NCCN 2025Clinical Pearls
- Most cancer diagnosed in HIV patients are NHL, Kaposi sarcoma (KS) and lung; declining with NHL and KS. HL is also common but the relationship with immune suppression is complex compared to NHL. Many have a strong association with EBV (~90% of PCNSL and HL, ~50% of BL, 40–50% of DLBCL [especially immunoblastic subtype]).
- Causes: Increased incidence due to unmasking immune reconstitution inflammatory syndrome (IRIS) soon after receiving ART [Immune Reacts, Illness Shows]. More likely to occurs with more immunosuppression (lower CD4+ T cell), exception for BL.
- Risk factors for worse survival: older, lymphoma while on ART, low CD4 at diagnosis, high HIV RNA (viral load), histology subtype.
- Evaluation: PE, ECOG, B symptoms (fever, night chills, wt loss), CBC, CMP, LDH, uric acid, PO4+, PET/CT, BM biopsy (if PET/CT is inadequate), LP (except for PEL), upper GI endoscopy, HBV/HCV, echo/MUGA (if anthracycline), beta2 micorglobulin, Ig quantitative, pregnancy.
- Subtype Evaluation: EBV, HHV8/KSHV (PEL), MYC, BCL2, BCL6, MUM1 (BL), CD4, HIV viral load
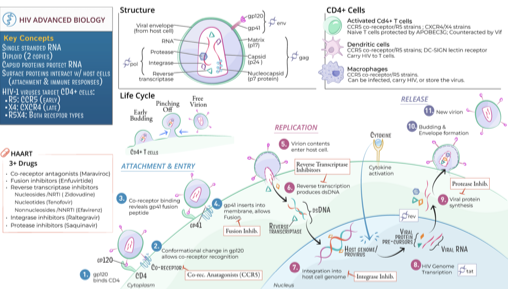
- Antiretroviral therapy (ART): may give with chemo (may affect chemo metabolism/toxicity). Avoid Zidovudine, Cobicistat, Ritonavir. Concomitant ART showed increase CR, OS and faster immune recovery. ART also allowed more dose-intense chemo and less toxicity. Rituximab also improves PFS and OS. DLBCL HIV on ART are candidates for CAR-T with appropriate supportive care. Consider prophylaxis against opportunistic infections if CD4<200.
- Types of HIV-associated B cell Lymphomas[ZA1] : most common are BL, PCNSL, DLBCL (including HHV8+); rare (<5%) with PEL, PBL
- HIV-related BL
- Worse prognosis if: CNS involvement, ECOG 2–4, ↑LDH, >1 extranodal site.
- 1L: modified R-CODOX-M/R-IVAC, DA-EPOCH-R, R-HyperCVAD alternating with HD MTX+AraC.
CODOX-M/IVAC had longer PFS & OS than DA-EPOCH or HyperCVAD.
- If CD4<50: maximize supportive care and monitor closely for cytopenia and infection
- G-CSF for all patients: filgrastim SC 5mcg/kg/d 24-72h after chemo, pegfilgrastim SC 6mg once 24h after chemo (avoid if within 14d of next chemo)
- If relapse (give 2L BL, limited data): DA-EPOCH-R (leptomeningeal) x6 cycles + IT MTX (if not previously given), RICE, RIVAC, R-HIDAC, RGDP
- If CR: consider HDT/ASCR ±ISRT, consider alloHCT±ISRT (if SC mobilization failure or BM involvement persists)
- If PR: additional 2L, consider HDT/ASCR ±ISRT, consider alloHCT±ISRT (if SC mob. failure or BM involvement persists)
- If NR/DP: clinical trial, best supportive care + palliative ISRT
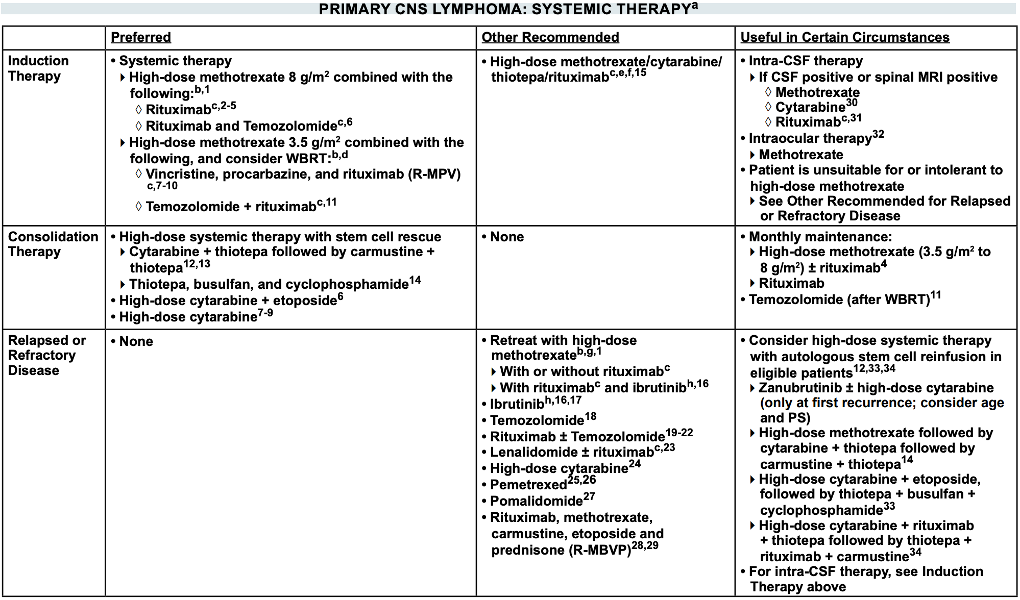
