Extended-spectrum β-lactamase-Producing Enterobacterales (ESBL-E)
ESBLs are enzymes that inactivate most penicillins, cephalosporins, and aztreonam. EBSL-E generally remains susceptible to carbapenems.
- Most common bacteria: Escherichia coli, Klebsiella pneumoniae, Klebsiella oxytoca, and Proteus mirabilis
- Type of ESBLs: CTX-M enzymes, TEM and SHV β- lactamases.
- Some but not all can be determined by: ceftriaxone minimum inhibitory concentrations [MICs] ≥2 µg/mL
Regimens
- Uncomplicated cystitis
- Preferred: Nitrofurantoin, TMP-SMX
- Alternative: Ciprofloxacin, levofloxacin, carbapenems
- Ecoli only (alternative): aminoglycoside (as a single dose) and oral fosfomycin
- Pyelonephritis or cUTI
- Preferred: TMP-SMX, ciprofloxacin, or levofloxacin
- Preferred (if resistant/toxicities with TMP-SMX or fluoroquinolones): Ertapenem, meropenem, imipenem-cilastatin
- Alternative: Aminoglycosides
- Non-UTI
- Preferred: Meropenem, imipenem-cilastatin, ertapenem
- Preferred (critically ill, hypoalbuminemia): meropenem, imipenem-cilastatin → after appropriate clinical response and susceptibility: transition to oral TMP-SMX, ciprofloxacin, levofloxacin
Piperacillin-tazobactam: If piperacillin-tazobactam was initiated as empiric therapy for uncomplicated cystitis caused by an organism later identified as an ESBL-E and clinical improvement occurs, no change or extension of antibiotic therapy is necessary. The panel suggests TMP-SMX, ciprofloxacin, levofloxacin, or carbapenems rather than piperacillin-tazobactam for the treatment of ESBL-E pyelonephritis or cUTI, with the understanding that the risk of clinical failure with piperacillin-tazobactam may be low. Piperacillin-tazobactam is not suggested for the treatment of infections outside of the urinary tract caused by ESBL-E, even if susceptibility to piperacillin-tazobactam is demonstrated.
Cefepime: If cefepime was initiated as empiric therapy for uncomplicated cystitis caused by an organism later identified as an ESBL-E and clinical improvement occurs, no change or extension of antibiotic therapy is necessary. The panel suggests avoiding cefepime for the treatment of pyelonephritis or cUTI. Cefepime is also not suggested for the treatment of infections outside of the urinary tract caused by ESBL-E, even if susceptibility to cefepime is demonstrated.
Cephamycins: not suggested until more data are available.
Newer β-lactam-β-lactamase inhibitor combinations and cefiderocol: The panel suggests that ceftazidime-avibactam, meropenem-vaborbactam, imipenem-cilastatin-relebactam, ceftolozane-tazobactam, and cefiderocol be preferentially reserved for treating infections caused by organisms exhibiting carbapenem resistance.
