Hem/Onc Pharmacotherapy Specialist Quick Reference Guide
Based on NCCN Guidelines Version 5.2026 | January 2026
OVERVIEW & EPIDEMIOLOGY
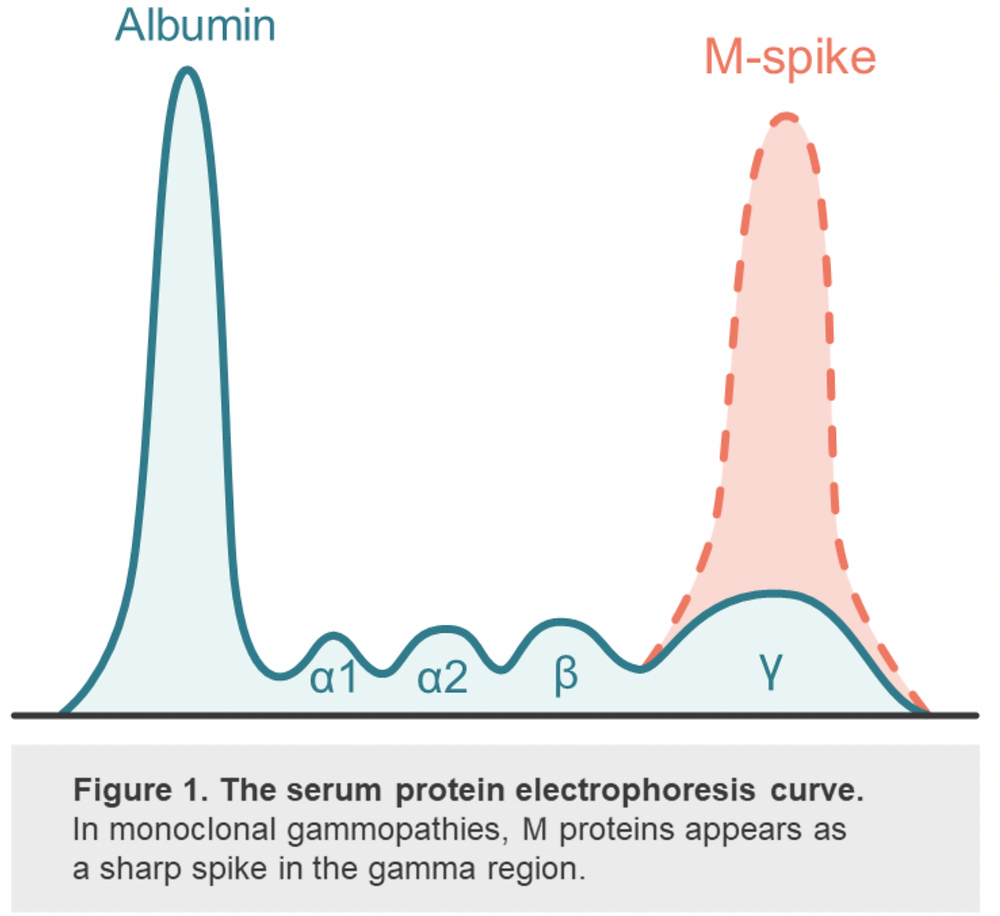
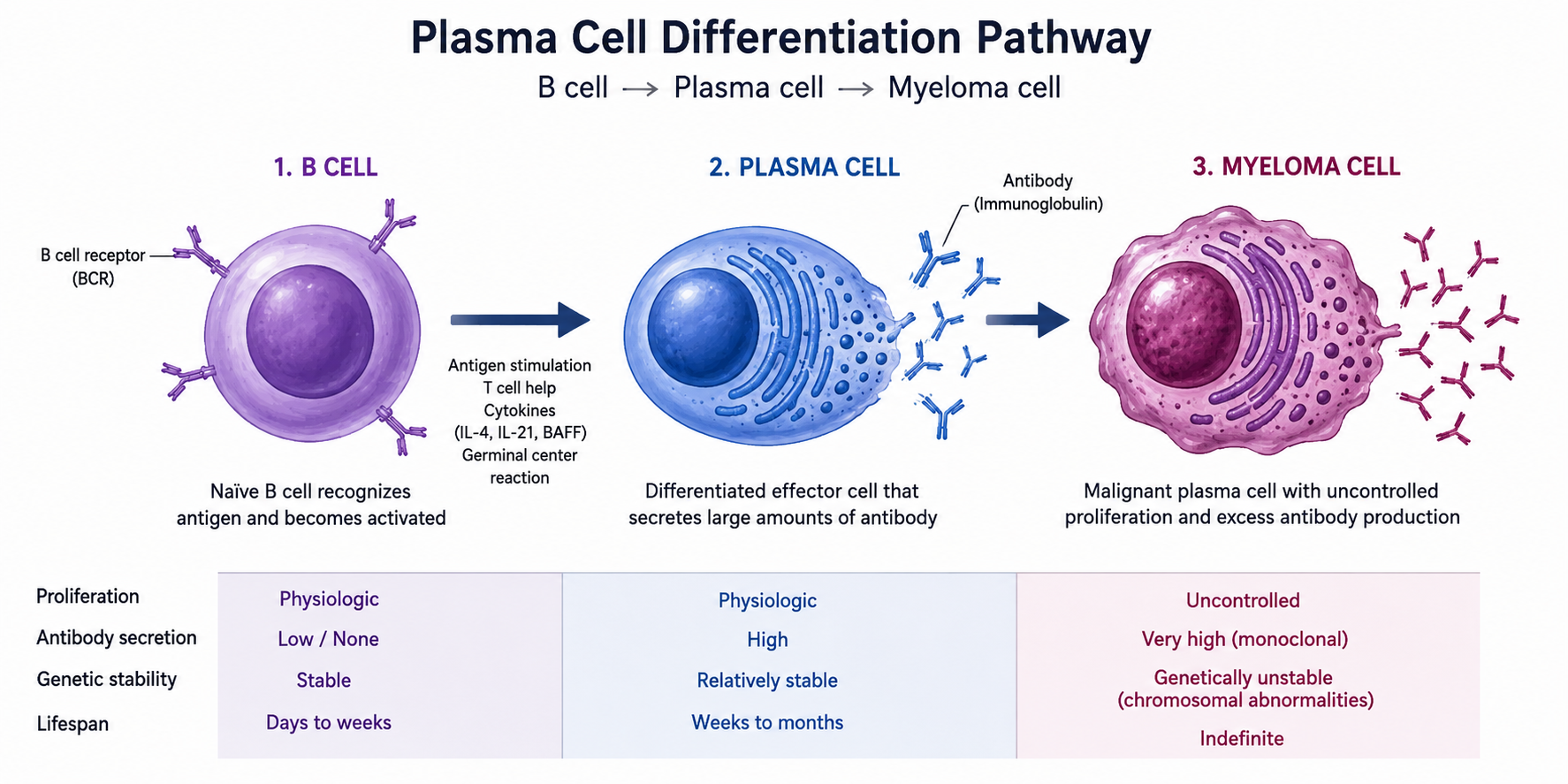
Multiple Myeloma (MM) is a malignant plasma cell disorder characterized by clonal proliferation of plasma cells in the bone marrow, production of monoclonal immunoglobulin (M-protein), and end-organ damage.
Key Epidemiology Facts
- ~35,000 new cases/year in the US; median age ~65–70 years
- 2nd most common hematologic malignancy after non-Hodgkin lymphoma
- Black/African American individuals have TWICE the incidence of all other races/ethnicities and earlier age at diagnosis
- Black/African Americans present with more severe symptoms: increased anemia, higher calcium, worse renal dysfunction, more extramedullary disease
- Black/African Americans more likely to have chr 14 translocations [t(11;14), t(14;16), t(14;20)]; LESS likely to have del17p, gain/amp 1q
💎 Pearl: Duffy-null phenotype (~67% of Black/African Americans) causes lower baseline ANC — do NOT use rigid reference ranges that may lead to inappropriate dose delays or reductions. This is physiologically insignificant regarding myeloma treatment. Duffy-null phenotype is a genetic RBC/chemokine receptor phenotype.
SIGNS & SYMPTOMS (CRAB/SLiM Criteria)
CRAB — Myeloma-Defining End-Organ Damage
| Acronym | Criterion | Definition/Threshold |
| C | HyperCalcemia | Serum Ca >0.25 mmol/L (>1 mg/dL) above ULN OR Serum Ca >2.75 mmol/L (>11 mg/dL) |
| R | Renal Insufficiency | CrCl <40 mL/min OR Serum creatinine >177 µmol/L (>2 mg/dL) |
| A | Anemia | Hgb >20 g/L below LLN OR Hgb <100 g/L |
| B | Bone Lesions | ≥1 osteolytic lesion on skeletal radiography, CT, or PET-CT |
Biomarkers of Malignancy (SLiM Criteria — for NDMM without CRAB)
- S — Sixty percent (≥60%) clonal bone marrow plasma cells (BMPC)
- Li — Light chain ratio: involved:uninvolved FLC ratio ≥100
- M — More than 1 focal lesion on MRI studies (>1 cm)
Other Signs & Symptoms
- Bone pain (most common): back pain, rib pain, pathologic fractures
- Fatigue, weakness, dyspnea from anemia
- Recurrent infections (pneumonia, sinusitis) — hypogammaglobulinemia (low normal immunoglobulins/antibodies in the blood due to the malignant plasma cell clone produces one monoclonal immunoglobulin — the M-protein — while suppressing normal plasma cells; therefore, high “total protein” or high M-spike, but their functional normal antibodies are low)
- Peripheral neuropathy (especially with amyloidosis or thalidomide/bortezomib)
- Hyperviscosity: headache, visual changes, bleeding, confusion
- Spinal cord compression — neurologic emergency
- Weight loss, night sweats, fever (uncommon — rule out other hematologic malignancies)
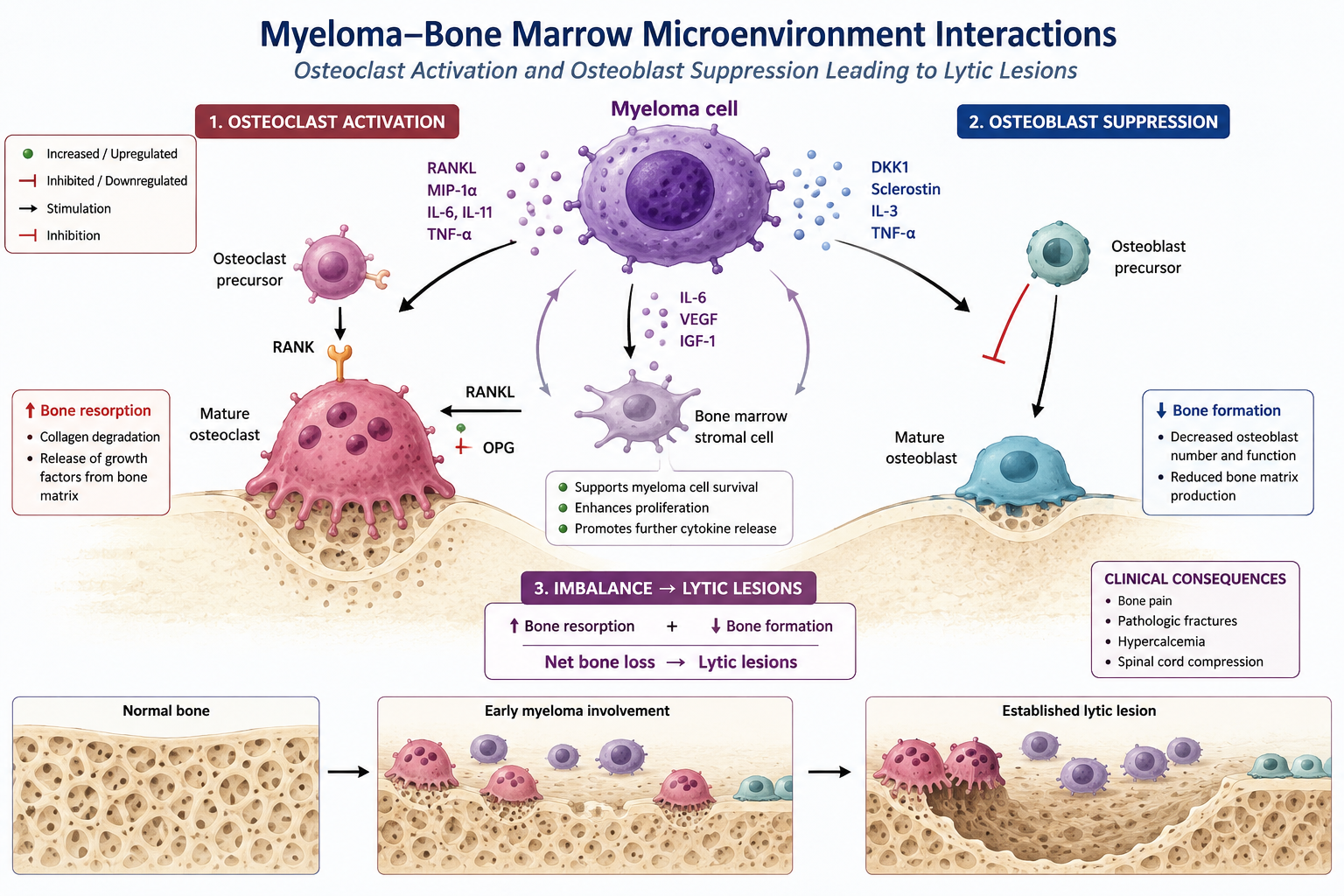
⚠ ~80% of MM patients have bone disease and up to 33% have renal compromise at diagnosis — aggressive supportive care is critical to avoid early complications.
