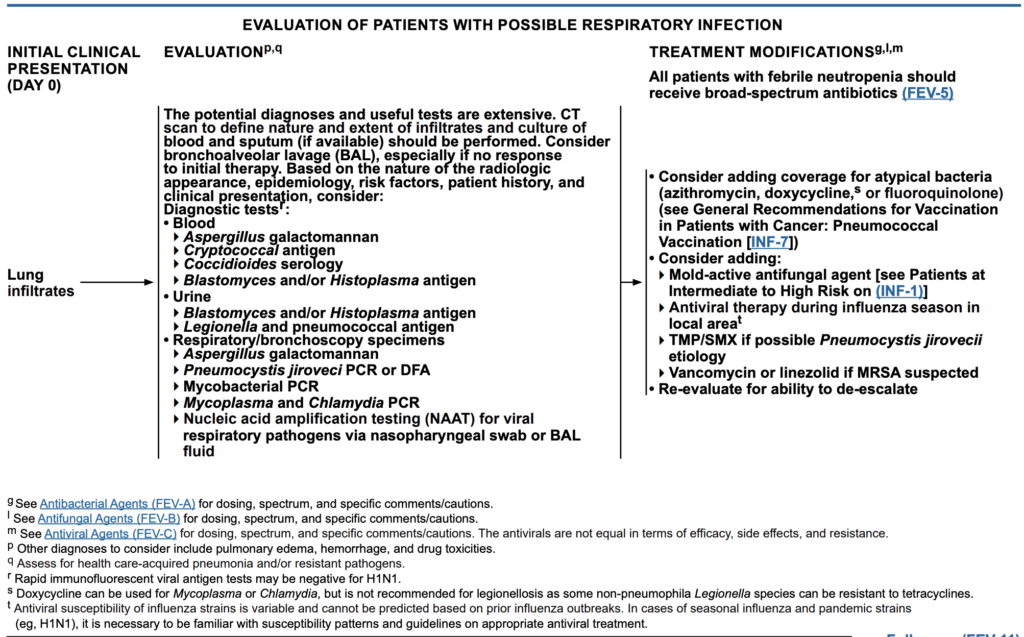
Fungal infection
- High risk: AML, high-risk ALL, relapsed acute leukemias, BMT, prolonged neutropenia, prolonged corticosteroids
- Suspect fungal infxn if prolonged fever ≥96h (4 days) while on broad-spectrum ABx
- BD-glucan testing results takes time (not routinely done in pediatrics), therefore antifungal is started unless BD-glucan testing is indicated.
| Antifungal Agent | Place in Therapy | Dose | Clinical Pearls |
| Amphotericin B | Broad spectrum (Candida, Aspergillus spp. (excluding A. terreus), Mucorales, rarer molds, C. neoformans, and dimorphic fungi) | AmB-D (per indication): 0.5–1.5 mg/kg IV daily ABLC: 5 mg/kg IV daily L-AMB: 3–5 mg/kg IV daily | ADE: nephrotoxic (saline loading), e- wasting, infusion reaction (antipyretics, antihistamine, meperidine (for rigors); slower rate) Lipisomal: Less infusion rxn, renal toxic Avoid in Scedosporium, Lomentospora |
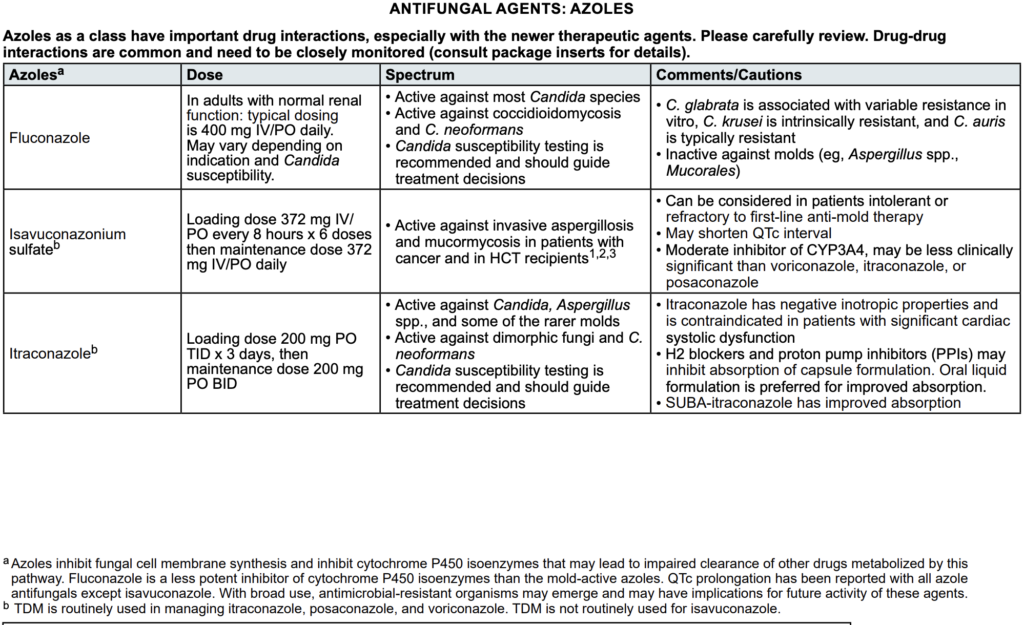
| Fluconazole IV/PO | Most BMT on fluconazole, not routinely used; candida | 400 mg IV/PO daily (renal adjustment) | DDI. Avoid in C. glabrata/krusei/auris, Aspergillus spp., Mucorales |
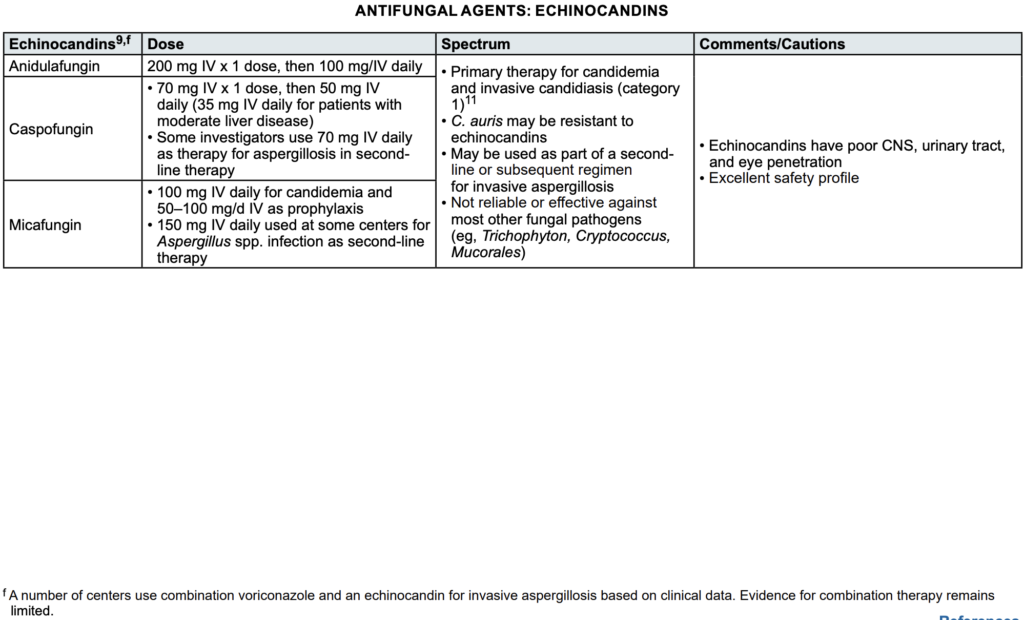
| Caspofungin IV | Candida, inpatient; invasive aspergillosis (2nd line, subsequent); refractory fluconazole | LD 70 mg, then 50 mg daily (35 mg daily in mod liver disease) Aspergillosis (2nd line, some institutes): 70 mg daily | ADE: tolerable. Poor CNS, urinary, eye penetration Avoid in C.auris, Trichophyton, Cryptococcus, Mucorales |