- HIV-related primary CNS lymphoma (PCNSL): brain, spine, CSF, leptomeninges; better prognosis, curable with less intensive chemo and ART even if opportunistic infections or poor healthcare access
- Start ART
- Consider HDMTX (even if poorly controlled HIV ± marginal ECOG[ZA2] ) or RT alone initially (if not candidate for systemic therapy)
- Systemic therapy (if good ECOG), supportive care
- HIV-related DLBCL, HHV8+ DLBCL, Primary Effusion Lymphoma (PEL)
- 1L: R-EPOCH, R-CHOP
- If CD4<50: maximize supportive care and monitor closely for cytopenia and infection
- If CD20-: remove Rituximab
- G-CSF for all patients
- CNS prophylaxis with intrathecal: ITMTX±ITAraC (4–8 doses) during or after the course of treatment
- PEL (pleura, pericardium, abdomen): caused by HHV8 (KSHV), often also EBV co-infection.
- Very poor prognosis (even in ART): 5y OS (National Cancer Database; n=10,769): DLBCL 42%, BL 45%, PCNSL 22%, PEL 28% (worst outcomes besides PCNSL). Combine ART with chemotherapy to improve survival.
- Poor prognosis factors: bad performance status, advanced disease, no ART before diagnosis.
- HIV-related Plasmablastic Lymphoma (PBL): jaw, oral; incidence is increasing, aggressive, CD20-, EBV+ (better EFS vs EBV-)
- Management same as HIV-
- Favorable prognostic factors: age <50y, early stage (SI-II)
- Worse prognosis: high IPI, BM involvement, PBL histology itself.
- 1L: EPOCH, modified CODOX-M/IVAC, HyperCVAD. CHOP is INADEQUATE
- If complete remission[ZA4] : consider HDT/ASCR in high risk (age-adj IPI>2, MYC+, TP53 gene deletion, HIV- PBL)
- CNS prophylaxis with intrathecal: ITMTX±ITAraC (4–8 doses) during or after the course of treatment
- Relapse: Brentuximab vedotin or below 2L (relapse <12mo or ≥12mo) without Rituximab
- TLS prophylaxis (monitor uric acid, Ca, PO4, K, SCr): hydration, allopurinol or Rasburicase (if uric acid>8, bulky disease)
- Management of relapse in DLBCL, HHV8+ DLBCL, PEL, PBL:
- Relapse <12mo (CAR-T eligible): Yescarta, Breyanzi; bridging therapy (DHAP, GDP, ICE, GemOx, PV±Benda±R, ISRT)
- Relapse <12mo (CAR-T ineligible): BiTE (Epcoritamab + GemOx, Glofitamab + GemOx), PV±Bendamustine±R, PV+Mosunetuzumab, Tafasitamab+Lenalidomide (not in refractory primary, “chemo-free regimen”),
- Other options: platinum-based chemo (DHAP±R, GDP±R, ICE±R, ESHAP±R), GemOx (if BiTE ineligible), CEOP±R, MINE±R, BV (if CD30+), ibrutinib (non-GCB DLBCL), R2 (non-GCB DLBCL)
- Relapse >12mo (ASCT eligible): platinum-based (DHAP±R, GDP±R, ICE±R, ESHAP±R, GemOx±R), MINE±R
- If CR: HD chemo f/b autoSCT ± ISRT (Category 1), alloSCT ± ISRT (consider); 75% relapse ~9mo of autoSCT.
- If PR: CAR T (anti-CD19; Yescarta, Breyanzi, Kymriah), HD chemo f/b autoSCT ± ISRT, alloSCT ± ISRT (consider).