DISEASE DEFINITIONS (MYEL-A)
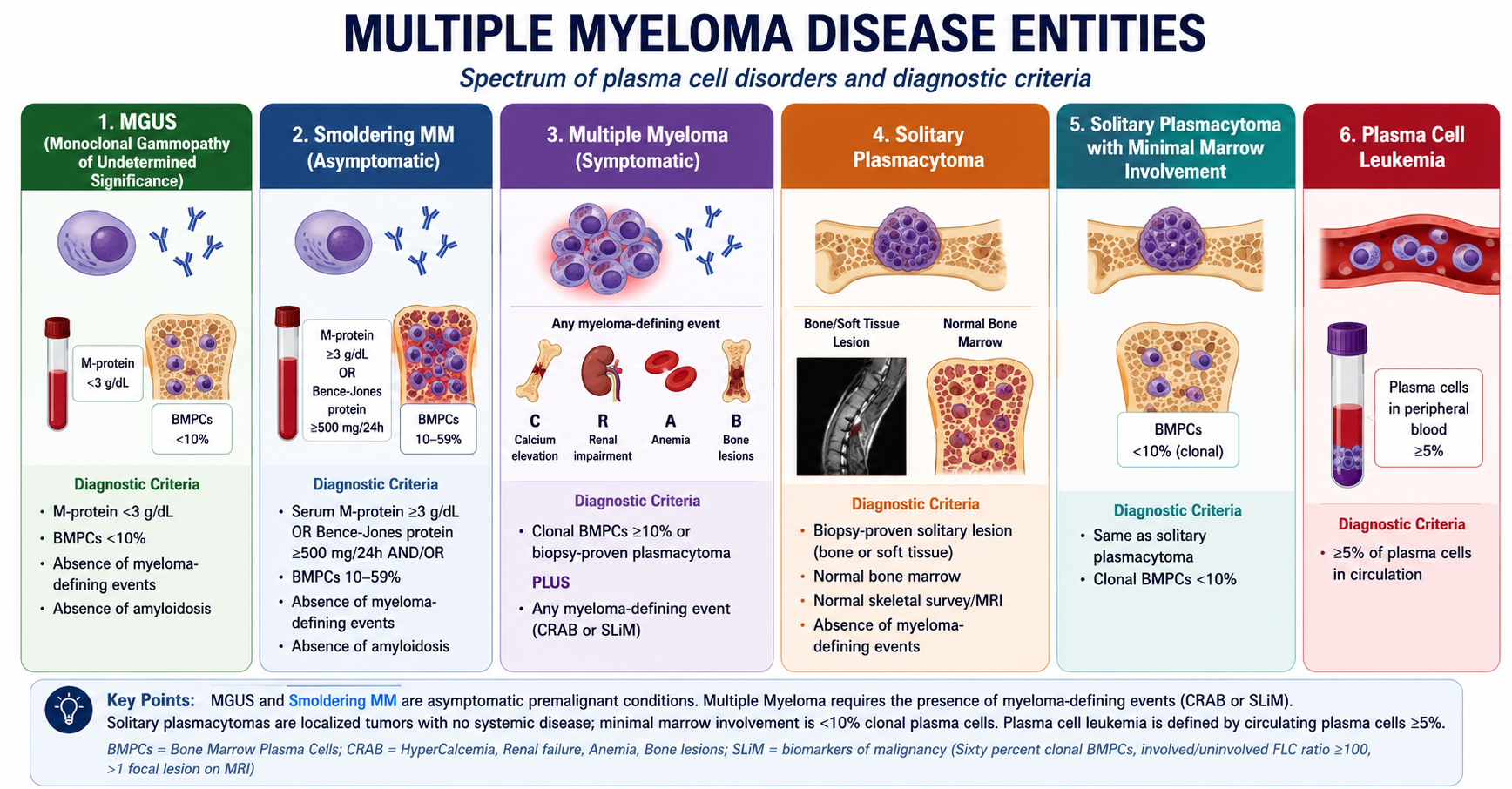
⚠ If BMPCs ≥10% in a solitary plasmacytoma → treat as active (symptomatic) MM and initiate systemic therapy. Also consider FISH testing on plasmacytoma biopsy if clonal cells absent/inadequate in marrow.
Smoldering MM Risk Stratification (for Progression to Active MM)
High-risk SMM defined as ≥2 of the following risk factors (Lakshman/Mateos criteria):
- BMPCs >20%
- M-protein >2 g/dL
- Serum FLC ratio (FLCr) >20
💎 Pearl: Patients with rising SMM parameters are considered high-risk and should be closely monitored at 3-month intervals. High-risk SMM patients may be candidates for select interventions (daratumumab cat 1, lenalidomide cat 2B).
INITIAL DIAGNOSTIC WORKUP (MYEL-1)
Essential Workup
| Category | Tests |
| History & Physical | Frailty assessment in older adults; H&P exam |
| CBC/Blood | CBC with differential and platelet count; peripheral blood smear |
| Chemistry (for staging) | BUN/Cr, electrolytes, LFTs, albumin, calcium, uric acid, LDH (essential for staging), beta-2 microglobulin (essential for staging) |
| Renal Function | Creatinine clearance (calculated or measured directly) |
| Protein Studies | Serum quantitative immunoglobulins, SPEP, SIFE; 24-h urine total protein, UPEP, UIFE; Serum free light chain (FLC) assay |
| Cardiac | NT-proBNP or BNP (if NT-proBNP not available) |
| Imaging | Whole-body FDG-PET/CT (preferred) or whole-body low-dose CT |
| Bone Marrow | Unilateral BM aspirate and biopsy with IHC and/or multi-parameter flow cytometry |
| FISH Panel | del(13), del(17p13), t(4;14), t(11;14), t(14;16), t(14;20), 1q21 gain/amplification, 1p deletion — CD138+ selected sample STRONGLY recommended |
| Molecular | NGS to assess for TP53 mutation (NEW in v1.2026) |
Useful in Certain Circumstances
- Whole-body MRI without contrast (if FDG-PET/CT or low-dose CT negative → to discern SMM from MM)
- Tissue biopsy to confirm suspected plasmacytoma
- Echocardiogram (cardiac evaluation for amyloidosis)
- Evaluation for light chain amyloidosis if appropriate
- Obtain baseline clonotype identification at diagnosis OR store aspirate sample for future MRD testing by NGS
- Serum viscosity (if hyperviscosity suspected)
- Hepatitis B, Hepatitis C, HIV screening as required
- Assess for circulating plasma cells as clinically indicated
- Renal biopsy if albuminuria or abnormal renal function (NEW v1.2026)
💎 Pearl: LDH and beta-2 microglobulin are ESSENTIAL for R-ISS staging — do not skip these. FISH panel requires CD138+ selected sample for optimal yield.
⚠ Daratumumab and isatuximab-irfc interfere with serologic testing → false-positive indirect Coombs test. TYPE AND SCREEN of RBC must be performed BEFORE initiating these agents.
STAGING & RISK STRATIFICATION (MYEL-B)
International Staging System (ISS)
| ISS Stage | Criteria |
| Stage I | Serum beta-2 microglobulin <3.5 mg/L AND serum albumin ≥3.5 g/dL |
| Stage II | Not Stage I or Stage III |
| Stage III | Serum beta-2 microglobulin ≥5.5 mg/L |
Revised ISS (R-ISS) — Most Clinically Used
| R-ISS Stage | Criteria |
| Stage I | ISS Stage I + standard-risk chromosomal abnormalities by FISH + LDH ≤ ULN |
| Stage II | Not R-ISS Stage I or III |
| Stage III | ISS Stage III + either high-risk chromosomal abnormalities [del(17p), t(4;14), t(14;16)] by FISH OR LDH > ULN |
R2-ISS (Second Revision) — Point-Based System
Each risk factor assigned points based on impact on OS (only validated for NDMM):
| Risk Factor | Points | Risk Category |
| ISS Stage II | +1 | Low risk: 0 pts |
| ISS Stage III | +1.5 | Low-intermediate: 0.5–1 pts |
| del(17p) | +1 | Intermediate-high: 1.5–2.5 pts |
| t(4;14) | +1 | High risk: 3–5 pts |
| 1q+ (gain or amplification) | +0.5 | |
| LDH > ULN | +1 |
IMS-IMWG Definition of High-Risk MM (2025)
High-Risk requires any of:
- del(17p) (>20% of plasma cells) AND/OR TP53 mutation
- One of these translocations co-occurring with 1q+ AND/OR del(1p32): t(4;14), t(14;16), t(14;20)
- Monoallelic del(1p32) along with 1q+ OR biallelic del(1p32)
- High beta-2M (>5.5 mg/dL) with normal creatinine (<1.2 mg/dL)
Cytogenetics — High-Risk Factors (MYEL-B 2 of 2)
Patients with ≥2 of these cytogenetic abnormalities are considered VERY HIGH RISK:
| Newly Diagnosed MM | Relapsed MM — Additional Risk Factors |
| R-ISS III | Disease relapse within 2 yrs of initial therapy (if transplant + maintenance used) |
| Extramedullary disease | Relapse within 18 months if non-transplant-based treatment |
| Circulating plasma cells | Acquisition of 1q gain/amplification and/or del(17p)/TP53 mutation at relapse |
| del(1p32) | Extramedullary disease at relapse and/or circulating plasma cells |
| t(4;14), t(14;16), t(14;20) | |
| del(17p)/monosomy 17/TP53 mutation | |
| 1q21 gain/amplification (≥3 copies; ≥4 copies = amplification) | |
| MYC translocation | |
| High-risk gene expression profile; markers of high proliferation |
💎 Pearl: 1q21 amplification = ≥4 copies by FISH; 1q21 gain = 3 copies. Sole 1q21 abnormality NOT considered a marker for high risk of progression/relapse. Two or more cytogenetic abnormalities = very high risk.