| Micafungin IV | Candida, outpatient; invasive aspergillosis (2nd line, subsequent) | Treatment: 100 mg daily Ppx: 50-100 mg daily Aspergillus (2nd line, some institutes): 150 mg IV daily | Tolerable ADE (poor CNS, urinary, eye penetration) Avoid in C.auris, Trichophyton, Cryptococcus, Mucorales |
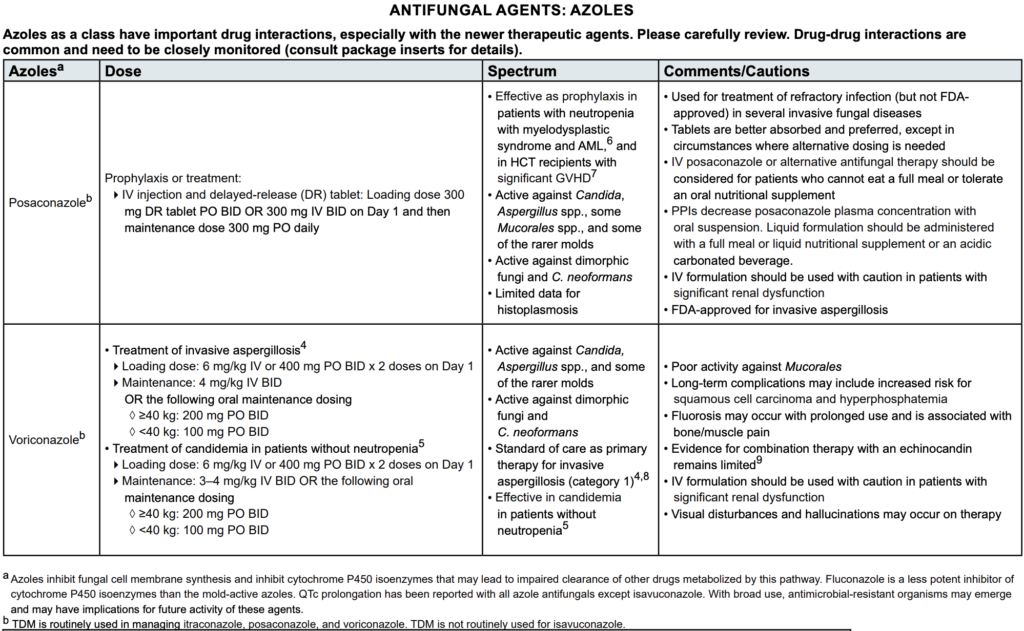
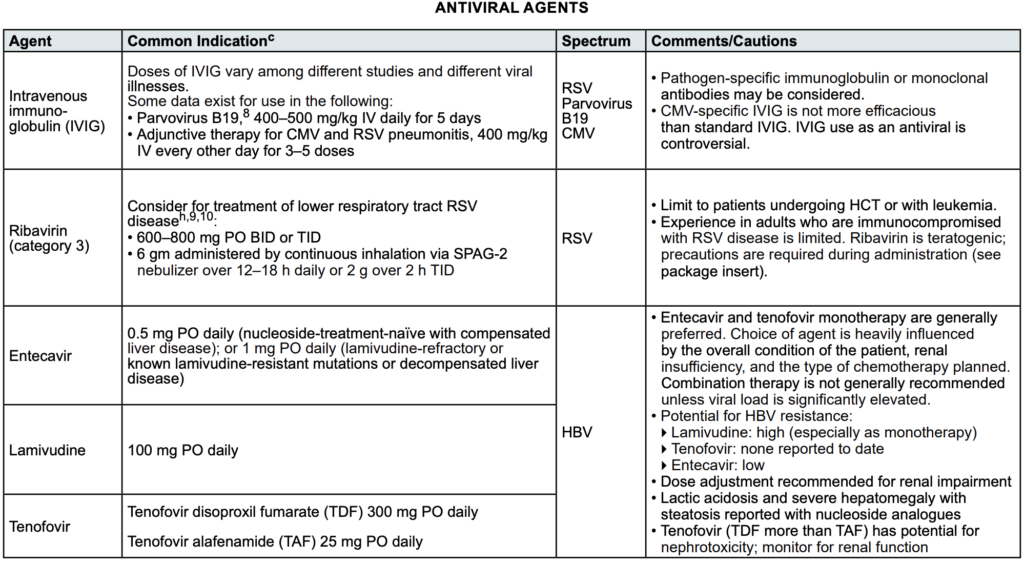
| Posaconazole IV/ PO DR | PPx (neutropenia with MDS and AML; HSCT significant GvHD) Refractory infection, candida, invasive aspergillus, some mucorales, some rarer molds, dimorphic fungi, C. neoformans | Treatment/ppx: LD 300mg BID x1d IV/PO then 300mg daily (Renal adjustments) | Better absorption with tablets IV who is oral intolerable DDI: PPIs |
| Voriconazole | Invasive Aspergillus, candida, rare molds, dimorphic fungi, C. neoformans; refractory fluconazole | Treatment of invasive aspergillosis LD 6 mg/kg IV or 400 mg PO BID x 2 doses on Day 1 MD 4 mg/kg IV BID, or 200mg (≥40kg), 100mg PO BID (<40kg) Treatment of candidemia in patients without neutropenia LD 6 mg/kg IV or 400 mg PO BID x 2 doses on Day 1 MD 3–4 mg/kg IV BID, or 200mg (≥40kg) or 100mg (<40kg) PO BID | Poor activity against Mucorales ADE: SCC risk, high phos, fluorosis, bone/muscle pain, visual disturbances, hallucinations Evidence for combination therapy with an echinocandin remains limited IV formulation should be used with caution in patients with significant renal dysfunction |
