Anticancer causative agent: mTOR (Everolimus, Sirolimus, Temsirolimus)
AntiHCV regimen (AASLD–IDSA HCV Guideline):
| Regimen & Genotypes & Clinical Pearls | Dose & Duration |
|---|---|
| Harvoni (Sofosbuvir/Ledipasvir 400/90mg) 1, 4-6 Avoid acid reducers; NS5A resistance if 1a | 1 tablet daily Treatment-naive patients without cirrhosis or with compensated cirrhosis: 12 wk (8 wk if no cirrhosis, HCV RNA <6 million units/mL, no HIV coinfection) Decompensated cirrhosis: 12wk with ribavirin; 24wk without ribavirin Decompensated cirrhosis in patients with prior sofosbuvir- or NS5A inhibitor–based treatment failure: 24wk with ribavirin Liver transplant recipients (treatment-naive and treatment-experienced) without cirrhosis or with compensated cirrhosis: 12 weeks. Liver transplant recipients (treatment-naive and treatment-experienced) with decompensated cirrhosis (off-label use): 12 wk with ribavirin (treatment-naive) or 24 wks (treatment-experienced). Kidney transplant recipients (treatment-naive and non-DAA treatment–experienced) without cirrhosis or with compensated cirrhosis (off-label use): 12 wks. |
| Epclusa (Sofosbuvir/ Velpatasvir 400/100mg) All genotypes Acid-reducing agents; NS5A resistance if 3 | 1 tablet daily Treatment naive without cirrhosis or with compensated cirrhosis, genotypes 1-6: 12 wk Decompensated cirrhosis, genotypes 1-6: 12 wks with ribavirin, 24 wks without ribavirin Decompensated cirrhosis, with prior sofosbuvir or NS5A inhibitor-based treatment failure, genotypes 1-6: 24wks with ribavirin Post kidney transplant, genotypes 1-6; treatment-naive and non-DAA-experienced, without cirrhosis or with compensated cirrhosis: 12wks Post liver transplant, genotypes 1-6; Treatment naive and non–DAA–experienced, without cirrhosis or with compensated cirrhosis: 12 wks. Post liver transplant, genotypes 1-6; Decompensated cirrhosis: 12 wks with ribavirin (treatment naive) or 24 wks. |
| Mavyret (Glecaprevir/ Pibrentasvir 300/120mg) All genotypes Avoid decompensated cirrhosis. | 3 tablet daily with food Treatment-naive patients without cirrhosis or with compensated cirrhosis: Genotype 1-6: 8 weeks (12 wks if HIV/HCV-coinfected with genotype 4 and compensated cirrhosis). Treatment-experienced patients (all genotypes) without cirrhosis or with compensated cirrhosis: Glecaprevir/Pibrentasvir treatment failures: 16 wks with sofosbuvir and weight-based ribavirin. Treatment-experienced patients (all genotypes) without cirrhosis or with compensated cirrhosis: Multiple DAA treatment failures, including sofosbuvir/velpatasvir/voxilaprevir or sofosbuvir plus glecaprevir/pibrentasvir: 16 wks with sofosbuvir and weight-based ribavirin (24 weeks in genotype 3 with cirrhosis or failure following sofosbuvir plus glecaprevir/pibrentasvir). Treatment-experienced patients (all genotypes) without cirrhosis or with compensated cirrhosis: Sofosbuvir-based treatment failures (alternative agent): 16 weeks (not recommended if prior exposure to an NS5A inhibitor plus NS3/4 protease inhibitor regimen [elbasvir/grazoprevir] or for genotype 3 infection with sofosbuvir/NS5A inhibitor experience). Hepatitis C, chronic, posttransplant (kidney, liver): 12 wks (not recommended for use in DAA treatment–experienced kidney or liver transplant recipients. Oral: 3 tablets (glecaprevir 100 mg/pibrentasvir 40 mg per tablet) once daily for 12 weeks (Ref). |