💎 Pearl: Two-drug maintenance is RECOMMENDED for high-risk MM patients.
DIFFERENTIAL DIAGNOSIS
| Condition | Distinguishing Features | Key Differentiator from MM |
| MGUS | M-protein <3 g/dL, BMPCs <10%, no CRAB | No end-organ damage; observation only |
| Smoldering MM | M-protein ≥3 g/dL or BMPCs 10–59%, no CRAB | No myeloma-defining events required for SMM |
| Waldenstrom Macroglobulinemia | IgM M-protein, lymphoplasmacytic lymphoma, hyperviscosity | IgM paraprotein; MYD88 L265P mutation; BM lymphoplasmacytic infiltrate |
| Primary Amyloidosis (AL) | Organ dysfunction from amyloid deposition (kidneys, heart, liver) | Biopsy shows amyloid deposits; NT-proBNP elevated |
| Metastatic Bone Disease | Lytic lesions without M-protein | No M-protein; primary solid tumor found |
| Plasmablastic Lymphoma | EBV-related; aggressive B-cell lymphoma | No BM plasma cells; EBV-positive |
| CLL/SLL | Lymphocytosis, lymphadenopathy | Flow cytometry; no M-protein spike |
| Reactive Plasmacytosis | Increased plasma cells from infection/inflammation | BMPCs <10%; no M-protein; polyclonal immunoglobulins |
IMAGING PRINCIPLES (MYEL-C)
Initial Diagnostic Workup
- Whole-body FDG-PET/CT (PREFERRED) OR whole-body low-dose CT — standard for initial workup
- If PET/CT or low-dose CT NEGATIVE → consider whole-body MRI without contrast to discern SMM from MM
- Skeletal survey acceptable in certain circumstances only
Solitary Plasmacytoma Imaging
- Extraosseous plasmacytoma: Whole-body FDG-PET/CT is FIRST choice (initial AND follow-up)
- Osseous plasmacytoma: Whole-body MRI preferred; FDG-PET/CT if MRI not available
- Yearly follow-up imaging for at least 5 years with same technique used at diagnosis
- Risk of progression to MM: 14–38% within first 3 years
Follow-up of MM & SMM
- Advanced whole-body imaging (FDG-PET/CT, low-dose CT, MRI without contrast) annually or as clinically indicated
- Use same imaging technique throughout follow-up for comparison
- Residual focal lesions on PET/CT or MRI = adverse prognostic significance
- Patients without measurable M-protein or FLC → follow with imaging at regular intervals
- Whole-body FDG-PET/CT recommended ~Day 100 after autologous HCT (new footnote, v1.2026)
💎 Pearl: DEXA scans are NOT useful to assess myeloma bone disease. Use PET/CT or low-dose CT instead.
RESPONSE CRITERIA — IMWG (MYEL-E)
| Response Category | Criteria |
| Sustained MRD-Negative | MRD-negative by NGF or NGS + imaging, confirmed ≥1 year apart |
| Imaging + MRD-Negative | MRD-negative by NGF/NGS + disappearance of all FDG-PET/CT uptake or <mediastinal blood pool SUV |
| Stringent CR (sCR) | CR + normal FLC ratio + absence of clonal cells in BM biopsy by IHC (κ/λ ratio ≤4:1 or ≥1:2, counting ≥100 plasma cells) |
| Complete Response (CR) | Negative immunofixation in serum AND urine + disappearance of soft tissue plasmacytomas + <5% plasma cells in BM aspirate |
| VGPR | M-protein detectable by immunofixation but NOT on electrophoresis OR ≥90% reduction in serum M-protein + urine M-protein <100 mg/24h |
| PR | ≥50% reduction of serum M-protein + ≥90% reduction in 24-h urinary M-protein or to <200 mg/24h |
| Minimal Response (MR) | ≥25% but ≤49% reduction of serum M-protein + 50–89% reduction in 24-h urine M-protein |
| Stable Disease (SD) | Not meeting criteria for CR, VGPR, PR, MR, or PD |
| Progressive Disease (PD) | ≥25% increase from lowest confirmed value in serum M-protein (absolute ≥0.5 g/dL) OR urine M-protein (absolute ≥200 mg/24h) OR new/enlarging lesions OR ≥50% increase in circulating plasma cells |
MRD Testing Notes
- Flow MRD-negative: absence of aberrant clonal PCs by NGF with sensitivity ≥1 in 10⁵ nucleated cells
- Sequencing MRD-negative: absence of clonal PCs by NGS with sensitivity ≥1 in 10⁵ nucleated cells
- MRD testing initiated only at time of suspected complete response
- All response categories require 2 consecutive assessments before starting new therapy (except MRD — no confirmation needed)
💎 Pearl: IgG kappa monoclonal antibodies (daratumumab, isatuximab) can produce FALSE-POSITIVE immunofixation or M-protein — the therapeutic antibody band can be mistaken for the patient’s M-protein. Use special interference testing or mass spectrometry to differentiate.
PHARMACOTHERAPY — PRIMARY THERAPY (MYEL-G)
⚠ QUADRUPLET regimen is PREFERRED for ALL newly diagnosed MM patients (HCT-eligible and ineligible). Based on functional status, may start with 2- or 3-drug regimen with additional drugs added as PS improves.
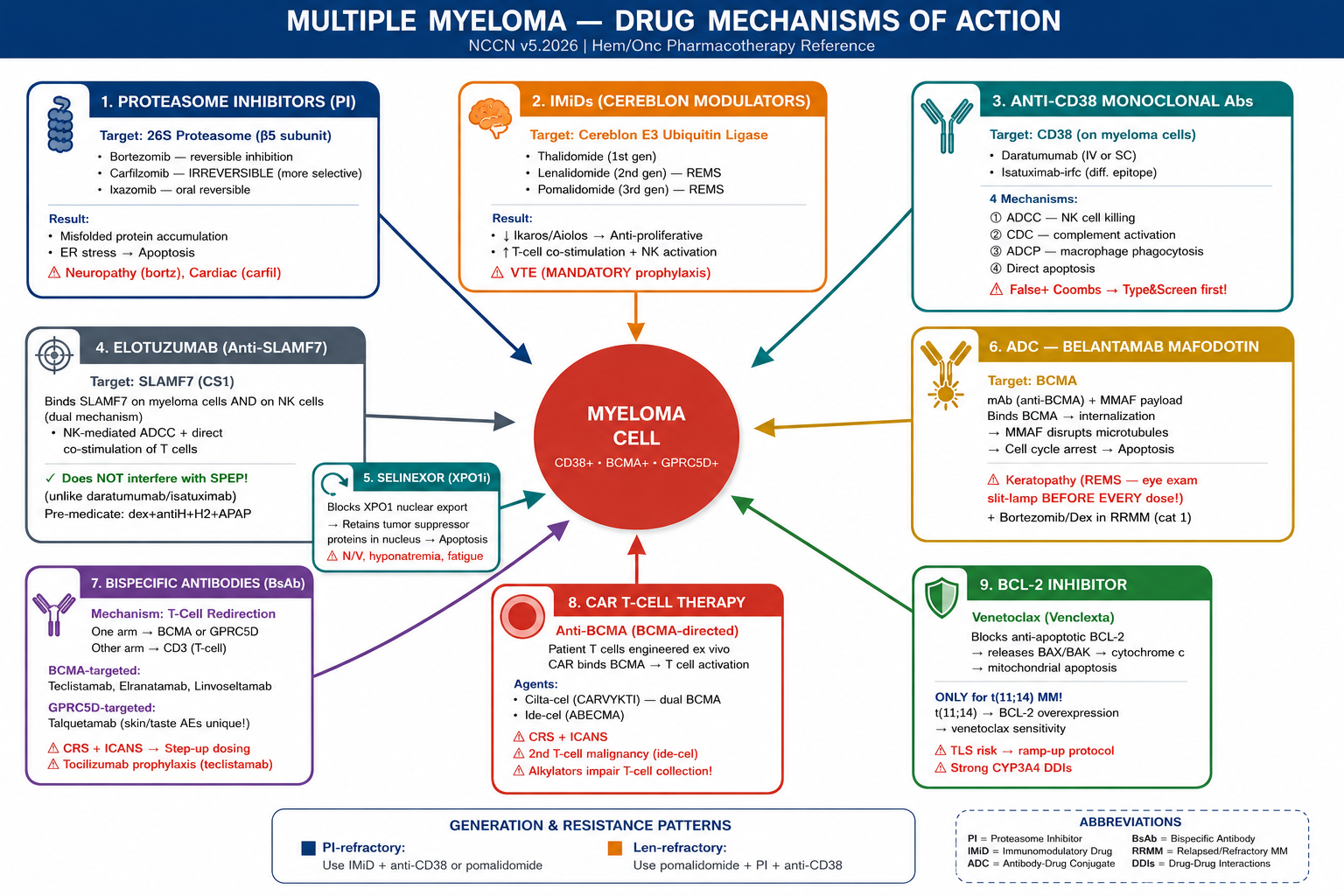
Clinical Pearl — MOA Quick Reference
- PIs (bortezomib, carfilzomib, ixazomib): block protein degradation → ER stress → apoptosis. SC bortezomib = less neuropathy.
- IMiDs (lenalidomide, pomalidomide): target cereblon → degrade Ikaros/Aiolos → anti-proliferative + immune stimulation. REMS mandatory.
- Anti-CD38 (daratumumab, isatuximab): 4 mechanisms — ADCC, CDC, ADCP, T-cell activation. Must type & screen BEFORE use.
- BsAbs (teclistamab, elranatamab, talquetamab, linvoseltamab): redirect patient T cells to kill myeloma. Step-up dosing mandatory.
- CAR-T (cilta-cel, ide-cel): patient T cells engineered to express BCMA-targeting receptor. Manufacturing takes 4–6 weeks.
- Venetoclax: BCL-2 inhibitor — ONLY active in t(11;14) MM where BCL-2 is overexpressed. TLS protocol required.
💎 Pearl: Talquetamab targets GPRC5D — not BCMA. Unique AEs: skin/nail toxicity, dysgeusia. Can be used as bridge to BCMA CAR-T per NCCN v5.2026.