| TMP/SMX | Pneumocystis jirovicii, Toxoplasma gondii and Nocardia | Prophylaxis: SS daily or DS TIW Therapy: 15 mg/kg/d in divided doses q6–8 hours per TMP | Monitor for renal insufficiency, high K, myelosuppression, hepatotoxicity DDI: methotrexate |
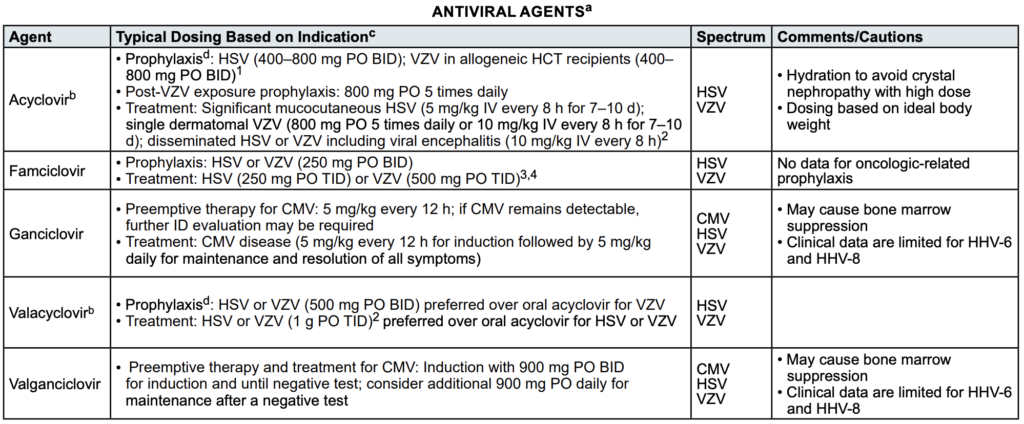
Viral infection
| Antiviral Agent | Place in Therapy | Dose | Clinical Pearls |
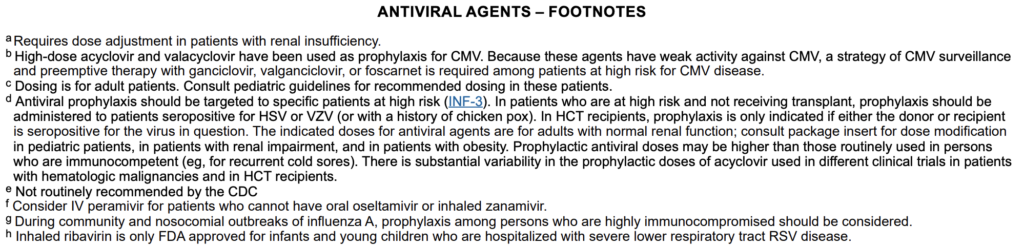
| Acyclovir | HSV, VZV | Prophylaxis: HSV (400–800 mg PO BID); VZV in alloHCT (400–800 mg PO BID)1 Post-VZV exposure ppx: 800 mg PO x5/d Significant mucocutaneous HSV: 5 mg/kg IV q8h x7–10 d Single dermatomal VZV: 800 mg PO x5/d or 10 mg/kg IV q8h x7–10d Disseminated HSV/VZV + viral encephalitis: 10 mg/kg IV q8h | Hydration to avoid crystal nephropathy with high dose Dosing based on IBW |
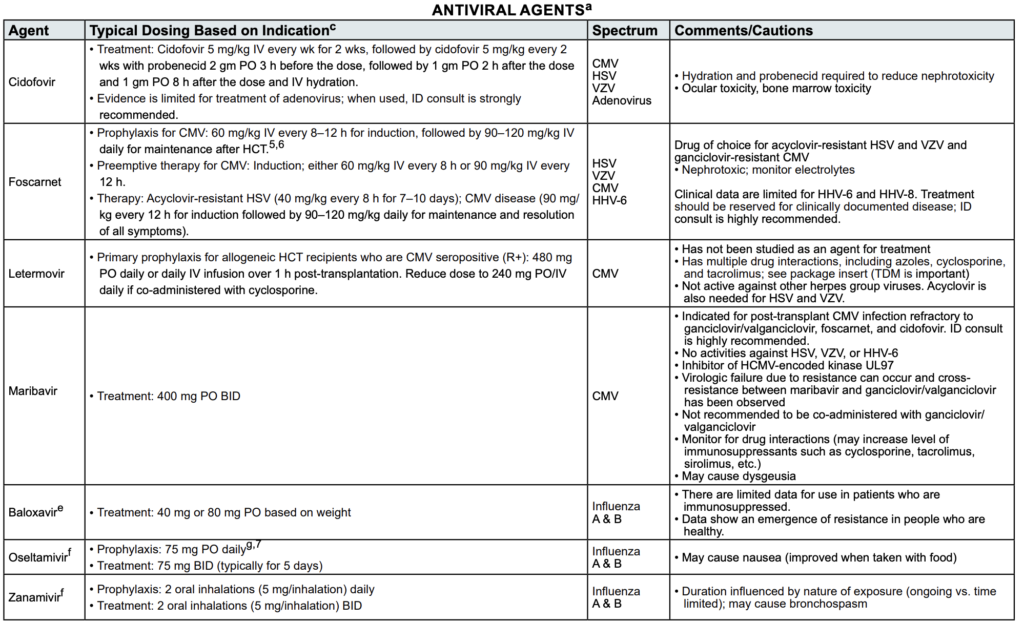
| Ganciclovir | CMV, HSV, VZV | Preemptive therapy for CMV: 5 mg/kg q12h; if CMV remains detectable, further ID evaluation may be required Treatment: CMV disease (5 mg/kg q12h for induction f/b 5 mg/kg/day for maintenance and resolution of all symptoms) | ADE: myelosuppression Clinical data are limited for HHV-6/8 |
| Valganciclovir | CMV, HSV, VZV | Preemptive therapy and treatment for CMV: Induction with 900 mg PO BID until negative test; consider additional 900 mg PO daily for maintenance after a negative test | ADE: myelosuppression Clinical data are limited for HHV-6/8 |
Duration of therapy
| Skin/soft tissue | 5-14 days |
| Bacterial sinusitis | 7-14 days |
| Bacterial pneumonia | 5-14 days |