| + Ribavirin Add in decompensated cirrhosia | +12–24 wk Use in combo only; many ADEs |
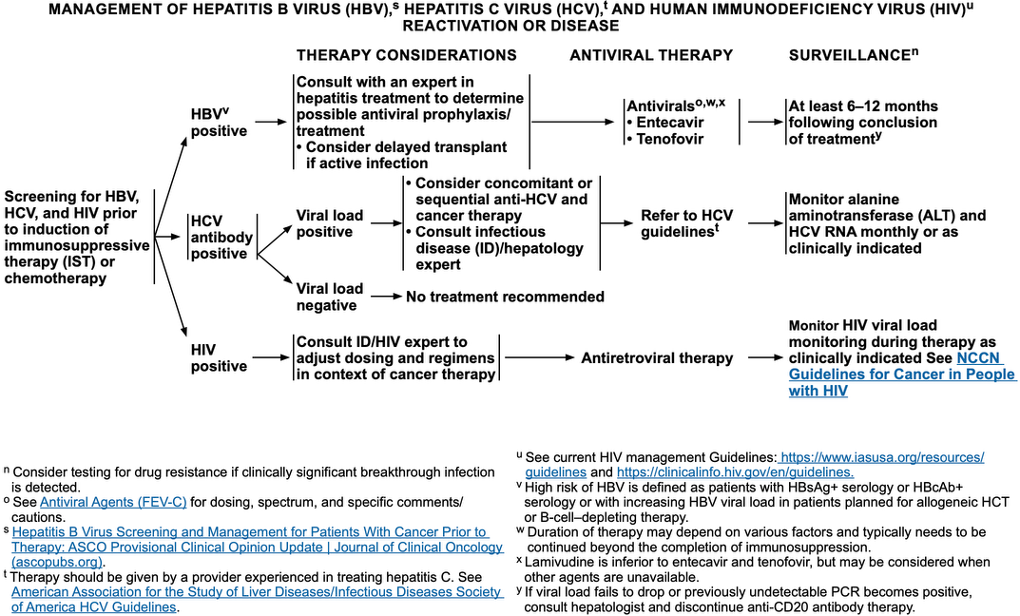
Studies for HCV reactivation in patients with cancer are not as expansive as studies for hepatitis B; however, an increase in mortality was reported in patients with cancer who had HCV infection compared to patients with cancer who were HCV negative. A review by Yazici et al summarized studies of HCV reactivation in patients receiving targeted therapies and the data correlated an increase in HCV reactivation with these therapies. Differences in outcomes between patients who are HCV positive with cancer versus HCV positive without cancer were reported to include higher occurrence of occult infection, higher risk of developing early cirrhosis, higher rate of fibrosis progression, development of viral reactivation, and poorer virologic outcomes (reviewed by Borchardt et al). The guidelines from the joint IDSA and AASLD Panels for the testing, management, and treatment of hepatitis C recommend that treatment for HCV be considered for patients with chronic HCV with a life expectancy of >12 months.
All patients who are expected to receive chemotherapy or IST should be screened for HCV. The data are limited regarding the treatment of HCV in patients with cancer, but it is generally not recommended that HCV treatment and cancer therapy be given concurrently. The IDSA/AASLD guidelines can provide additional guidance for antiviral therapy, but an infectious diseases consult is necessary to evaluate the use of concomitant or sequential anti-HCV and cancer therapy. Monitoring of ALT levels and HCV viral load monthly, or as clinically indicated, should be initiated as part of surveillance (see Management Of Hepatitis B Virus, Hepatitis C Virus, And Human Immunodeficiency Virus Reactivation Or
NCCN B-cell Lymphoma Guideline
New evidence from large epidemiologic studies, molecular biology research, and clinical observation supports an association between HCV and B-cell non-Hodgkin lymphoma (NHL). Recently approved direct-acting antiviral (DAA) agents for chronic carriers of HCV with genotype 1 demonstrated a high rate of sustained viral responses.
- Low-grade B-cell NHL
- According to the American Association for the Study of Liver Diseases, combined therapy with DAA agents should be considered in asymptomatic patients with HCV genotype 1 since this therapy can result in regression of lymphoma.
- Aggressive B-cell NHL
- Patients should be initially treated with chemoimmunotherapy regimens as outlined in these guidelines.
- Liver functional tests and serum HCV RNA levels should be closely monitored during and after chemoimmunotherapy for development of hepatotoxicity.
- Antiviral therapy should be considered in patients in complete remission after completion of lymphoma therapy.