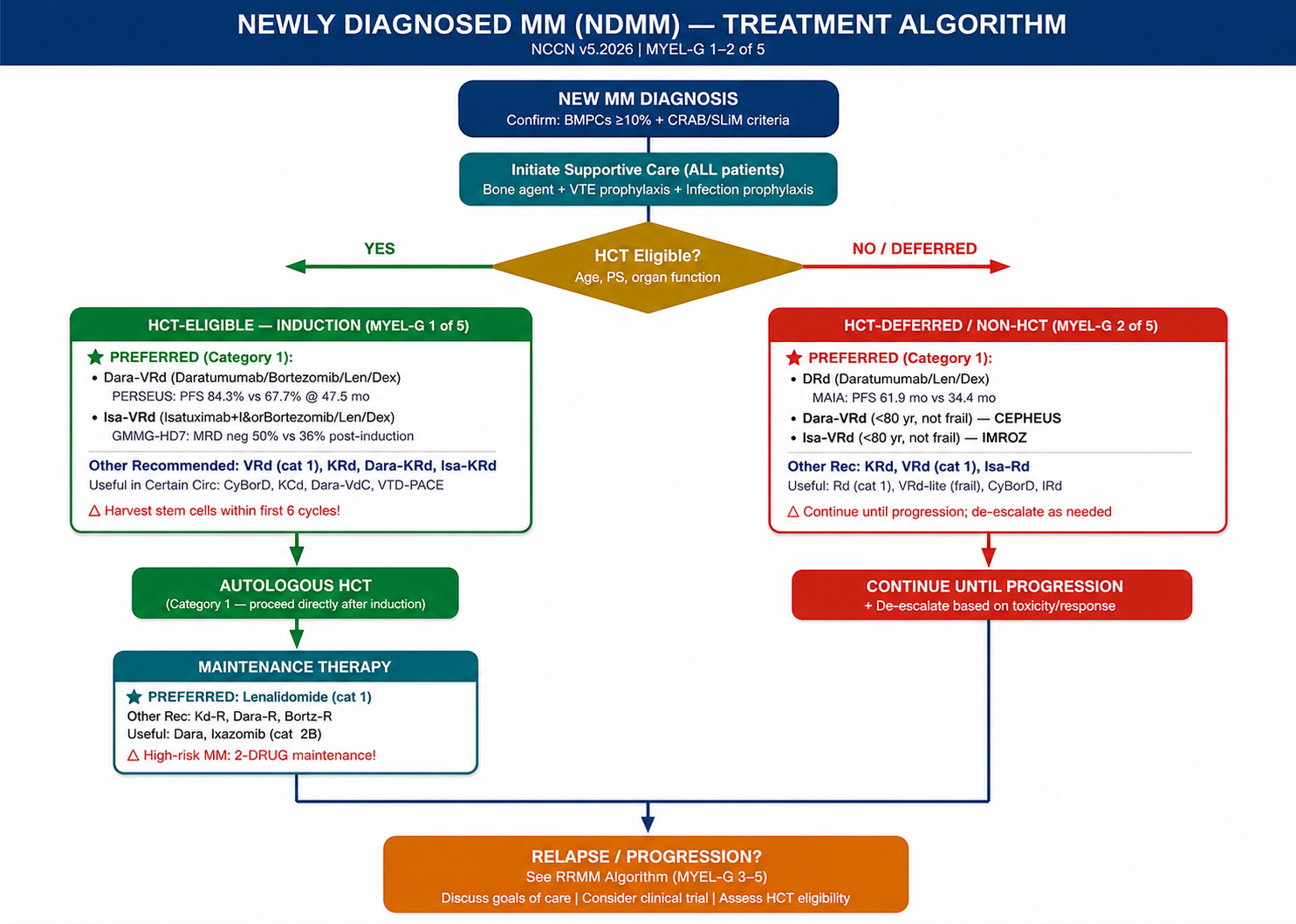
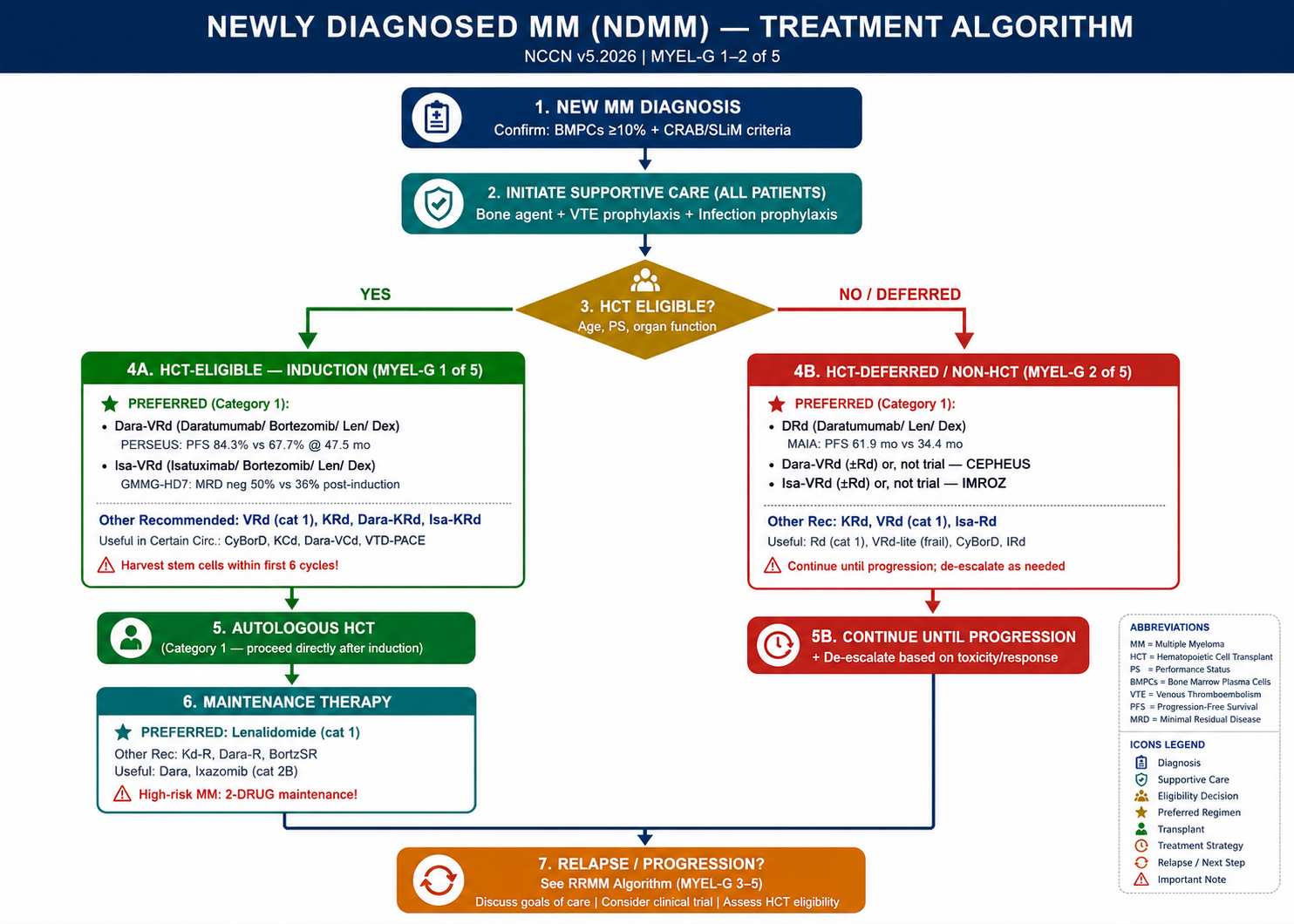
A. Primary Therapy — HCT Candidates (MYEL-G 1 of 5)
PREFERRED (Category 1)
| Regimen | Category | Key Trial / Notes |
| Daratumumab/Bortezomib/Lenalidomide/Dexamethasone (Dara-VRd) | 1 | PERSEUS trial: PFS rate 84.3% vs 67.7% (VRd) at 47.5 mo; 58% reduction in risk of progression/death |
| Isatuximab-irfc/Bortezomib/Lenalidomide/Dexamethasone (Isa-VRd) | 1 | GMMG-HD7: deeper MRD negativity (50% vs 36% after induction); PFS HR 0.70 at 4-yr follow-up |
Other Recommended
| Regimen | Category | Notes |
| Bortezomib/Lenalidomide/Dexamethasone (VRd) | 1 | SWOG S0777: PFS 43 vs 30 mo; OS 75 vs 64 mo vs Rd |
| Carfilzomib/Lenalidomide/Dexamethasone (KRd) | 2A | ENDURANCE: similar PFS to VRd; less neuropathy but more cardiac/pulmonary/renal toxicity |
| Daratumumab/Carfilzomib/Lenalidomide/Dexamethasone (Dara-KRd) | 2A | MASTER trial: MRD <10⁻⁵ in 81% (no HRCA); 36-mo PFS 88% (no HRCA) |
| Isatuximab-irfc/Carfilzomib/Lenalidomide/Dexamethasone (Isa-KRd) | 2A | IsKia trial: MRD neg 77% vs 67% (KRd) after consolidation |
Useful in Certain Circumstances
- Bortezomib/Cyclophosphamide/Dexamethasone (CyBorD) — renal insufficiency, no access to PI/lenalidomide
- Carfilzomib/Cyclophosphamide/Dexamethasone — renal insufficiency and/or peripheral neuropathy
- Daratumumab/Bortezomib/Cyclophosphamide/Dexamethasone — renal insufficiency; no access to dara-VRd
- VTD-PACE (Dara/Bortezomib/Thalidomide/Cisplatin/Doxorubicin/Cyclophosphamide/Etoposide) — aggressive MM, extramedullary disease, plasma cell leukemia
B. Maintenance Therapy Post-HCT (MYEL-G 1 of 5)
| Regimen | Category | Notes |
| Lenalidomide (PREFERRED) | 1 | Increased risk of secondary cancers (especially with lenalidomide post-transplant) — discuss risk/benefit with patient |
| Carfilzomib/Lenalidomide | 2A | Other recommended option |
| Daratumumab/Lenalidomide | 2A | Used in PERSEUS trial maintenance; consider in dara-VRd responders |
| Bortezomib ± Lenalidomide | 2A | Useful in certain circumstances; preferred for high-risk MM (2-drug maintenance) |
| Daratumumab | 2A | Useful in certain circumstances (new in v1.2026) |
| Ixazomib | 2B | All-oral option; convenient for patients unable to travel |
⚠ Two-drug maintenance is recommended for HIGH-RISK MM. Consider dara + lenalidomide or bortezomib + lenalidomide.
C. Primary Therapy — HCT-Deferred or Non-HCT Candidates (MYEL-G 2 of 5)
In general, continue primary therapy UNTIL PROGRESSION with de-escalation as needed.
PREFERRED
| Regimen | Category | Key Trial / Notes |
| Daratumumab/Lenalidomide/Dexamethasone (DRd) | 1 | MAIA: median PFS 61.9 mo vs 34.4 mo (Rd); OS benefit demonstrated |
| Dara-VRd (patients <80 yr, not frail) | 1 | CEPHEUS: MRD neg 60.9% vs 39.4%; PFS HR 0.57 |
| Isa-VRd (patients <80 yr, not frail) | 1 | IMROZ: PFS 63.2% vs 45.2% at 5 yr; 40% reduction in risk of progression/death |
Other Recommended
- Carfilzomib/Lenalidomide/Dexamethasone (KRd) — Category 2A
- Bortezomib/Lenalidomide/Dexamethasone (VRd) — Category 1
- Isatuximab-irfc/Lenalidomide/Dexamethasone (Isa-Rd) — Category 2A (good option if peripheral neuropathy)
Useful in Certain Circumstances
- Lenalidomide/Low-dose Dexamethasone (Rd) — Category 1; for frail/elderly; FIRST trial
- VRd-lite — Category 2A; for frail patients (lenalidomide 15 mg days 1–21; bortezomib 1.3 mg/m² weekly SC; dex 20 mg day of and day after bortz)
- Bortezomib/Cyclophosphamide/Dexamethasone — renal insufficiency; no access to PI/Rd
- Ixazomib/Lenalidomide/Dexamethasone — all-oral; for patients with logistical constraints; TOURMALINE-MM2 (did not meet primary endpoint)
- Daratumumab/Cyclophosphamide/Bortezomib/Dexamethasone — renal insufficiency/AKI
💎 Pearl: Strongly consider collecting and storing stem cells for future HCT in non-HCT candidates receiving primary therapy — within first 6 cycles, before prolonged lenalidomide or daratumumab exposure.
RELAPSED/REFRACTORY MM — THERAPY (MYEL-G 3–5 of 5)
⚠ For RRMM: use drugs/drug classes NOT previously exposed to, or not exposed to for at least 6 months. Agents/regimens may be reconsidered if relapse ≥6 months after stopping therapy.