| Gram-negative bacteremia Gram-positive bacteremia S. aureus bacteremia Yeast bacteremia Catheter bacteremia | 7-14 days 7-14 days 4 weeks after first negative blood culture; ID consult ≥2 weeks after first negative blood culture Catheter removal for Candida or other yeasts, S. aureus, P.aeruginosa, Corynebacterium jeikeium, Acinetobacter spp., nontuberculous mycobacteria, molds, VRE, Steno. maltophilia, and other MDROs |
| Candida Mold | ≥2 weeks after first negative blood culture ≥ 12 weeks |
| HSV/VZV Influenza A | 7-10 days (uncomplicated localized disease to skin; acyclovir, valacyclovir, famciclovir) ≥ 5 days of oseltamivir |
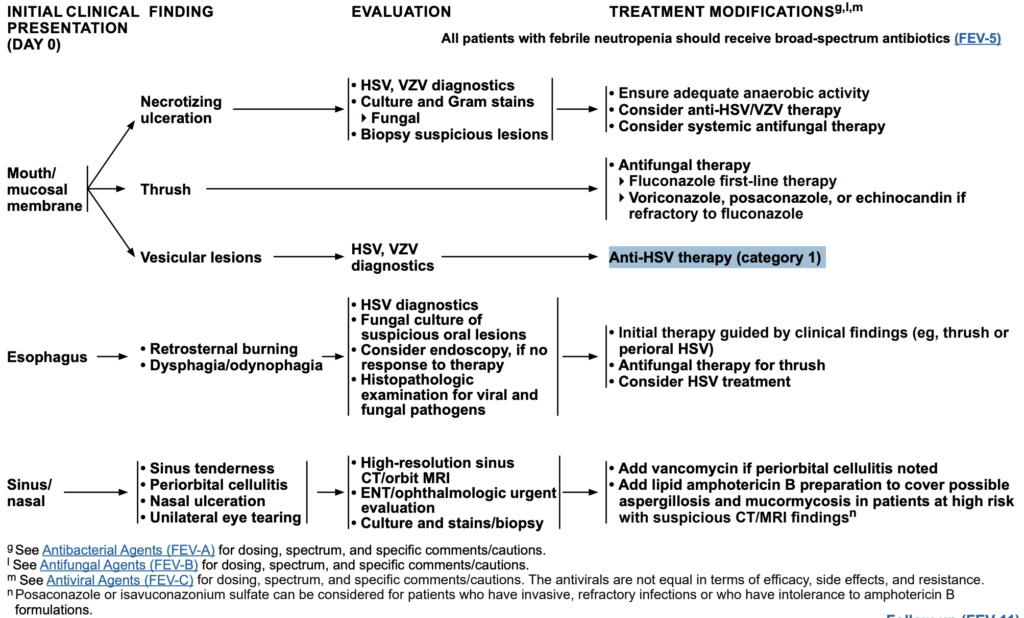
Other Cancer-Related Infections
| Finding | Evaluation | Management |
| Mouth/mucosal Necrotizing ulceration | • HSV, VZV diagnostics • Culture and Gram stains; Fungal • Biopsy suspicious lesions | • Ensure adequate anaerobic activity • Consider anti-HSV/VZV therapy • Consider systemic antifungal therapy |
| Mouth/mucosal Thrush | • Fluconazole first-line therapy • Voriconazole, posaconazole, echinocandin (if fluconazole refractory) | |
| Mouth/mucosal Vesicular lesions | HSV, VZV diagnostics | Anti-HSV therapy (category 1) |
Medications
Antibactieral Agents (Gram-Positive Activity)
| Agents | Spectrum | Dose, ADE, Clinical Pearls |
Antibactieral Agents (Gram-Pseudomonal Activity)
| Agents | Spectrum | Dose, ADE, Clinical Pearls |
Antibactieral Agents (Other Activity)
| Agents | Spectrum | Dose, ADE, Clinical Pearls |
