HSV is a key pathogen in neutropenia and mucositis, mainly due to reactivation of latent virus. Reactivation/infection occurs in 60–80% of seropositive HCT recipients and acute leukemia patients without prophylaxis. In allogeneic HCT, HSV typically reactivates within the first month post-transplant but can occur later with intense immunosuppression. While disseminated infection is uncommon, HSV reactivation worsens mucosal damage, increasing pain, impairing oral intake, and raising the risk of secondary infections.
Anticancer agent: alkylating (Bendamustine), antimetabolite (fludarabine – intermediate risk), prolonged steroids (≥20mg/d prednisone x4wk or equivalent), cytotoxic chemotherapy (induction or consolidation therapy for acute leukemia), BTKi (Ibrutinib, Acalabrutinib, Zanubrutinib, Pirtobrutinib), JAKi (Momelotinib, Ruxolitinib, Fedratinib, Pacritinib), BiTE (Blinatumomab, Teclistamab-cgyv, Elranatamab-bcmm, Epcoritamab-bysp, Glofitamab-gxbm, Mosunetuzumab-axgb, Talquetamab-tgvs), antiCD20 (Rituximab, Obinutuzumab, Ofatumumab), antiCD30 (Brentuximab vedotin), antiCD20 (alemtuzumab – high risk), antiCD38 (Daratumumab, Isatuximab), antiCD52 (Alemtuzumab), antiCD319/SLAMF7 (Elotuzumab), CCR4 (Mogamulizumab), IL6i (Tocilizumab, Siltuximab), ADC (Polatuzumab vedotin-piiq)
Cancer/condition: CLL (intermediate risk), acute leukemia (high risk), autoHCT (intermediate risk), alloHCT (high risk), GVHD (high risk), lymphoma (intermediate risk), multiple myeloma (intermediate risk), hematologic malignancies with prolonged neutropenia
HSV Prophylaxis
Recommend HSV ppx: BiTE (Teclistamab-cgyv, Elranatamab-bcmm, Epcoritamab-bysp, Glofitamab-gxbm, Mosunetuzumab-axgb, Talquetamab-tgvs), antiCD38 (Daratumumab, Isatuximab), antiCD52 (Alemtuzumab), antiCD319/SLAMF7 (Elotuzumab), CCR4 (Mogamulizumab),
CAR T-cell CD19 (Axi-cel, Brex-cel, Tisa, Liso-cel), CAR T-cell BCMA (Ide-cel, Cilta-cel)
Consider HSV ppx: BTKi (Ibrutinib, Acalabrutinib, Zanubrutinib, Pirtobrutinib), JAKi (Momelotinib, Ruxolitinib, Fedratinib, Pacritinib),
BiTE (Blinatumomab), antiCD20 (Rituximab, Obinutuzumab, Ofatumumab), antiCD30 (Brentuximab vedotin), ADC (Polatuzumab vedotin-piiq), anticipated neutropenia ≥7 days or <7 days if HSV+ (≤500, or ≤1000 with ≤500 in 48h)
Choice of HSV medication: acyclovir, valacyclovir, famciclovir foscarnet (if acyclovir-resistant)