A. After 1–3 Prior Therapies — Preferred Regimens
Anti-CD38 Refractory
| Regimen | Category | Notes |
| Carfilzomib/Lenalidomide/Dexamethasone (KRd) | 1 | ASPIRE trial |
| Carfilzomib/Pomalidomide/Dexamethasone | 2A | |
| Pomalidomide/Bortezomib/Dexamethasone (PVd) | 1 | |
| Elotuzumab/Pomalidomide/Dexamethasone (after 2 prior, incl Len + PI) | 2A | |
| Ixazomib/Pomalidomide/Dexamethasone (after 2 prior IMiD+PI, PD within 60d) | 2A |
Bortezomib-Refractory
| Regimen | Category | Notes |
| KRd | 1 | |
| Daratumumab/Carfilzomib/Dexamethasone (DKd) | 1 | CANDOR trial |
| Daratumumab/Lenalidomide/Dexamethasone (DRd) | 1 | POLLUX trial |
| Isatuximab-irfc/Carfilzomib/Dexamethasone (IsaKd) | 1 | IKEMA trial |
| Daratumumab/Pomalidomide/Dexamethasone (DPd) — after 1 prior (Len+PI) | 1 | APOLLO/EQUULEUS trial |
| Daratumumab/Teclistamab-cqyv — after 1 prior (Len+PI) | 1 | NEW in v5.2026; BsAb combination |
| Isatuximab-irfc/Pomalidomide/Dex (after 2 prior Len+PI) | 1 | IKEMA data |
Lenalidomide-Refractory
| Regimen | Category | Notes |
| Daratumumab/Bortezomib/Dexamethasone (DVd) | 1 | CASTOR trial |
| Daratumumab/Carfilzomib/Dexamethasone (DKd) | 1 | |
| Isatuximab-irfc/Carfilzomib/Dexamethasone | 1 | |
| Pomalidomide/Bortezomib/Dexamethasone | 1 | |
| Daratumumab/Pomalidomide/Dex (after 1 prior Len+PI) | 1 | |
| Daratumumab/Teclistamab-cqyv (after 1 prior Len+PI) | 1 | NEW in v5.2026 |
| Isatuximab-irfc/Pomalidomide/Dex (after 2 prior Len+PI) | 1 |
CAR T-Cell Therapy (After 1–3 Prior Lines)
| Agent | Category | Indication |
| Ciltacabtagene autoleucel (Cilta-cel, CARVYKTI) | 1 | After ≥1 prior line including IMiD + PI, AND refractory to lenalidomide |
| Idecabtagene vicleucel (Ide-cel, ABECMA) | 1 | After ≥2 prior lines including IMiD + anti-CD38 mAb + PI |
10B. After ≥3 Prior Lines of Therapy — Preferred
CAR T-Cell Therapy (Preferred)
- Ciltacabtagene autoleucel OR Idecabtagene vicleucel
Bispecific Antibodies (BsAb) — After ≥4 Prior Lines (anti-CD38 + PI + IMiD)
| Agent (Brand) | Target | Notes |
| Elranatamab-bcmm (Elrexfio) | BCMA × CD3 | |
| Linvoseltamab-gcpt (Lynozyfic) | BCMA × CD3 | NEW in v2.2026 |
| Talquetamab-tgvs (Talvey) | GPRC5D × CD3 | May be used as bridge to BCMA CAR-T (new footnote v5.2026) |
| Teclistamab-cqyv (Tecvayli) | BCMA × CD3 | Prophylactic tocilizumab may be considered prior to 1st dose to reduce CRS risk |
Other Recommended (After ≥3 Prior Lines)
- High-dose or fractionated cyclophosphamide
- Selinexor/Dexamethasone — after ≥4 prior lines, refractory to ≥2 PIs, ≥2 IMiDs, anti-CD38 mAb
Useful in Certain Circumstances (After ≥3 Prior Lines)
- Belantamab mafodotin-blmf (as available through expanded access program; v5.2026)
- Bendamustine (alone or + bortezomib/carfilzomib/lenalidomide with dex) — NOTE: bendamustine and alkylating agents can impair T-cell collection for CAR T
- Talquetamab + Teclistamab combination
Other Recommended — After 1–3 Prior Lines
- Elotuzumab/Lenalidomide/Dexamethasone (cat 1); Ixazomib/Lenalidomide/Dexamethasone (cat 1)
- Selinexor/Bortezomib/Dexamethasone (cat 1) — XVd; Bortezomib/Cyclophosphamide/Dexamethasone
- Venetoclax/Dexamethasone ± Daratumumab or PI — ONLY for t(11;14) patients
- Belantamab mafodotin-blmf/Bortezomib/Dexamethasone (cat 1) — after 2 prior therapies including IMiD and PI (v3.2026)
💎 Pearl: Patients can receive more than one BCMA-targeted therapy. However, optimal sequencing of sequential BCMA-directed therapies is unknown; immediate follow-on BCMA therapy after relapse may be associated with lower response rates.
⚠ Alkylating agents (bendamustine, cyclophosphamide) can impair the ability to collect T cells for CAR T-cell therapy. Plan carefully before using these agents in potential CAR T candidates.
11. KEY CLINICAL TRIALS — BRIEF SUMMARY
| Trial | Population | Intervention | Comparator | Key Results |
| PERSEUS | NDMM, HCT-eligible (n=709) | Dara-VRd → ASCT → Dara-R maintenance | VRd → ASCT → R maintenance | PFS 84.3% vs 67.7% at 47.5 mo; HR 0.42; MRD neg 75% vs 48% |
| GRIFFIN | NDMM, HCT-eligible | Dara-VRd | VRd | sCR 67% vs 48%; 4-yr PFS 87.2% vs 70% |
| GMMG-HD7 | NDMM, HCT-eligible (n=660) | Isa-VRd (3 cycles) → HCT | VRd (3 cycles) → HCT | MRD neg 50% vs 36% post-induction; PFS HR 0.70 at 4 yr |
| MAIA | NDMM, HCT-ineligible (n=737) | DRd (continuous) | Rd (continuous) | Median PFS 61.9 mo vs 34.4 mo; OS benefit confirmed |
| CEPHEUS | NDMM, HCT-deferred or not planned, <80 yr, not frail (n=395) | Dara-VRd → Dara-R maintenance | VRd → R maintenance | MRD neg 60.9% vs 39.4%; PFS HR 0.57 |
| IMROZ | NDMM, HCT-ineligible, ≤80 yr (n=446) | Isa-VRd (4 cycles) → Isa-Rd continuous | VRd → Rd continuous | PFS 63.2% vs 45.2% at 5 yr; HR 0.60; CR+ 74.7% vs 64.1% |
| SWOG S0777 | NDMM (n=525), no intent to transplant immediately | VRd × 6 cycles → Rd maintenance | Rd × 6 cycles → Rd maintenance | PFS 43 vs 30 mo; OS 75 vs 64 mo |
| ENDURANCE | NDMM (n=1053) — excluded t(4;14) and other HR | KRd | VRd | Similar PFS; less neuropathy with KRd but more cardiac/renal/pulmonary toxicity |
| POLLUX | RRMM (1–3 prior), n=569 | DRd | Rd | PFS HR 0.37; ORR 92% vs 76% |
| CASTOR | RRMM (1–3 prior), n=498 | DVd | Vd | PFS HR 0.31; ORR 83% vs 63% |
| CANDOR | RRMM (1–3 prior), n=466 | DKd | Kd | Median PFS 28.6 vs 15.2 mo; HR 0.59 |
| IKEMA | RRMM (1–3 prior), n=302 | IsaKd | Kd | PFS HR 0.53; MRD neg 29.6% vs 13.0% |
| APOLLO | RRMM (1–3 prior), n=304 | DPd | Pd | PFS HR 0.63; ORR 69% vs 46% |
| MAJESTIC-1 / MajesTEC-1 | RRMM (≥3 prior), n=165 | Teclistamab 1.5 mg/kg SC QW | Single arm | ORR 63%; median PFS 11.3 mo; most common AE: CRS 72% |
12. DRUG DOSING, ADJUSTMENTS & PHARMACIST REFERENCE
12A. Drug Class Overview & Key Dosing
| Drug (Brand) | Class | Standard Dose | Route | Key Monitoring / Dose Adj |
| BORTEZOMIB (Velcade) | PI (1st gen) | 1.3 mg/m² D1,8,15,22 (weekly preferred) or D1,4,8,11 (twice-weekly) | SC (preferred) or IV | Peripheral neuropathy (grade ≥2 → dose reduce or hold); CBC; LFTs; hold if platelets <25k |
| CARFILZOMIB (Kyprolis) | PI (2nd gen) | Weekly: 70 mg/m² D1,8,15 (28-day); or 20→27 mg/m² D1,2,8,9,15,16 (twice-weekly) | IV | Cardiac (HTN, CHF, MI — monitor BP each infusion); pulmonary; renal; CBC; Cycle 1 Day 1: 20 mg/m² only (ramp up) |
| IXAZOMIB (Ninlaro) | PI (oral, 3rd gen) | 4 mg PO D1,8,15 of 28-day cycle | PO | GI (N/V/D); peripheral neuropathy; rash; avoid high-fat meals (take ≥1h before or 2h after food) |
| LENALIDOMIDE (Revlimid) | IMiD (2nd gen) | Induction: 25 mg PO D1–21 of 28-day cycle; Maintenance: 10–15 mg PO D1–21 | PO | CBC, SCr (REMS required — RiskMAP); VTE prophylaxis MANDATORY; renal dose adjust (see below); secondary malignancy risk |
| POMALIDOMIDE (Pomalyst) | IMiD (3rd gen) | 4 mg PO D1–21 of 28-day cycle | PO | Myelosuppression; VTE prophylaxis; REMS program; no renal dose adjustment needed (unlike lenalidomide); hold if ANC <0.5 or platelets <25k |
| THALIDOMIDE (Thalomid) | IMiD (1st gen) | 50–200 mg PO QHS | PO | Sedation, constipation, DVT, peripheral neuropathy; REMS; teratogenic; VTE prophylaxis |
| DARATUMUMAB (Darzalex) | Anti-CD38 mAb | 16 mg/kg IV weekly × 8, then biweekly × 8, then monthly | IV | Infusion reactions (pre-medicate: dex + acetaminophen + antihistamine); false+ indirect Coombs; type & screen BEFORE starting; VZV prophylaxis; hypogammaglobulinemia |
| DARATUMUMAB SC (Darzalex Faspro) | Anti-CD38 mAb | 1800 mg SC flat dose (with hyaluronidase); Q-weekly/biweekly/monthly | SC | Same AEs as IV but FEWER infusion reactions; ~5 min administration; different dosing than IV formulation; caution in significant thrombocytopenia |
| ISATUXIMAB-IRFC (Sarclisa) | Anti-CD38 mAb | 10 mg/kg IV on D1,8,15,22 (cycle 1), then D1,15 (cycles 2+) | IV | Infusion reactions (pre-medicate); false+ indirect Coombs; type & screen BEFORE starting; different dosing schedule than daratumumab |
| ELOTUZUMAB (Empliciti) | Anti-SLAMF7 mAb | 10 mg/kg IV D1,8,15,22 (cycles 1–2); 10 mg/kg D1,15 (cycles 3+) OR 20 mg/kg D1 Q4W | IV | Infusion reactions; pre-medicate (dex+antihistamine+H2 blocker+acetaminophen); lymphopenia; does NOT interfere with SPEP/immunofixation |
| DEXAMETHASONE | Corticosteroid | 40 mg PO/IV weekly (standard); 20 mg weekly for older/frail patients | PO / IV | Hyperglycemia (monitor glucose); infection risk; fluid retention; GI (take with food); mood changes; consider taper in elderly; REDUCE TO 20 mg/weekly in older adults and discontinue at earliest possible timepoint |
| TECLISTAMAB-CQYV (Tecvayli) | BsAb BCMA×CD3 | Step-up: 0.06 mg/kg SC D1, 0.3 mg/kg SC D4, then 1.5 mg/kg SC QW | SC | CRS (most common 72%, grade 3-4 ~1%); ICANS; infections (levofloxacin + PJP prophylaxis); cytopenias; consider prophylactic tocilizumab prior to 1st dose |
| ELRANATAMAB-BCMM (Elrexfio) | BsAb BCMA×CD3 | Step-up: 12 mg SC D1, 32 mg SC D4, then 76 mg SC QW × 24 wks, then Q2W if ≥PR | SC | CRS; ICANS; infections; consider step-up dosing hospitalization for monitoring |
| TALQUETAMAB-TGVS (Talvey) | BsAb GPRC5D×CD3 | Step-up: 0.01 mg/kg SC D1, 0.06 mg/kg D4, then 0.4 mg/kg QW or 0.8 mg/kg Q2W | SC | CRS; skin toxicity (rash, nail changes, dryness — unique to GPRC5D target); dysgeusia; weight loss; cytokine release |
| LINVOSELTAMAB-GCPT (Lynozyfic) | BsAb BCMA×CD3 | Step-up dosing; 200 mg SC QW × 24 wks then Q4W if ≥VGPR | SC | CRS; infections; cytopenias; NEW in v2.2026 |
| CILTACABTAGENE autoleucel (CARVYKTI) | CAR T (BCMA) | One-time infusion: 0.5–1.0 × 10⁶ CAR+ T cells/kg IV | IV | CRS (within 7 days); ICANS; prolonged cytopenias; infections; REMS; manufacturing time 4–6 wks; leukapheresis required |
| IDECABTAGENE vicleucel (ABECMA) | CAR T (BCMA) | One-time infusion: 300–460 × 10⁶ CAR+ T cells IV | IV | CRS; ICANS; prolonged cytopenias; secondary T-cell malignancy risk (boxed warning); REMS |
| SELINEXOR (Xpovio) | XPO1 inhibitor | 80 mg PO BIW (with bortezomib); or 100 mg PO weekly (with dex) | PO | Nausea/vomiting (use ondansetron or olanzapine prophylactically); anorexia; weight loss; hyponatremia; thrombocytopenia; fatigue |
| VENETOCLAX (Venclexta) | BCL-2 inhibitor | 400 mg PO daily (ramp up per protocol) with PI/dex | PO | ONLY for t(11;14) patients; tumor lysis syndrome (TLS) prophylaxis mandatory; ramp-up dosing; avoid strong CYP3A4 inhibitors |
| BELANTAMAB MAFODOTIN-BLMF (Blenrep) | ADC (BCMA) | 2.5 mg/kg IV Q21 days (in combination with bortezomib/dex) | IV | Corneal epithelial changes/keratopathy (eye exam REQUIRED before each dose — REMS); blurred vision; dry eyes; thrombocytopenia; BCMA ADC |
12B. Lenalidomide Renal Dose Adjustments (MYEL-L)
⚠ Lenalidomide is primarily renally cleared — MUST dose-adjust for renal impairment using Cockcroft-Gault CrCl.