Antifungal Agents (Azoles)
| Agents | Spectrum | Dose, ADE, Clinical Pearls |
Antifungal Agents (Amphotericin B)
| Agents | Spectrum | Dose, ADE, Clinical Pearls |
Antifungal Agents (Echinocandins)
| Agents | Spectrum | Dose, ADE, Clinical Pearls |
Antiviral Agents
| Agents | Spectrum | Dose, ADE, Clinical Pearls |
Febrile Neutropenia Prophylaxis (Prevention is the Key)
NCCN Hematopoietic Growth Factors – Version 3.2026 – December 5, 2025
Prevention interventions: G-CSF prophylaxis, antimicrobial prophylaxis, vaccinations
Granulocyte Colony Stimulating Factor (G-CSF) Prophylaxis
Primary prophylaxis (prevent neutropenia/FN with first cycle of chemotherapy)
- High risk of FN (>20%): give G-CSF prophylaxis (category 1)
- Anticancer therapy: NHL (BV-CHP, DA-EPOCH, HyperCVAD, dd-CHOP-14, Pola-R-CHOP, DHAP, ESHAP, ICE, MINE), HL (BV-AVD, eBEACOPP, BrECADD), MM (DT-PACE ± Bortezomib, DCEP, high-dose cyclophosphamide), ALL regimens, breast (dd-AC f/b dd-paclitaxel, TAC, TCH, TCH), bladder (dd-MVAC), RCC (doxo/gem), testicular (VeIP, VIP, TIP), SCLC (topotecan), ovarian (topotecan, docetaxel, TC), melanoma (CVD, PHP), bone (VAIA, VDC-IE, doxo/cis, VDC, VIDE), soft-tissue sarcoma (MAID, doxo, ifos/doxo), head/neck SCC (TPF)
- Other risk factors: poor performance status, HIV (low CD4 counts), chronic immunosuppression in post-txp (organ/stem cell txp)
| Prophylaxis | Treatment | Therapeutic in radiation-induced myelosuppression (H-ARS) |