- Relapse >12mo (ASCT ineligible): CAR-T (if eligible, Breyanzi), BiTE [Epcoritamab+GemOx, Glofitamab+GemOx (category 1)], PV±Bendamustine±R, PV+Mosunetuzumab, Tafasitamab+Lenalidomide (“chemo-free regimen”), CEOP±R, GDP±R, GemOx (if BiTE ineligible), Rituximab monotherapy, BV (if CD30+), ibrutinib (non-GCB DLBCL), R2 (non-GCB DLBCL)
- Include Rituximab if relapse after remission >6mo. Omit Rituximab if primary refractory.
- EPOCH (± Rituximab) in DLBCL, BL (mostly low-risk), PBL (+Bortezomib)
- AMC 034 (Concurrent vs Sequential Rituximab; n=106, 75% DLBCL, 25% BL/BL-like): CR 73% vs 55%, similar 2y PFS/OS (PFS ~65%, OS ~70%). Similar overall toxicity but higher mortality with CD4<50/mcL in concurrent rituximab. Concurrent ART showed faster immune recovery (↑CD4, ↓HIV viral load).
- AMC pooled analysis (150 patients, AMC 010 + 034; EPOCH-R vs R-CHOP): EPOCH-R had better EFS & OS (after adjusting for CD4 & aaIPI). Key risk: CD4 <50 → much higher death rate (37% vs 6%).
- Favorable prognostic factors: Low age-adjusted IPI, Baseline CD4 ≥100/mcL
- Dose-Adjusted EPOCH (DA-EPOCH; n=39, 79% DLBCL, 18% BL): ORR 87%, CR 74%, 5y PFS 73%, 5y OS 60%, 5y DFS 92%
- Risk factors for worse OS: Low CD4 (≤100 → OS 16% vs 87%), CNS involvement
- Short-Course EPOCH-RR (SC-EPOCH-RR, Rituximab Dose-Dense)
- DLBCL (n=33): CR 91%, 5y PFS 84%, 5y OS 68%, no excess infection deaths.
- BL (n=11, low-risk): PFS 100%, OS 90% (median FU ~7 yrs), less fever/neutropenia vs DA-EPOCH-R.
- EPOCH + Novel Agents
- Vorinostat + EPOCH-R (high-risk patients): no added benefit (CR ~74% vs 68%). Poorer prognosis if MYC+, low CD4, or rapid diagnosis-to-treatment interval.
- Bortezomib + EPOCH: Retrospective data: safe and effective in HIV-associated PBL.
- CHOP (± Rituximab) in DLBCL
- CHOP Alone: CR ~30–48%, median OS ~25 months
- AMC 010 (Phase III, n=150; 80% DLBCL, 9% BL; R-CHOP vs CHOP): CR 58% vs 47%, median TTP 29 vs 20mo, median OS 32 vs 25mo, similar median PFS 10 vs 9mo.
- Maint. Rituximab: No survival benefit (consistent with HIV- trials). Not recommended due to infection deaths
- Phase II Trials (6 cycles R-CHOP): CR/CRu 69–77%, 2y OS 75%, 3y OS 56%. Manageable toxicity.
- R-CDOP (liposomal doxorubicin instead of standard doxo)
- AMC 047 (n=40; ~98% DLBCL): ORR = 68% (CR = 48%), 1y PFS 61%, 1y OS 70%, 2y PFS 52%, 2y OS 62%. Toxicity: 40% infectious complications (5% G4), but no infection-related deaths (+ART + OI prophylaxis if CD4 ≤100).
- Comparison: Effective, but EPOCH is superior in outcomes.
- CODOX-M/IVAC (± Rituximab) in BL (mostly high-risk)
- Retrospective Study (80 BL patients, HIV+ and HIV–): similar CR 88% vs 93%, similar 3y PFS 68%, 3y OS 68% vs 72%
- Adding rituximab: trend toward better survival (3y PFS 74% vs 61%; OS 77% vs 66%)
- AMC 048 [Prospective, 34 HIV+ BL; 2 low-risk (R-CODOX-M only, 3 cycles), 32 high-risk (R-CODOX-M/IVAC), median FU 26mo]: 1y PFS 69%, 1y OS 72%, 2y OS 69%
- Retrospective Study (80 BL patients, HIV+ and HIV–): similar CR 88% vs 93%, similar 3y PFS 68%, 3y OS 68% vs 72%
- HyperCVAD (± Rituximab) alternating with high-dose methotrexate and cytarabine in BL/BL-like lymphoma
- CR 64%–92%, median OS ~12mo.
- Rituximab: Improves outcomes, especially in older patients.
- With ART: Effective and tolerable.