| Renal Function (CG CrCl) | Lenalidomide Dose | Notes |
| Normal (≥60 mL/min) | 25 mg D1–21 of 28-day cycle | Full dose |
| Moderate (≥30 to <60 mL/min) | 10 mg every 24 hours | Reduce dose |
| Severe (<30 mL/min, not on dialysis) | 15 mg every 48 hours | Further reduction |
| ESRD (<30 mL/min, requiring dialysis) | 5 mg once daily; on dialysis days — administer AFTER dialysis | Dose after HD session |
12C. Bone-Modifying Agent Dosing in Renal Impairment (MYEL-L)
| Renal Impairment | Pamidronate (Aredia) | Zoledronic Acid (Zometa) | Denosumab (Xgeva) |
| None (normal) | 90 mg IV Q3–4 wks | 4 mg IV Q1–3 months | 120 mg SC Q4 wks |
| Mild/Moderate | Standard dose (but use with caution — focal segmental glomerulosclerosis risk) | Reduce dose (per package insert) | 120 mg SC Q4 wks |
| Severe (CrCl <30 mL/min) | 60–90 mg (caution) | NOT RECOMMENDED | 120 mg SC Q4 wks (monitor Ca²⁺ closely — risk of severe hypocalcemia) |
⚠ Zoledronic acid is NOT recommended in severe renal impairment. Denosumab is PREFERRED in renal insufficiency but carries risk of severe hypocalcemia — monitor calcium levels closely. Do NOT forget vitamin D supplementation.
12D. Considerations for Myeloma Therapy — General (MYEL-F)
- Subcutaneous bortezomib is the PREFERRED method of administration (less neurotoxicity than IV)
- Weekly bortezomib PREFERRED over twice-weekly (similar efficacy, less grade 3/4 toxicity, less neuropathy)
- Carfilzomib: weekly (PREFERRED) or twice-weekly; note Cycle 1 Day 1 ramp-up dose required (20 mg/m²)
- Daratumumab IV or SC (Darzalex Faspro 1800 mg flat dose) may be used in any dara-containing regimen
- Reduce dexamethasone to 20 mg weekly in older/frail patients; discontinue at earliest possible timepoint
- Consider biosimilars as appropriate substitutes for any recommended systemic biologic therapy
- Limit myelotoxic agents (alkylators, nitrosoureas) in potential HCT candidates to preserve stem cell reserve
- Harvest stem cells within first 6 cycles BEFORE prolonged lenalidomide or daratumumab exposure
💎 Pearl: Subcutaneous bortezomib SIGNIFICANTLY reduces peripheral neuropathy risk versus IV — MMY-3021 trial. Always use SC route unless contraindicated.
💎 Pearl: Ixazomib may be substituted for bortezomib or carfilzomib in select patients for logistical reasons (all-oral), intolerance, or patient preference — discuss on case-by-case basis.
13. SUPPORTIVE CARE (MYEL-I)
13A. Bone Disease
⚠ ALL patients receiving primary myeloma therapy should receive bone-targeting treatment (bisphosphonates [cat 1] or denosumab) — do not skip this.
- Baseline dental exam STRONGLY RECOMMENDED before starting bone-targeting therapy
- Assess vitamin D status (supplement if deficient)
- Monitor renal function with bisphosphonate therapy
- Monitor for osteonecrosis of the jaw (ONJ) — dental hygiene counseling essential
- Continue bone-targeting treatment for up to 2 years; beyond 2 years based on clinical judgment
- Monthly vs. Q3 months dosing frequency depends on individual patient criteria, response, and agent used
- If denosumab discontinued → give maintenance denosumab Q6 months OR single dose bisphosphonate to prevent rebound osteoporosis
- DEXA scans are NOT useful to assess myeloma bone disease
- Consider vertebroplasty or kyphoplasty for symptomatic vertebral compression fractures
- Orthopedic consultation for impending or actual long-bone fractures or spinal cord compression/instability
13B. Hypercalcemia Management
- IV hydration (first-line, urgent)
- Bisphosphonates: zoledronic acid 4 mg IV PREFERRED (onset 2–4 days)
- Denosumab 120 mg SC (alternative, especially in renal impairment)
- Calcitonin 4–8 units/kg IM/SC Q6–12h (fastest onset, tolerance develops within 48–72h)
- Corticosteroids (dexamethasone/prednisone) — useful in myeloma-related hypercalcemia
- Furosemide (only after adequate hydration; helps excretion)
13C. Hyperviscosity
- Plasmapheresis as ADJUNCTIVE therapy for symptomatic hyperviscosity — initiate systemic therapy concurrently
- Most commonly with IgM myeloma (Waldenström) but can occur in IgA, IgG3 subtypes
13D. Anemia
- See NCCN Guidelines for Hematopoietic Growth Factors
- Consider erythropoiesis-stimulating agents (ESAs) — INCREASED VTE RISK with ESAs in MM patients on IMiD-based therapy
- Transfusion support as needed
13E. Peripheral Neuropathy (Treatment-Related)
Bortezomib-induced neuropathy grading guide:
| Grade | Description | Bortezomib Dose Modification |
| Grade 1 | Asymptomatic, loss of reflexes, paresthesia — no pain | Continue without modification; consider switch to SC |
| Grade 2 | Moderate symptoms, limiting instrumental ADL | Reduce bortezomib by 1 dose level (1.3→1.0→0.7 mg/m²) |
| Grade 3 | Severe symptoms, limiting self-care ADL | Hold until resolved ≤Grade 1, restart at reduced dose |
| Grade 4 | Life-threatening, urgent intervention indicated | DISCONTINUE bortezomib |
14. INFECTION PROPHYLAXIS & MANAGEMENT (MYEL-J)
14A. Bacterial Infection Prophylaxis
| Intervention | Dose | Indication & Duration |
| Levofloxacin | 500 mg PO daily (alt: Cefdinir 300 mg PO BID or Augmentin 875 mg PO BID) | CAR-T or BsAb: start when ANC <500 or per clinician discretion → until neutrophil recovery; AutoHCT: same; NDMM (newly diagnosed): consider for 12 weeks after diagnosis |
| Immunoglobulin (IVIG) replacement | Per IgG level | CAR-T: regular IVIG based on clinical context; BsAb: consider for duration of therapy; Other: IgG <400 mg/dL AND/OR recurrent life-threatening infections |
| Pneumococcal vaccination | 1 dose PCV20 OR PCV15 then PPSV23 ≥1 yr later (CDC) | Revaccination 3–6 months after CAR-T or AutoHCT; update status before BsAb therapy |
⚠ To estimate NORMAL IgG in IgG myeloma patients: subtract the M-spike value from total IgG. If the corrected IgG <400 mg/dL (not polyclonal), replacement can be considered.
14B. Viral Prophylaxis
| Infection | Agent & Dose | Duration |
| HSV/VZV (Shingles) | Acyclovir 400–800 mg PO BID OR Valacyclovir 500 mg PO QD–BID | CAR-T: minimum 1 year; indefinite preferred. BsAb: indefinite. AutoHCT: 1 year post-HCT. PI or mAb regimens: while on therapy + 3 months after OR per institutional practice |
| COVID-19 | Vaccination per CDC | Stay up to date with current recommendations; consult NCCN guidelines for cancer-related infections |
| Influenza | Annual influenza vaccination | Per CDC for immunosuppressed patients |
| RSV | Single dose bivalent vaccine | For MM patients ≥60 years old |
| CMV | Monitor viral load by PCR only if symptomatic or high risk | See NCCN guidelines for treatment indication |
14C. Fungal Prophylaxis
| Infection | Agent & Dose | Duration |
| PJP (Pneumocystis jirovecii) | TMP-SMX (preferred) or pentamidine or atovaquone | CAR-T and BsAb: start with therapy and continue ≥6 months after infusion OR until CD4 ≥200/mm³ (whichever is longer); Other: when dexamethasone equivalent >40 mg/day for 4 days/week |
| Yeast | Fluconazole 400 mg PO daily | CAR-T and BsAb (high-risk): when ANC <500 or per clinician discretion → until neutrophil recovery |
| Mold | Anti-mold azole (voriconazole/posaconazole) | High-risk patients: consider ongoing prophylaxis; CAR-T and BsAb high-risk patients |
💎 Pearl: High-risk for infection: patients on CAR-T or BsAb receiving >1 dose of tocilizumab; use of anakinra or siltuximab for CRS/ICANS; prolonged/high-dose steroids (>3 days of dex 10 mg/day in 7-day period or methylprednisolone >1 g/day).