| Pegfilgrastim (or biosimilars) Eflapegrastim-xnst Efbemalenograstim alfa-vuxw Filgrastim (in practice though not mentioned in NCCN) | (GF during FN; discontinued at time of ANC recovery) Filgrastim (or biosimilars) 5 mcg/kg tbo-filgrastim 5 mcg/kg Sargramostim 250 mcg/m2/day | Filgrastim (or biosimilars) tbo-filgrastim Pegfilgrastim (or biosimilars) Sargramostim Eflapegrastim-xnst Efbemalenograstim alfa-vuxw |
- Intermediate risk of FN (10-20%): consider G-CSF prophylaxis if ≥1 risk factors (prior chemo/RT, persistent neutropenia, bone marrow involvement, recent surgery ± open wounds, liver (bilirubin >2g/dL), renal (CrCl<50), age >65 on full chemo dose intensity)
- Examples: NHL (GDP, CHOP, CDOP, bendamustine), breast (docetaxel, AC, paclitaxel q21d, sacituzumab govitecan-hziy), prostate (Cabazitaxel, docetaxel), testicular (BEP, cis/etopo), SCLC (carbo/etopo), NSCLC (cis/pacli, cis/vinor, cis/docet, cis/etop, carbo/pacli, docetaxel), adenocarcinoma (gem/docetaxel), esophageal/gastric (iri/cis, FLOT), CRC (FOLFIRINOX), pancreatic (FOLFIRINOX), ovarian (carbo/doce, cis/etop), cervical (cis/topo, pacli/cisp, topo, iri), uterine sarcoma (docetaxel), occult (doc/gem)
- Low risk of FN (<10%): G-CSF is not recommended, may consider if ≥2 risk factor (prior chemo/RT, persistent neutropenia, bone marrow involvement, recent surgery ± open wounds, liver (bilirubin >2g/dL), renal (CrCl<50), age >65 on full chemo dose intensity)
Secondary prophylaxis (prevent recurrent neutropenias), consider adding G-CSFs on future cycles.
