| Hallmark (normal values) | Risk of getting TLS |
|---|---|
| Hyperkalemia (3.5–5 mmol/L): ≥6 mmol/L or 25% increase from baseline Hyperuricemia (2.7–7.8 mg/dL): ≥8 mg/dL or 25% increase from baseline Hyperphosphatemia (2.4–5 mg/dL): ≥4.5 mg/dL or 25% increase from baseline Hypocalcemia (8.8–10.5 mg/dL): ≤7 mg/dL (chelation with phos) or 25% decrease from baseline | High (WBC AML≥50, ALL≥100), Burkitt’s, B-ALL Moderate (WBC AML 10-50, ALL 50-100, CLL 10-100), DLBCL Low (WBC AML≤10, ALL≤50, CLL ≤10), indolent NHL |
Cairo-Bishop Definitions
- Laboratory TLS (LTLS): ≥2 abnormal serum values or change by 25% within 3 days before or 7 days after initiation of therapy
- Clinical TLS (CTLS): laboratory TLS plus ≥1 of the following (SCr >1.5 ULN, cardiac arrhythmia or sudden death, seizures). It may not be directly/probably attributable to therapeutic agent. Goal is to prevent it!
Risk Factors: Rapid cell death after chemo in leukemia/lymphoma or high tumor burdens (chemosensitivie)
- Dehydration, acidic urine, oliguria, anuria, low urinary flow, renal insufficiency, preexisting uremia or hyperuricemia, large tumor burden, tumor chemosensitive (NHL, AML, ALL), high tumor cell proliferation rate, increased LDH level.
Clinical Manifestation (spontaneous or 12-72h after chemo): NVD, fluid overload, hematuria; CHF, tetany, syncope, and possible sudden death
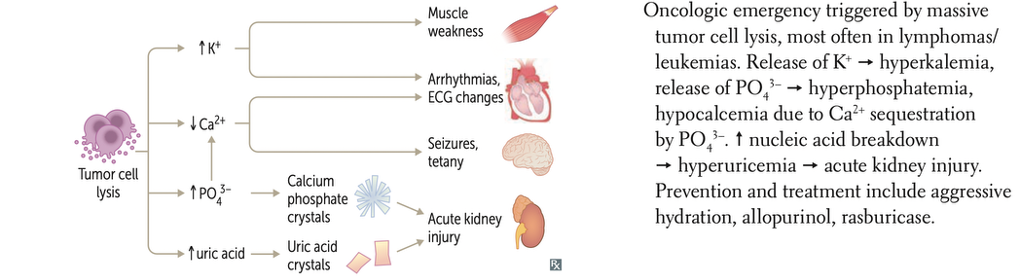
- Cardiac: Arrhythmias, cardiac arrest (from hyperkalemia, hypocalcemia)
- Renal: Oliguria, AKI (from uric acid & Ca-PO₄ precipitation)
- Neurologic: Seizures, confusion, muscle spasms (from hypocalcemia)
Complications: renal failure (that might put patients on dialysis)
Chemotherapy to start anti-TLS: 7+3 (cytarabine + daunorubicin/idarubicin) in AML; venetoclax; DA-R-EPOCH in lymphoma, high tumor burden, age ≥65 years
Management
| Intervention | Negligible Risk | Low Risk | Intermediate Risk | High Risk |
|---|---|---|---|---|
| Monitoring | None | Daily (OP/IP) | Every 8-12 hrs (Inpatient) | Every 6-8 hrs +ECGs (IP) |
| Hydration | None | IV Fluids | IV Fluids | IV Fluids (aggressive) |
| Drug Intervention | None | ± Allopurinol | Allopurinol or Rasburicase (if renal issues) | Rasburicase |
IV Hydration
- Hyperhydration (2.5-3L/m2/day; NS 3–5 L/m²/day, avoid LR [contains K]): improve renal profusion and GFR, promote excretion of uric acid and phosphate (goal high UOP: ≥80-100 mL/m2/h in adults)
- Loop diuretics (furosemide) if volume overload; ensure no obstructive uropathy and/or hypovolemia present
- Urine alkalinization with IV sodium bicarbonate: solubility of uric acid increases to 200 mg/dL with pH 7. It’s no longer used as it does not increase solubility of xanthines, and may ppt Ca/Phos
- Monitor vital signs, I/O’s (ins/outs)
Hyperuricemia (3 days before or 7 days after chemotherapy)
- Allopurinol (Aloprim IV® Zyloprim PO®; xanthine oxidase inh; prevents uric acid production) [NCCN: use for intermediate risk]
- Dose: 100 mg/m2/dose q8h upto 800 mg/d (some limit 300 mg/d); renal dosing. If ppx, can be started 2d before chemo
- Duration of therapy: continue until tumor burden, WBC count, uric acid, and pertinent laboratory values have normalized
- Rasburicase (Elitek®, recombinant xanthine oxidase [enzyme] allantoin [more soluble]) [NCCN: use for high risk patients]
- FDA approved indication: initial management of plasma uric acid levels for pediatric/adult patients with leukemia, lymphoma, and solid tumor malignancies who are receiving anticancer therapy expected to result in TLS and hyperuricemia
- Dose (FDA) 0.2 mg/kg/day upto 5 days
- Off-label (flat dosing) 3–7.5 mg – 6mg in a single dose due to cost
- Case reports, case series, and reviews on single full dose: lowered uric acid to less than uric acid assay (started in 2006 in adults). Efficient and cost-effective method to lower uric acid in patients with TLS
- Off-label (flat dosing) 3–7.5 mg – 6mg in a single dose due to cost
- Warnings and precautions: hypersensitivity/anaphylaxis, hemolysis in G6PD deficiency (CI), methemoglobinemia, blood samples must be sent on ice to prevent uric acid degradation (from Rasburicase) and falsely low results.
Hyperkalemia (K⁺ >6 mEq/L): Calcium gluconate 1 g IV, Insulin + Dextrose, Sodium bicarbonate, Sodium polystyrene (kayexalate)
Hyperphosphatemia (PO₄³⁻ >6 mg/dL): Phosphate binders (Sevelamer 800-1600 mg PO TID), lanthanum, avoid phosphate-containing fluids
Hypocalcemia (Ca²⁺ <7 mg/dL): Treat ONLY if symptomatic (tetany, seizures, arrhythmias) as it can worsen Ca-PO₄ precipitation & AKI: Calcium gluconate 1-2 g IV
Summary TLS Management
| Intervention | Indication | Dose/Regimen | Clinical Pearl |
|---|---|---|---|
| Fluids (NS 0.9%) | Prevention & Treatment | 3–5 L/m²/day | Avoid LR (contains K⁺) |
| Allopurinol | Prevention | 300 mg PO daily | Does NOT lower existing uric acid |
| Rasburicase | Treatment (Uric acid >8) | 0.15–0.2 mg/kg IV once | Avoid in G6PD deficiency |
| Calcium gluconate | Symptomatic hypocalcemia | 1–2 g IV | Avoid if asymptomatic |
| Insulin + Dextrose | Hyperkalemia (K⁺ >6) | 10 units IV + D50 | Moves K⁺ intracellularly |
| Phosphate binders (Sevelamer, Lanthanum) | Hyperphosphatemia | Sevelamer 800–1600 mg PO TID | Only oral; ineffective acutely |
| Dialysis | Severe TLS | Emergency intervention | Needed if refractory to treatment |