15. VTE PROPHYLAXIS & MANAGEMENT (MYEL-K)
15A. Risk Stratification Scores
IMPEDE Score
| Risk Factor | Points | Category |
| Previous VTE | +5 | |
| IMiD (any) | +4 | |
| Pelvic/hip/femur fracture | +4 | |
| Dexamethasone >160 mg/month | +4 | |
| Doxorubicin or multiagent chemo | +3 | |
| Central venous catheter / tunneled central line | +2 | |
| Dexamethasone ≤160 mg/month | +2 | |
| Obesity (BMI ≥25) | +1 | |
| ESA use | +1 | |
| Asian/Pacific Islander race | -3 | Protective |
| Existing prophylactic LMWH or aspirin | -3 | Protective |
| Existing therapeutic LMWH or warfarin | -4 | Protective |
| THRESHOLD: ≤3 pts → LOW RISK → Aspirin 81–325 mg daily | ||
| THRESHOLD: ≥4 pts → HIGH RISK → LMWH or DOAC or warfarin | ||
SAVED Score
| Variable | Points | Category |
| Surgery within 90 days | +2 | |
| VTE history | +3 | |
| Age ≥80 years | +1 | |
| Dexamethasone standard dose (120–160 mg/cycle) | +1 | |
| Dexamethasone high dose (>160 mg/cycle) | +2 | |
| Asian race | -3 | Protective |
| THRESHOLD: <2 pts → LOW RISK → Aspirin 81–325 mg daily | ||
| THRESHOLD: ≥2 pts → HIGH RISK → LMWH or DOAC or warfarin | ||
15B. VTE Prophylaxis Recommendations
| Risk Level | Prophylaxis Options | Duration |
| LOW RISK (≤3 IMPEDE or <2 SAVED) | Aspirin 81–325 mg once daily | Indefinite while on myeloma therapy |
| HIGH RISK (≥4 IMPEDE or ≥2 SAVED) | LMWH (enoxaparin 40 mg SC daily) OR Rivaroxaban 10 mg daily OR Apixaban 2.5 mg BID OR Fondaparinux 2.5 mg daily OR Warfarin (INR 2–3) | 3–6 months then aspirin (longer if persistent risk factors) OR indefinite while on IMiD |
Key VTE Principles
- Highest VTE risk in FIRST 6 MONTHS after new MM diagnosis
- For any patient developing VTE on IMiD-based therapy → continue therapeutic-dose anticoagulation for AS LONG AS IMiD therapy is indicated
- Full-dose anticoagulation CONTRAINDICATED with platelets <50,000/µL; prophylactic may be appropriate if platelets as low as 25,000/µL in high-VTE-risk patients
- Patients already on therapeutic anticoagulation for other reasons (e.g., AFib) → CONTINUE current anticoagulation
- Carfilzomib + IMiD combination → higher VTE risk; consider DOAC or LMWH over aspirin
💎 Pearl: Warfarin at INR 2–3 is NOT directly comparable to DOAC or LMWH at prophylactic doses with respect to bleeding and thrombotic risks. Prefer DOACs or LMWH where possible.
16. CRITICAL PHARMACIST WATCHOUTS
16A. REMS Programs — MANDATORY Enrollment
| Drug | REMS Name | Key Requirement |
| Lenalidomide (Revlimid) | RevASSIST | Mandatory contraception (2 methods); monthly pregnancy test; dispensed ≤28-day supply; males also enrolled |
| Pomalidomide (Pomalyst) | Pomalidomide REMS | Same as lenalidomide — mandatory contraception and pregnancy testing |
| Thalidomide (Thalomid) | THALOMID REMS (S.T.E.P.S.) | STRONGEST teratogen — mandatory contraception; dispensed ≤28 days; no blood/sperm donation |
| Belantamab mafodotin (Blenrep) | BLENREP REMS | Eye exam (slit-lamp) REQUIRED before each dose; patients wear hydrating eye drops; prescribers certified; dispensed to certified healthcare facilities only |
| Cilta-cel (CARVYKTI) | CARVYKTI REMS | Only certified treatment facilities; patient wallet card; monitor for CRS, ICANS; secondary T-cell malignancy |
| Ide-cel (ABECMA) | ABECMA REMS | Only certified treatment facilities; monitor for CRS, ICANS; secondary T-cell malignancy |
16B. Drug-Drug Interactions of Note
| Drug | Interaction | Clinical Action |
| Lenalidomide/Pomalidomide | AVOID combined with strong CYP1A2 inhibitors (e.g., fluvoxamine) | Increased IMiD exposure |
| Ixazomib (Ninlaro) | Avoid strong CYP3A4 inducers (rifampin, carbamazepine, phenytoin) | Significantly reduces ixazomib exposure; loss of efficacy |
| Venetoclax | Strong CYP3A4 inhibitors (azoles, clarithromycin): increase venetoclax levels; CYP3A4 inducers: decrease levels | Dose reduce if unavoidable CYP3A4 inhibitor; avoid grapefruit; follow ramp-up protocol to minimize TLS |
| Dexamethasone + CYP3A substrates | Dexamethasone is a moderate CYP3A4 inducer | May reduce exposure of CYP3A4 substrates (e.g., some statins, certain antifungals) |
| Selinexor | Inhibits XPO1 — affects nuclear export of many proteins; serotonergic risk | Avoid coadministration with serotonergic agents if possible; monitor closely |
| Daratumumab / Isatuximab | Interfere with blood bank testing | Type & screen BEFORE starting; notify blood bank; inform patient |
| Any IMiD + ESA | Synergistic VTE risk | Aggressive VTE prophylaxis mandatory; prefer therapeutic anticoagulation |
| Bortezomib + green tea extract (EGCG) | EGCG inhibits bortezomib activity in vitro | Counsel patients to AVOID green tea supplements while on bortezomib |
16C. Common Adverse Effects Management
| AE | Causative Agent(s) | Management |
| Peripheral neuropathy | Bortezomib (most), thalidomide | Switch IV → SC bortezomib; dose reduce per grade; neurontin or duloxetine for symptomatic relief |
| Infusion reactions | Daratumumab, isatuximab, elotuzumab | Pre-medicate: dexamethasone + antihistamine + acetaminophen; slow infusion rate; have epinephrine available |
| CRS | CAR-T, bispecific antibodies | Grade 1: antipyretics/fluids; Grade 2–3: tocilizumab 8 mg/kg IV; Grade 4: dexamethasone + tocilizumab; ensure stepwise dosing for BsAbs |
| Cytopenia | All myeloma therapies | Monitor CBC; dose hold/reduction per protocol; G-CSF per NCCN guidelines for hematopoietic growth factors |
| Hyperglycemia | Dexamethasone | Insulin management; counsel on glucose monitoring; reduce/eliminate dex dose when possible |
| ONJ (Osteonecrosis of jaw) | Bisphosphonates, denosumab | Dental exam BEFORE therapy; avoid invasive dental procedures while on therapy; report jaw pain |
| Hypocalcemia | Denosumab | Supplement calcium + vitamin D; severe in renal impairment (CrCl <30 mL/min); monitor ionized calcium |
| Skin/nail changes, dysgeusia | Talquetamab (GPRC5D-targeted) | Unique to GPRC5D target; moisturizers for skin; dietary counseling for taste changes; supportive care |
| Keratopathy/Corneal changes | Belantamab mafodotin | Mandatory eye exams (slit-lamp) before EVERY dose; dose hold/reduce based on grade; lubricating eye drops |
| TLS | Venetoclax | Ramp-up dosing per protocol; hydration; uric acid monitoring; allopurinol prophylaxis; avoid in high-burden disease without adequate monitoring |
| Secondary malignancies | Lenalidomide maintenance post-HCT | Discuss risk/benefit with patient; increased risk of hematologic secondary cancers; balance against PFS benefit |
17. DRUG CLASS REFERENCE TABLE — MM THERAPEUTICS
| Drug (Brand) | Class/MOA | Clinical Pearls / Key Side Effects / Counseling |
| Bortezomib (Velcade) | PI — reversible 26S proteasome inhibitor → accumulation of misfolded proteins → apoptosis | SC preferred (less neuropathy); weekly preferred; give herpes prophylaxis; monitor CBC, LFTs; hold if Grade ≥2 PN; green tea/EGCG supplements inhibit activity |
| Carfilzomib (Kyprolis) | PI — IRREVERSIBLE proteasome inhibitor; more selective for β5 subunit | Cycle 1 Day 1 ramp-up to 20 mg/m²; monitor BP each visit; cardiac, pulmonary, renal toxicity; hold for acute kidney injury; hydrate before infusion |
| Ixazomib (Ninlaro) | PI — oral, reversible; first oral PI | Take on empty stomach (≥1h before or 2h after food); GI toxicity common; peripheral neuropathy; avoid strong CYP3A4 inducers; logistical convenience |
| Lenalidomide (Revlimid) | IMiD — targets cereblon E3 ubiquitin ligase → degrades Ikaros/Aiolos → anti-myeloma + immunomodulatory | REMS mandatory; renal dose-adjust REQUIRED; VTE prophylaxis MANDATORY; secondary malignancy risk; embryo-fetal toxicity; monitor CBC, SCr, LFTs; 28-day supply max |
| Pomalidomide (Pomalyst) | IMiD (3rd gen) — more potent cereblon modulator than lenalidomide | REMS mandatory; NO renal adjustment needed; VTE prophylaxis; myelosuppression; used in lenalidomide-refractory patients |
| Thalidomide (Thalomid) | IMiD (1st gen) — anti-angiogenic, immunomodulatory | MOST teratogenic — S.T.E.P.S. REMS; profound sedation (take at night); constipation; DVT; peripheral neuropathy; no longer commonly used as primary therapy |
| Daratumumab (Darzalex / Darzalex Faspro) | Anti-CD38 IgG1κ mAb → CDC, ADCC, ADCP, T-cell activation | Pre-medicate (dex+antihistamine+APAP); type & screen BEFORE use; false+ indirect Coombs; SC formulation (1800 mg flat) preferred for convenience; VZV prophylaxis; IVIG for hypogammaglobulinemia; false+ IFE (IgG kappa myeloma) |
| Isatuximab-irfc (Sarclisa) | Anti-CD38 IgG1κ mAb — different epitope than daratumumab; ADCC, CDC, direct apoptosis | Pre-medicate similarly to daratumumab; type & screen BEFORE use; false+ indirect Coombs; different dosing schedule (Cycle 1: QW × 4 doses; cycles 2+: Q2W) |
| Elotuzumab (Empliciti) | Anti-SLAMF7 mAb → NK cell-mediated ADCC; co-stimulatory T-cell activation | Pre-medicate (dex+antihistamine+H2 blocker+APAP); does NOT interfere with SPEP or immunofixation (important!); lymphopenia; rarely used as first-line |
| Teclistamab (Tecvayli) | BsAb BCMA × CD3 — redirects T cells to kill BCMA+ myeloma cells | Step-up dosing (hospitalization); CRS 72% (mostly G1–2); ICANS; severe infections; levofloxacin + PJP + VZV prophylaxis; consider tocilizumab pre-dose 1 |
| Elranatamab (Elrexfio) | BsAb BCMA × CD3 | Step-up dosing; CRS; infections; ICANS; similar management to teclistamab |
| Talquetamab (Talvey) | BsAb GPRC5D × CD3 — UNIQUE non-BCMA target | CRS; unique: skin/nail toxicity, dysgeusia, weight loss (GPRC5D expressed on skin/hair/taste); may use as bridge to BCMA CAR-T (v5.2026 footnote) |
| Linvoseltamab (Lynozyfic) | BsAb BCMA × CD3 | NEW in v2.2026; step-up dosing; CRS; infections; cytopenia; 200 mg SC QW then Q4W if ≥VGPR |
| Cilta-cel (CARVYKTI) | BCMA-directed CAR T-cell therapy — autologous; dual BCMA-binding domains | REMS; leukapheresis → 4–6 wk manufacturing; lymphodepleting chemo (fludarabine/cyclophosphamide) before infusion; CRS; ICANS; delayed neurotoxicity (Parkinsonism described); prolonged cytopenias; 100-day monitoring |
| Ide-cel (ABECMA) | BCMA-directed CAR T-cell therapy — autologous; single-domain BCMA antibody | REMS; CRS; ICANS; secondary T-cell malignancy (boxed warning); prolonged cytopenias; 100-day monitoring |