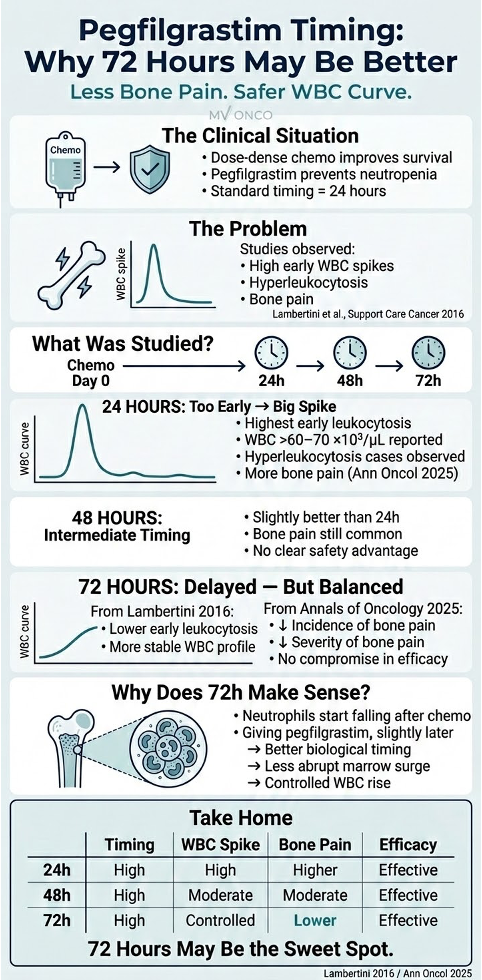
Timing of G-CSFs
| Agent | Timing |
| Filgrastim SC 5mcg/kg/day | Start 24-72h after chemo, give daily until post-nadir ANC recovery (~5–7 days; no study showed duration) |
| Pegfilgrastim SC 6mg once | Give once, ≥24h after chemo, not within 14 days of next chemo |
| tbo-filgrastim SC 5mcg/kg/day | Same as filgrastim timing and duration |
| Avoid G-CSFs during or within 24h of chemotherapy as the chemo cytotoxicity will kill more neutrophils; making G-CSFs ineffective. Avoid pegfilgrastim in weekly chemo regimens due to its long half-life (15-80h) as it overlaps the anticancer and pegfilgrastim effects. ANC: normal (≥1500–8000), mild neutropenia (1000-1499), moderate (500-999), severe (<500), agranulocytosis (<100) | |
Important information
- Consider dose reduction instead of CSF in palliative patients (not worth the ADE of G-CSF and cost).
- Risk of bleomycin-induced pulmonary toxicity/fibrosis may be increased with G-CSFs (conflicting data, some may give filgrastim same day, some doesn’t)
- ES-SCLC: Trilaciclib can be used as ppx before platinum/etoposide ± ICI or topotecan-regimens, to reduce chemo-induced myelosuppression
Granulocyte-CSFs
- Common ADE: bone pain (cetirizine (long-acting), loratadine (sedation, anticholinergic), diphenhydramine (sedation)], fever, headache; splenomegaly, hyperuricemia, rash, hypotension, leukocytosis, hypersensitivity to proteins produced by E.coli (filgrastim is made from E.coli)
| Medication | Dosing | Clinical Pearls |
| Filgrastim (Neupogen) (category 1) Biosimilars: Tbo-filgrastim (Granix) (category 1) Filgrastim-sndz (Zarxio) Filgrastim-aafi (Nivestym) | 5 mcg/kg/d SC (round to the vial size per institution) until post-nadir ANC recovery to normal or near-normal | tbo-filgrastim (not biosimilar): Higher fluid retention/fever vs. filgrastim Warnings: allergic reactions (rash, facial edema, wheezing, dyspnea, hypotension, tachycardia, anaphylaxis), splenic rupture, ARDS, alveolar hemorrhage/hemoptysis, sickle cell crises in SCD, MDS/AML with chronic use Precautions • Rare: vasculitis, sweet syndrome • Immunogenicity (with biosimilars) Clinical trials checked ANC daily to see the curve, but the goal is to prevent FN and not only ANC recovery. Shorter duration showed less efficacy |
| Pegfilgrastim (Neulasta) (category 1) Pegfilgrastim-jmdb (Fulphila) Pegfilgrastim-cbqv (Udenyca) Pegfilgrastim-bmez (Ziextenzo) Pegfilgrastim-apgf (Nyvepria) | 6mg SC once | PK: long half-life (15-80h) Can be used in Q3-week regimens (Category 1), Q2-week regimens (supported by Phase II trials), but not recommended in Q1-week regimens Neulasta On-pro: novel delivery device, auto-inject 27h after application. Preferred for outpatient setting. Watch for delivery failure with On-Pro Warning, Precautions, ADE same as filgrastim |
| Eflapegrastim-xnst (Rolvedon) | 13.2 mg SC daily | Administer ~24h after chemo. Do not give ~14 days before or 24h after chemo Newer long-acting G-CSF. Higher potency in some trials |
| Efbemalenograstim alfa-vuxw (Ryzneuta) | 20 mg SC once | Administer ~24h after chemo. Do not give ~14 days before or 24h after chemo Newest agent (FDA approved late 2022). Pegylated, long-acting |
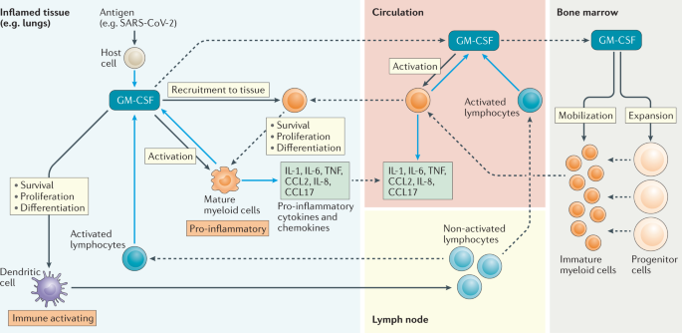
Granulocyte/macrophage-CSF (GM-CSF)
- Hematopoietic growth factor that stimulates the development and production of WBC (granulocytes, macrophages, monocytes). These effector cells help to mediate antibody-dependent cell mediated cytotoxicity (ADCC).