In CMV prophylaxis, Letermovir might requires additional HSV prophylaxis (ganciclovir, foscarnet are active against HSV)
| Medication | Spectrum | ADE and Clinical Pearls |
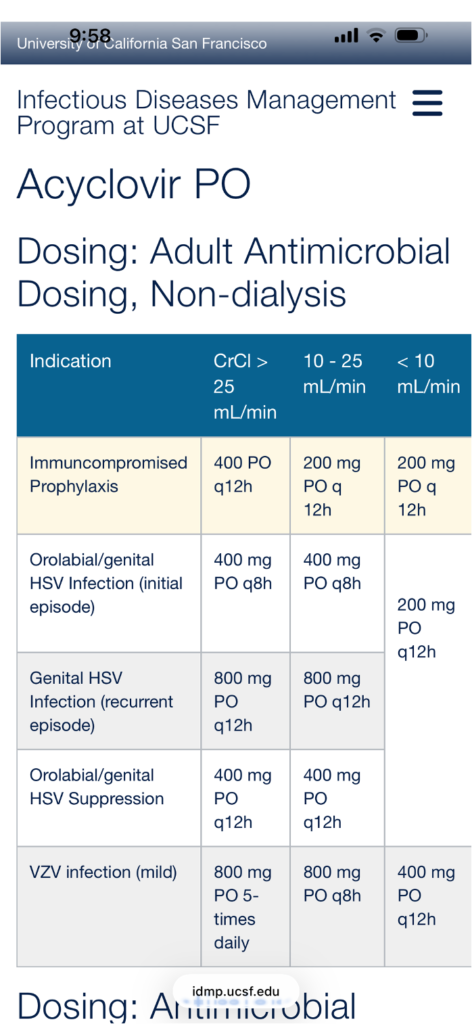
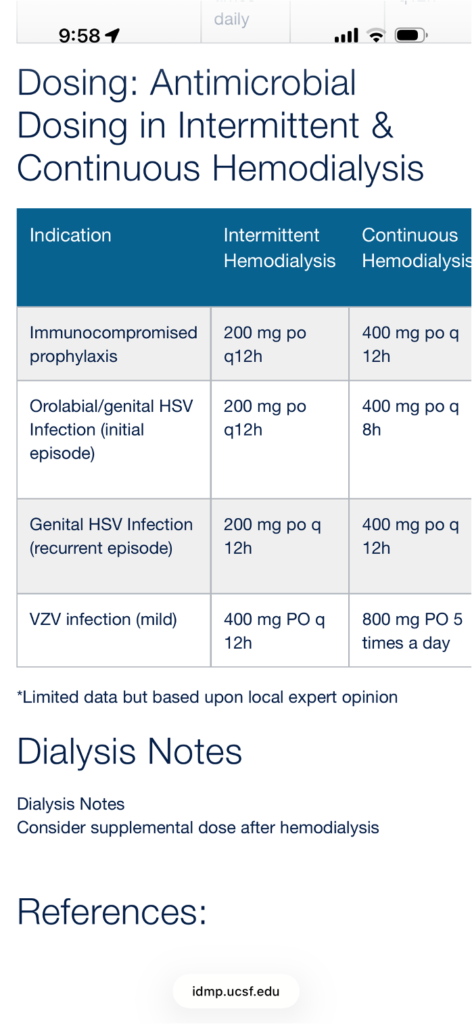
| Acyclovir PO/IV | HSV/VZV | Prophylaxis PO (high risk, HSV+): 400–800 mg BID Treatment IV Significant mucocutaneous HSV: 5 mg/kg q8h for 7–10 daysDisseminated HSV including viral encephalitis: 10 mg/kg q8h ADE: nephropathy (hydration to avoid crystal nephropathy with high dose). Dosing based on ideal body weight. High-dose have been used as CMV ppx (but weak activity; ganciclovir, valganciclovir, foscarnet if high CMV risk). |
| Valacyclovir PO | HSV/VZV | Prophylaxis PO (HSV+): 500 mg BID Treatment PO (preferred over acyclovir PO): 1 g TID It have been used as CMV ppx (but weak activity; ganciclovir, valganciclovir, foscarnet if high CMV risk). |
| Famciclovir PO | HSV/VZV | Prophylaxis PO: 250 mg BID Treatment PO: 250 mg TID No data for oncologic-related prophylaxis |
| Foscarnet IV | HSV/VZV CMV HHV-6 | Treatment IV (acyclovir-resistant HSV drug of choice): 40 mg/kg q8h for 7–10 days ADE: nephrotoxic; monitor electrolytes Limited clinical data for HHV-6/HHV-8. Treatment should be reserved for clinically documented disease; ID consult is highly recommended. |
| Ganciclovir IV | HSV/VZV CMV | May cause bone marrow suppression Limited clinical data for HHV-6/HHV-8 |
| Valganciclovir PO | HSV/VZV CMV | May cause bone marrow suppression Limited clinical data for HHV-6/HHV-8 |
| Cidofovir IV | HSV/VZV CMV Adenovirus | Treatment: 5 mg/kg every wk for 2 wks 5 mg/kg every 2 wks + probenecid PO 2g 3h before 1g 2h after 1g 8h after Cidofovir/hydration IV (reduce nephrotoxicity) Evidence is limited for treatment of adenovirus; when used, ID consult is strongly recommended Ocular toxicity, bone marrow toxicity |
| Doses are for adults and in normal renal function. All require renal dosing | ||
Duration of HSV
HSV Prophylaxis
| Disease/Therapy | Duration |
| Alemtuzumab AlloHCT GvHD requiring significant immunosuppression escalation | Minimum of 2 months after Alemtuzumab until CD4≥200 cells/mcL |
| Acute leukemia | During therapy and neutropenia periods |
| AutoHCT, lymphoma, MM, CLL, purine analog (fludarabine) | Consider during therapy or longer depend on immunosuppression degree |
Link to UCSF Acyclovir Oral dosing