| Selinexor (Xpovio) | XPO1 inhibitor → prevents nuclear export of tumor suppressor proteins → nuclear retention → apoptosis | N/V/anorexia (antiemetic prophylaxis mandatory — ondansetron or olanzapine); weight loss; hyponatremia (monitor Na⁺); thrombocytopenia; fatigue; take with food |
| Venetoclax (Venclexta) | BCL-2 inhibitor → restores apoptosis in BCL-2-dependent cells | ONLY for t(11;14) patients in MM; TLS risk → ramp-up protocol mandatory; avoid strong CYP3A4 inhibitors; no data in MM outside t(11;14); check for azole antifungal interactions |
| Belantamab mafodotin (Blenrep) | ADC: anti-BCMA mAb conjugated to MMAF (auristatin microtubule inhibitor) | BLENREP REMS; mandatory slit-lamp eye exam before EVERY dose; lubricating eye drops; grade-based dose modification for keratopathy; thrombocytopenia; nausea; corneal toxicity most limiting |
| Zoledronic acid (Zometa) | Bisphosphonate — inhibits osteoclast activity (farnesyl pyrophosphate synthase) | Infuse over ≥15 min (renal toxicity with rapid infusion); renal monitoring; dental exam before; ONJ risk; hold if CrCl <30; flu-like symptoms (1st dose); supplement Ca + Vit D |
| Denosumab (Xgeva) | RANK-L inhibitor → prevents osteoclast formation | SC injection Q4 weeks; PREFERRED in renal impairment; severe hypocalcemia risk (supplement Ca + Vit D always); rebound hypercalcemia/vertebral fractures if discontinued → give bisphosphonate or maintenance Q6 months |
| Pamidronate (Aredia) | Bisphosphonate — less potent than zoledronic acid | IV over ≥2 hours; focal segmental glomerulosclerosis risk (avoid in nephrotic range proteinuria); dental exam before; supplement Ca + Vit D; osteonecrosis of jaw |
18. CLINICAL PEARLS SUMMARY — RAPID REVIEW
| Clinical Pearl |
| SC bortezomib is preferred over IV — significantly less peripheral neuropathy (MMY-3021 trial) with non-inferior efficacy. |
| Weekly bortezomib dosing is preferred over twice-weekly — similar ORR and VGPR, but fewer grade 3/4 AEs. |
| Quadruplet regimens (Dara-VRd, Isa-VRd) are preferred for ALL newly diagnosed MM — both HCT-eligible and ineligible. |
| TYPE AND SCREEN must be done BEFORE starting daratumumab or isatuximab — they cause false-positive indirect Coombs test. |
| Lenalidomide requires mandatory REMS (RevASSIST) and RENAL DOSE ADJUSTMENT using Cockcroft-Gault CrCl. |
| For IgG myeloma patients: estimate NORMAL IgG by subtracting M-spike from total IgG. Consider IVIG if corrected IgG <400 mg/dL. |
| Daratumumab/isatuximab can produce FALSE-POSITIVE M-spike on immunofixation in IgG kappa patients. Use mass spectrometry to differentiate. |
| Denosumab is PREFERRED bone-targeting agent in renal impairment but requires calcium + vitamin D supplementation and close calcium monitoring. |
| Zoledronic acid is NOT recommended when CrCl <30 mL/min — switch to denosumab. |
| If denosumab is discontinued, give bisphosphonate or Q6-month maintenance denosumab to prevent rebound osteoporosis and vertebral fractures. |
| VTE prophylaxis is MANDATORY with IMiD-based therapy. Use IMPEDE or SAVED score; aspirin for low risk, DOAC/LMWH for high risk. |
| Carfilzomib ramp-up is REQUIRED: Cycle 1 Day 1 = 20 mg/m² only (regardless of target dose). Monitor BP before EVERY infusion. |
| Venetoclax has activity in MM ONLY for t(11;14) patients. Do not use in non-t(11;14) outside of a clinical trial. |
| Belantamab mafodotin (Blenrep) requires MANDATORY eye exam (slit-lamp) before EVERY dose — REMS requirement. No exceptions. |
| BsAbs (teclistamab, elranatamab, talquetamab, linvoseltamab) require STEP-UP DOSING to reduce CRS risk. Hospitalization for monitoring during step-up. |
| Talquetamab targets GPRC5D (not BCMA) — unique AEs include skin/nail toxicity and dysgeusia (taste changes). Can be used as bridge to BCMA CAR-T. |
| Alkylating agents (bendamustine, cyclophosphamide) CAN IMPAIR T-cell collection for CAR-T — plan treatment sequence carefully in potential CAR-T candidates. |
| Smoldering MM: high-risk (≥2 of: BMPCs >20%, M-protein >2 g/dL, FLCr >20) → clinical trial preferred; daratumumab (cat 1) is now a treatment option. |
| Duffy-null phenotype in Black/African Americans → lower baseline ANC but physiologically insignificant. Do NOT use rigid reference ranges for dose adjustments. |
| For dex dose reduction: reduce to 20 mg/week in older/frail patients; discontinue at earliest possible timepoint once response achieved or toxicity present. |
| Stem cell harvest should be done within first 6 treatment cycles BEFORE prolonged lenalidomide or daratumumab exposure — limits future HCT eligibility. |
| Two-drug maintenance is recommended for HIGH-RISK MM (e.g., dara + lenalidomide, or bortezomib + lenalidomide). |
| PJP prophylaxis required for CAR-T and BsAb patients: TMP-SMX (or alternatives) from therapy start, continuing ≥6 months post-infusion OR until CD4 ≥200/mm³. |
| VZV prophylaxis indefinite for BsAb patients and ≥12 months (preferably indefinite) for CAR-T patients — regardless of vaccination status. |
| CAR-T ide-cel (Abecma) has boxed warning for SECONDARY T-CELL MALIGNANCIES. Counsel patients and monitor long-term. |
19. MANAGEMENT OF RENAL DISEASE IN MM (MYEL-L)
Renal disease defined as serum creatinine >2 mg/dL OR eGFR <60 mL/min/1.73 m².
Workup
- Serum creatinine, electrolytes, uric acid
- Urinalysis with sediment and electrolytes
- 24-hour urine collection for total protein, UPEP, UIFE
- SPEP/SIFE and serum FLCs
- Consider renal ultrasound and renal biopsy
- Consider other diagnoses: amyloid, light chain deposition disease for patients with significant proteinuria
Treatment Approach
- Pulse dexamethasone (rapid effect)
- Regimens containing BORTEZOMIB and/or DARATUMUMAB preferred (rapidly reduce light chain burden)
- Can switch to other regimen once renal function has improved or stabilized
- Goal urine output: 100–150 cc/h (hydration to dilute tubular light chains)
- Monitor fluid status; treat hypercalcemia, hyperuricemia, other metabolic abnormalities
- Discontinue ALL nephrotoxic medications (NSAIDs, aminoglycosides, contrast agents)
- Dialysis for: refractory electrolyte disturbances, uremia, fluid overload
💎 Pearl: Renal dysfunction and advanced age are NOT contraindications to autologous HCT. Systemic therapy should NOT be delayed to perform plasmapheresis or high cutoff dialysis.
⚠ Lenalidomide is renally cleared — MUST adjust dose per CrCl. Pomalidomide does NOT require renal dose adjustment (key differentiator from lenalidomide).
20. CNS MYELOMA — CNSM-1 (NEW IN V1.2026)
Clinical Presentation
- Confusion, headache, visual symptoms, weakness, cranial nerve palsies
- Hyperammonemic encephalopathy is RARE and NOT considered CNS involvement (resolves with systemic therapy)
- Hyperviscosity and hypercalcemia can cause neurologic symptoms but NOT CNS involvement
Diagnosis
- Brain and spine MRI with and without contrast
- Lumbar puncture: flow cytometry, cytopathology, cell count, total protein
- CSF SPEP is NOT appropriate for CNS diagnosis in MM
- Definitive: clonal plasma cells in CSF by immunophenotyping OR tissue diagnosis in affected CNS tissue
- Probable: leptomeningeal enhancement or parenchymal lesions on MRI without definitive clonal plasma cells
Management (MYEL-H)
- Multimodality therapy — radiation + systemic therapy
- Intrathecal chemotherapy: Thiotepa/Hydrocortisone OR Methotrexate/Cytarabine/Hydrocortisone
- Do NOT give concurrent IT methotrexate and radiation — space ≥2 weeks apart (myelopathy risk)
- Novel agents with CNS penetration: pomalidomide, lenalidomide (some BBB penetration observed clinically)
- Venetoclax: preclinical BBB penetration data; consider for t(11;14) if no other options
- CAR-T and BsAbs: prior CNS disease does NOT preclude use; limited data on CNS penetration
- Proteasome inhibitors: LIMITED CNS penetration; no clear signal for activity in CNS disease
- Palliative care integration strongly recommended
21. QUICK REFERENCE ALGORITHM & CHECKLIST
At Diagnosis — Pharmacist Checklist
| ✓ | Action Item |
| ☐ | Confirm diagnosis: BMPCs%, M-protein, CRAB/SLiM criteria reviewed |
| ☐ | Staging: ISS, R-ISS, R2-ISS calculated; LDH and beta-2 microglobulin obtained |
| ☐ | Cytogenetics FISH panel reviewed: del(17p), t(4;14), t(11;14), t(14;16), 1q21, del(1p32), TP53 by NGS |
| ☐ | HCT eligibility assessed: age, PS, organ function |
| ☐ | Renal function: CrCl calculated (Cockcroft-Gault); lenalidomide dose adjusted if needed |
| ☐ | Type and screen ordered BEFORE daratumumab or isatuximab |
| ☐ | VTE risk stratified (IMPEDE or SAVED); prophylaxis ordered |
| ☐ | VZV prophylaxis ordered (acyclovir or valacyclovir) |
| ☐ | Bone-targeting therapy initiated (zoledronic acid or denosumab) |
| ☐ | Calcium and vitamin D supplementation ordered |
| ☐ | Dental exam recommended before bisphosphonate/denosumab |
| ☐ | Hepatitis B, hepatitis C, HIV screening done (before immunotherapy/chemotherapy) |
| ☐ | REMS program enrollment confirmed (lenalidomide/pomalidomide/thalidomide/belantamab/CAR-T) |
| ☐ | NT-proBNP/BNP reviewed (amyloid workup if elevated) |
| ☐ | MRD clonotype baseline obtained or stored for future MRD testing |
At Each Clinic Visit — Ongoing Monitoring
| ✓ | Monitoring Parameter |
| ☐ | CBC with differential — neutropenia, thrombocytopenia, anemia |
| ☐ | Comprehensive metabolic panel — SCr, LFTs, Ca, albumin |
| ☐ | SPEP + SIFE and serum FLC assay — disease response assessment |
| ☐ | 24-h urine total protein/UPEP/UIFE (as clinically indicated) |
| ☐ | Blood pressure before each carfilzomib infusion |
| ☐ | Assessment for peripheral neuropathy (bortezomib, thalidomide) |
| ☐ | Glucose monitoring if on dexamethasone |
| ☐ | VTE symptoms; anticoagulation adherence and INR (if warfarin) |
| ☐ | ONJ screening (jaw pain, exposed bone) if on bisphosphonate/denosumab |
| ☐ | Eye exam (slit-lamp) before each dose of belantamab mafodotin |
| ☐ | CRS and ICANS signs for bispecific antibody and CAR-T patients |
| ☐ | Infection symptoms; review prophylaxis adherence |
| ☐ | Medication reconciliation — drug interactions, OTC supplements |
NCCN Guidelines Version 5.2026 — Multiple Myeloma — January 9, 2026 | For educational use only