- The Fc fragment of the Dinutuximab mAb binds the Fc receptors on these effector cells, which in turn engulf the bound tumor cell and destroy it.
- ADE (from pro-inflammatory cytokine release like IL-1, IL-6, TNF-α): fever/chills, fatigue, malaise, bone pain/myalgias, headache, injection site reaction/rash, N/V, diarrhea, edema (peripheral, facial)
- Serious: capillary leak syndrome (hypotension, edema, hypoalbuminemia, hemoconcentration), pulmonary toxicity (dyspnea, pleural/pericardial effusion, pulmonary infiltrates; caution with bleomycin), hypersensitivity reactions (anaphylaxis, urticaria, angioedema), leukocytosis/thrombocytosis (may cause elevated WBCs and platelets; monitor CBC), arrhythmias/chest pain (especially in those with pre-existing cardiac conditions)
- Rare/Immune-mediated Effects: autoimmune-like syndromes (Sweet’s syndrome – acute febrile neutrophilic dermatosis), vasculitis, hearing loss (rare), renal dysfunction (rare cases of proteinuria, hematuria)
| Medication | Dosing | Clinical Pearls |
| Sargramostim (Leukine) | 250 mcg/m²/day SC or IV | Start 24–72h post-chemo and continue until ANC >1,500 x 2 daysNot routinely used for FN prophylaxis per NCCN (use G-CSFs instead). May improve recovery of monocytes/macrophages tooFDA indication: AML induction in older adults (to ↓infection duration), PBPCs mobilization, post-transplant recovery (bone marrow or stem cell) ADE: More inflammatory effects (vs filgrastim; fever, bone pain, fluid retention, capillary leak), diarrhea, nausea, first-dose effect (flushing, hypotension, dyspnea), pericardial/pleural effusion (rare). IV ADE differs from SCUsed with T-VEC (cancer vaccine) recruit immune cells (dendritic cells, macrophages, T-cells) to enhance anti-tumor response and kill cancers in melanoma (immunoambulization) COVID19 (see pic below) |
| Molgramostim | 5-10 mcg/kg/day SC (60k-110k 000 IU/kg) | Start 24h post-chemo and continue for 7-10 days.ADE: transient hypotension and flushing, bone/MSK pain, fever and chills, dyspnoea, rash, fatigue, GI effects; antibodies. Rare: anaphylactic reactions, pleural and pericardial effusion, cardiac arrhythmias. Fetotoxic in animal studiesPrecaution: myeloid malignancies, pulmonary disease |
Antibiotic Prophylaxis
- Goal: reduce rate of bacteremia, infxn, mortality
- Infection risk categories
- Low: solid tumor, neutropenia <7 days
- Intermediate: chronic leukemias, autoHSCT, lymphomas, MM, neutropenia 7-10 days
- High: acute leukemias, alloHSCT, neutropenia >10 days; ANC nadir <500 for ≥7 days
- Broad-spectrum antimicrobials: antibacterial (FQ: levofloxacin preferred), antifungal (azole, echinocandins), antiviral (HSV/VZV)
- Risk of antibiotic prophylaxis: C.diff, invasive fungal, Abx resistance
- Stop antibiotic prophylaxis if ANC ≥500
Vaccinations
Avoid LIVE vaccines during chemotherapy or period immunosuppression. Herd immunity (all household members should be up-to-date)
| Influenza | Pneumococcal | Meningococcal | HPV |
| Annually | New, vaccine-naïve: PCV12 PPSV23 8-wk after Prior PPSV23: PCV13 after ≥1 year Follow high-risk adult guidelines for subsequent PPSV23 | High risk: persistent complement deficiency, on eculizumab, asplenia (anatomic/functional) | Offer to ≤27 years old |