AmpC β-Lactamase-Producing Enterobacterales
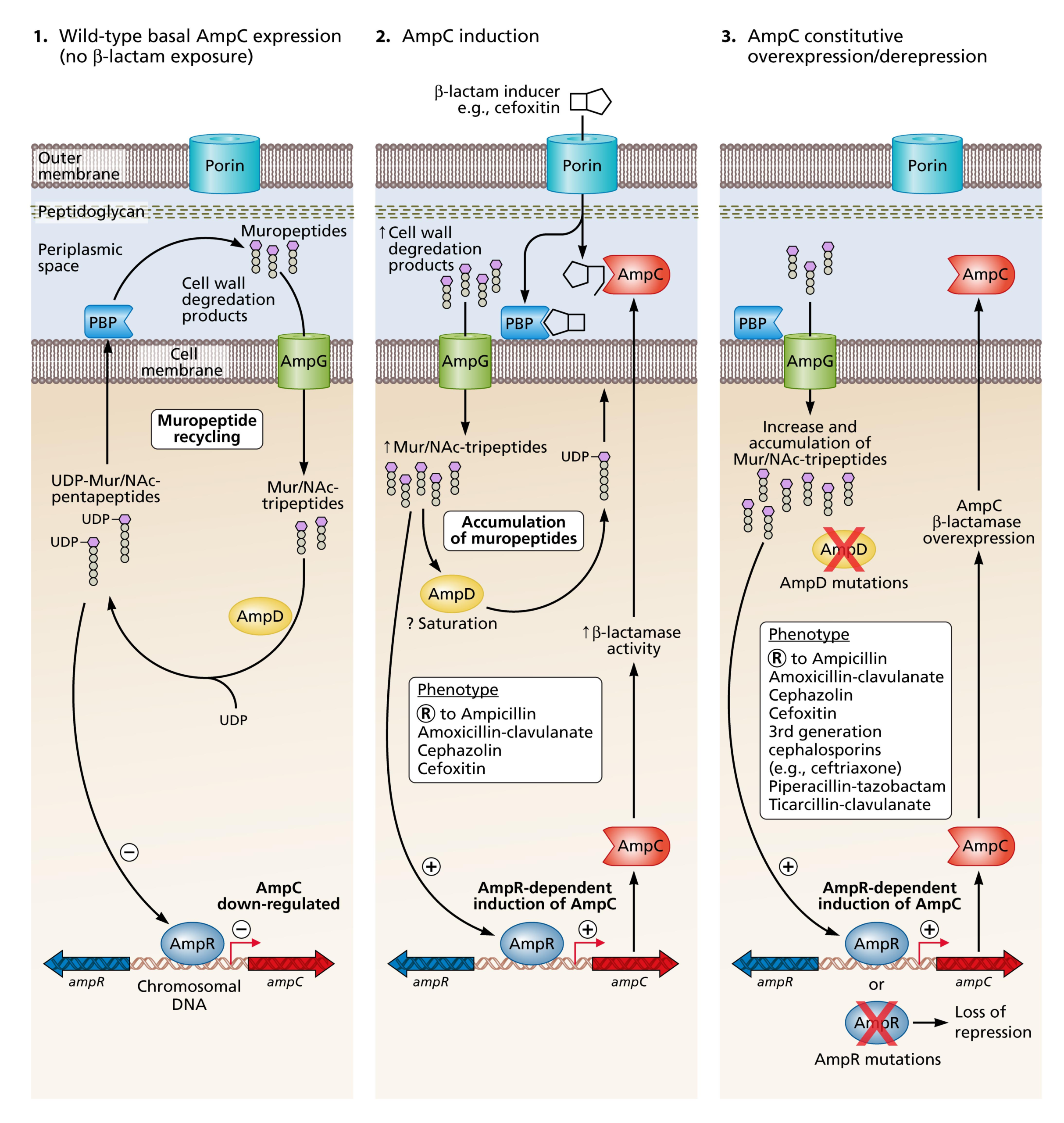
- Most common moderate risk for inducible AmpC production: Enterobacter cloacae complex, Klebsiella aerogenes, and Citrobacter freundii
Carbapenem-Resistant Enterobacterales
k
Pseudomonas aeruginosa with Difficult-to-Treat Resistance (PsA-DTR)
k
Carbapenem-Resistant Acinetobacter baumannii (CRAB)
Stenotrophomonas maltophilia
- Resistance mechanisms
- L1 metallo-β-lactamase (MBL): hydrolyzes carbapenems and most β-lactams but not avibactam, tazobactam, or clavulanate
- L2 serine cephalosporinase: Hydrolyzes cephalosporins and aztreonam
- Multiple efflux pumps
- Reduced outer membrane permeability
- Ability to form biofilms
- Frequent acquisition of resistance during therapy
S. maltophilia can be a true pathogen that causes considerable morbidity and mortality, particularly in patients with hematologic malignancies where it can cause hemorrhagic pneumonia or bacteremia699-705.