- Concurrent ART (DHHS and IDSA-HIVMA Guidelines)
- PIs (Ritonavir, Cobicistat) should be avoided due to DDI (CYP3A4 inhibitors/inducers) with vincr, doxo, cyclophos, etoposide…
- NNRTIs (Efavirenz, Nevirapine, Etravirine) best avoided due to DDI (CYP3A4 inducers)
- NRTIs backbone (Tenofovir [TAF, TDF], Emtricitabine [FTC], Lamivudine [3TC])
- INSTIs (Dolutegravir, Bictegravir) has minimal DDI. Choices: BIC/TAF/FTC, DTG/TAF/FTC, DTG/TDF/FTC, DTG/TDF/3TC
- HBV coinfection: (TDF or TAF) + (FTC or 3TC) + INSTI (Dolutegravir, Bictegravir). ETV+DTG+ABC/3TC (if Tenofovir ineligible)
- HCV coinfection: Glecaprevir/Pibrentasvir (Mavyret) 3 tablets/day with food x8-12 weeks; avoid in decompensated cirrhosis. Sofosbuvir/velpatasvir x12 weeks
- HIV RNA PCR monthly until undetectable then q3-4mo; CD4 counts q3mo (if <300 cells/mm³) then q6mo (if higher)
- Opportunistic Infections
- CMV, HSV, mpox, talaromycosis (formerly penicilliosis), cystoisosporiasis (formerly isosporiasis), HHV8, cryptosporidiosis, microsporidiosis, progressive multifocal leukoencephalopathy (PML).
While most cancers are not diagnosed in young with HIV; lung, anal, myelomas may occur in young with HIV (vs no HIV). HPV-related cancers are cervical, vaginal, vulvular, anal. Vaccinations against HPV, HBV reduces risk of cervical, anal, head/ neck cancers and HCC. Providers should be alert for human oncogenic viral-based cancers related to EBV,HPV,HCV,HBV, even if no recommended screening.
| Regimens | Medications |
| R-CODOX-M | Rituximab, Cyclophosphamide, vincristine (Oncovin), DOXorubicin, Methotrexate (high-dose) |
| R-CODOX-M/ R-IVAC | Rituximab, Cyclophosphamide, vincristine (Oncovin), DOXorubicin, Methotrexate (high-dose) Alternating with Rituximab, Ifosfamide, Mesna (uroprotection), etoposide (Vepesid), cytarabine (high-dose AraC) CNS prophylaxis: Intrathecal MTX or Ara-C in every cycle. |
| R-HyperCVAD | Rituximab, Hyperfractionated (smaller doses but more frequent), Cyclophosphamide, Vincristine, doxorubicin (Adriamycin), Dexamethasone [+IT MTX +IT AraC] Alternating with rituximab, high-dose methotrexate and cytarabine [+IT MTX +IT AraC] |
| DA-R-EPOCH | Dose-Adjusted Rituximab, Etoposide, Prednisone, vincristine (Oncovin), Cyclophosphamide, doxorubicin (Hydroxydaunorubicin) [+IT MTX] |
| SC-EPOCH-RR | Short-Course Etoposide, Prednisone, Vincristine (Oncovin), Cyclophosphamide, Doxorubicin (Hydroxydaunorubicin), Rituximab, Rituximab |
| R-CHOP | Rituximab, Cyclophosphamide, doxorubicin (Hydroxydaunorubicin), vincristine (Oncovin), Prednisone |
| R-IVAC | Rituximab, Ifosfamide, Mesna (uroprotection), etoposide (Vepesid), cytarabine (high-dose Ara-C), |
| R-GDP | Rituximab, Gemcitabine, Dexamethasone, Platinum (carboplatin, cisplatin) [+IT MTX] |
| R-ICE | Rituximab, Ifosfamide, Carboplatin, Etoposide [+IT MTX] |
| R-HiDAC | Rituximab, High Dose Cytarabine (Ara-C) |
| DHAP | Dexamethasone, cytarabine (High-dose Ara-C), Platinum (carboplatin, cisplatin, oxaliplatin) |
| ICE | Ifosfamide, Carboplatin, Etoposide |
| ESHAP | Etoposide, methylprednisolone (Solu-Medrol), cytarabine (High-dose Ara-C), Platinum (cisplatin) |
| CEOP | Cyclophosphamide, Etoposide, vincristine (Oncovin), Prednisone |
| CDOP | Cyclophosphamide, liposomal Doxorubicin, vincristine (Oncovin), Prednisone |
| MINE | Mesna (uroprotectant, supportive), Ifosfamide, mitoxaNtrone, Etoposide |
| GemOx | Gemcitabine, Oxaliplatin |
| R2 | Rituximab, lenalidomide (Revlimid) |